Men's Health
·16 min read
The Great Male Decline
Why Testosterone Has Fallen for Decades — and What the Data Actually Says You Can Do About It
By Tony Medrano, CEO & Founder, LongevityPlan.AI
Here is an uncomfortable fact that has nothing to do with how many push-ups you can do. The average middle-aged American man today walks around with measurably less testosterone than a man of the same age did a generation ago. Not because he is older — because of when he was born. In 2007, epidemiologist Thomas G. Travison and colleagues at the New England Research Institute published a study that put this on the map: tracking men in the Massachusetts Male Aging Study from roughly 1987–2004, they found a decline of more than 1% per year in men's testosterone that was independent of age. A 60-year-old measured in the late 1980s, on average, had higher testosterone than a different 60-year-old measured fifteen years later. Same age. Different decade. Lower hormone.
What makes the finding so durable — and so useful for anyone serious about their healthspan — is the part most headlines skipped. The decline was not explained by the obvious culprit. As Travison's team put it, the drop was "not explained fully by the usual suspects: increasing BMI and prevalence of obesity."
In other words: yes, men got heavier, and that matters enormously (we will get to the fat). But subtract obesity, and you are still left with a population-wide downshift that points to something in the shared environment — and to the way each individual body is built to respond to it.
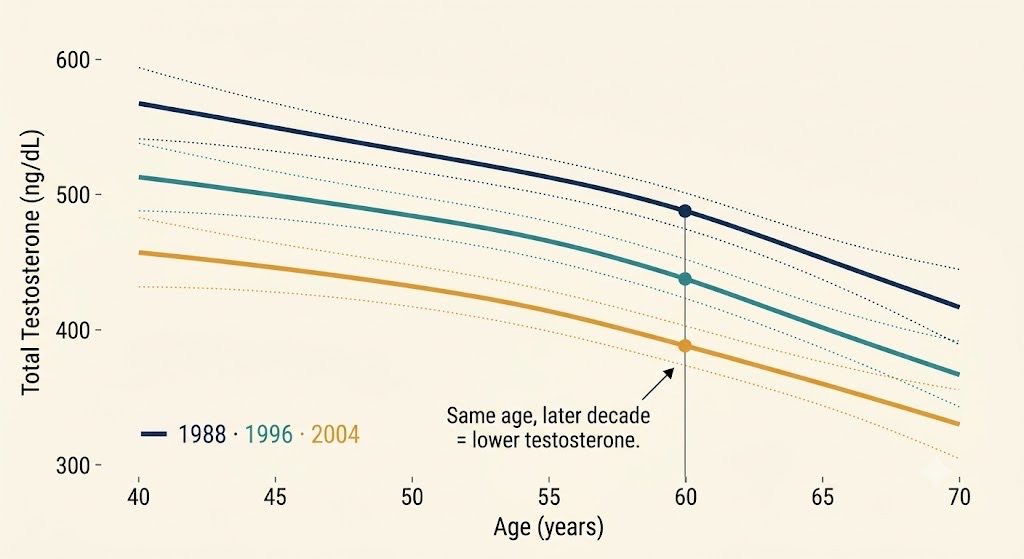
A man's birth year now predicts his testosterone nearly as much as his age. In the Massachusetts Male Aging Study, men of the same age measured in later decades had lower testosterone — an age-independent, population-wide decline of more than 1% per year.
This article is a field guide to the three biggest forces implicated in the male testosterone slide — endocrine-disrupting chemicals, fatherhood, and obesity — and to the precision-medicine reason the same three forces produce wildly different results in different men. The thesis is simple and not especially flattering to the wellness industry: population averages tell you the weather; only your own data tells you the climate you personally live in. The men who age best in the next twenty years will be the ones who stop guessing.
First, a confession the lab won't make: your "low T" might be your assay's fault
Before we assign blame to plastics or parenting, a precision-medicine reality check that almost no consumer article mentions. For years, the number printed on a man's testosterone result depended heavily on which laboratory ran it. In 2017, Travison led a second landmark paper — 9,054 men pooled from four large cohorts, including the Framingham Heart Study and the European Male Aging Study, all re-measured against a single reference method at the U.S. Centers for Disease Control and Prevention. The harmonized normal range for a healthy, non-obese man aged 19–39 came out to 264–916 ng/dL. The kicker buried in the methods: a substantial share of the disagreement between cohorts was due not to biology but to differences in how the assays were calibrated.
Hubert Vesper of the CDC, a co-author and co-chair of the Partnership for the Accurate Testing of Hormones, did not mince words: "Without harmonized reference ranges and standardized assays, tests can lead to misdiagnoses."
Major reference laboratories took the point seriously — Labcorp, for instance, revised its adult-male reference interval to align with the 264–916 ng/dL standard, and the broader effort to anchor hormone assays to a CDC reference method now shapes how Quest Diagnostics and reference-grade platforms from Thermo Fisher Scientific (the LC-MS/MS mass spectrometry that serious endocrinology runs on) report results.
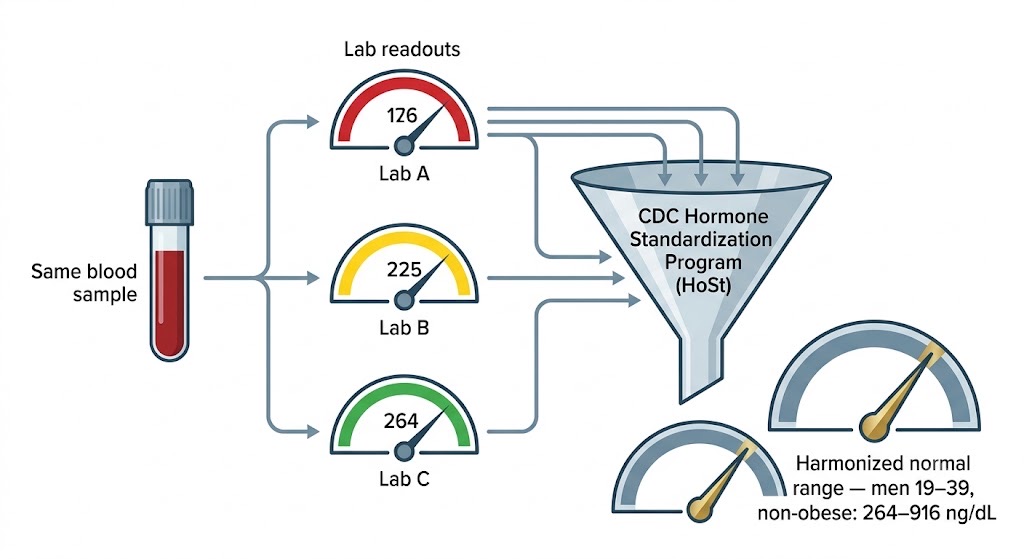
Same blood, three answers. Until assays are calibrated to a single CDC reference method, "low T" can be an artifact of the lab. The harmonized adult-male reference range is 264–916 ng/dL.
Why open with plumbing? Because it is the whole argument in miniature. A man who is told he is "normal" by a poorly standardized immunoassay, and a man told he is "low" by a stricter one, may have identical blood. Multi-modal health data beats a single number measured once on an unknown instrument. If you take nothing else from this piece: when you measure testosterone, measure it in the morning, fasted, on a standardized assay, more than once — and read it alongside SHBG, LH, FSH, and estradiol, not in isolation. That is not biohacking. That is just doing the test correctly.
Force One: the chemicals that were never tested for this
The term "endocrine disruptor" was coined at a 1991 scientific meeting at the Wingspread conference center, convened by the late zoologist Theo Colborn — who went on to found The Endocrine Disruption Exchange (TEDX) and co-author Our Stolen Future, the book that dragged this field into public view. TEDX's working list of chemicals with evidence of endocrine activity runs to roughly a thousand compounds. They share an inconvenient property: they were designed to make plastics flexible, furniture flame-resistant, and receipts printable — not to be screened against the human hormone system before mass production.
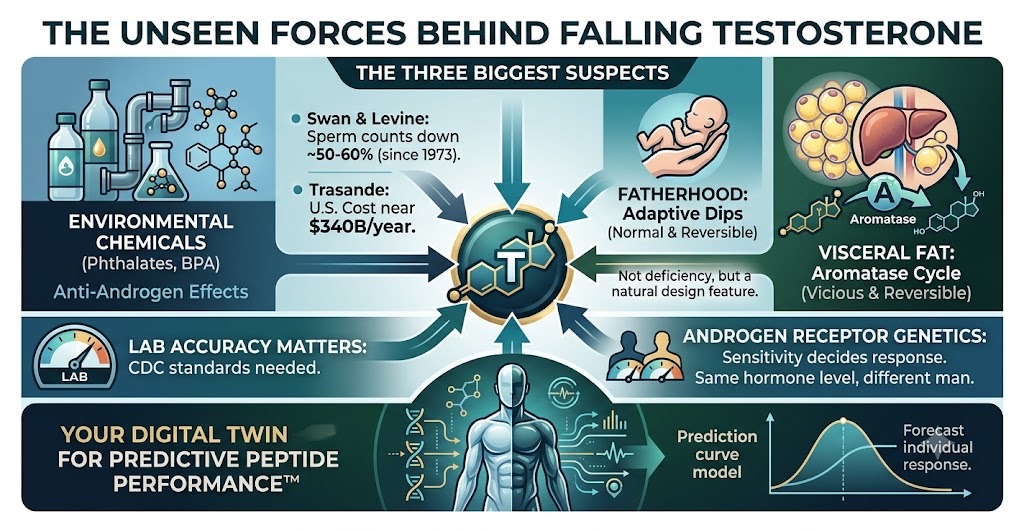
Two classes matter most for male hormones. Phthalates, the plasticizers in soft PVC, fragrances, and food-contact materials, are anti-androgenic — they blunt the action of testosterone during the fetal window when the male reproductive tract is being built. The most striking human evidence comes from Shanna H. Swan of the Icahn School of Medicine at Mount Sinai, whose teams showed that boys whose mothers had higher prenatal phthalate exposure were born with a shorter anogenital distance — a sensitive, validated readout of androgen action in the womb. Bisphenol A (BPA), meanwhile, was the subject of Frederick vom Saal's low-dose work showing hormonal effects at exposures regulators had assumed were safe — part of a body of "low-dose, non-monotonic" science advanced by researchers such as Laura Vandenberg, Ana Soto, and Carlos Sonnenschein that fundamentally challenged the old toxicology axiom that the dose alone makes the poison.
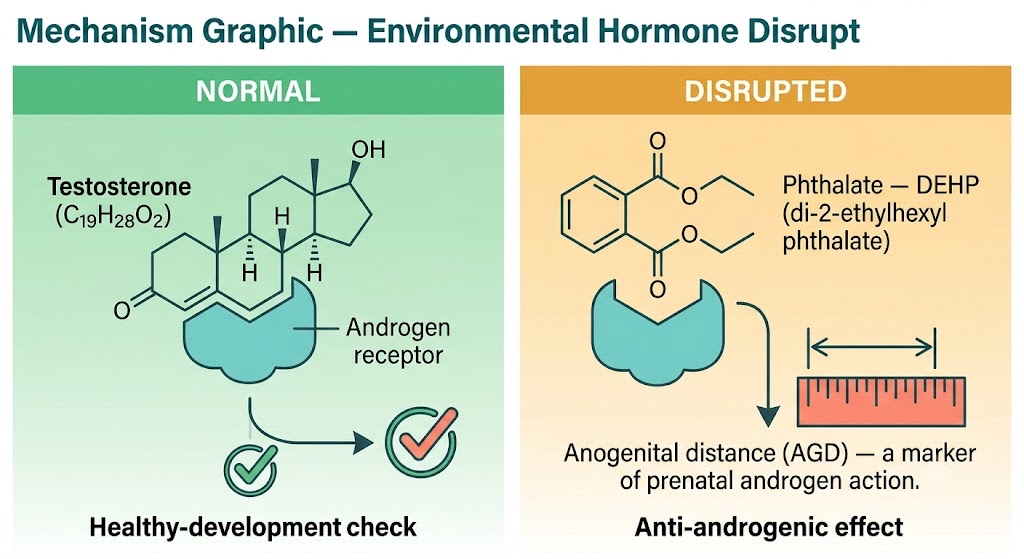
Phthalates are anti-androgens — they blunt testosterone's action during the fetal window. Higher prenatal phthalate exposure tracks with shorter anogenital distance in boys, a validated readout of androgen signaling in the womb.
Reproductive epidemiology has moved in lockstep with chemistry. Hagai Levine of Hebrew University and Swan, building on the testicular-dysgenesis framework of Niels Skakkebæk and Richard Sharpe, published meta-analyses showing sperm concentration in men of North America, Europe, and Australia fell by roughly 52% between 1973 and 2011, with total sperm count down about 59% — and no sign of leveling off. Their 2022 follow-up extended the decline to South and Central America, Asia, and Africa, and reported that the slide has, if anything, accelerated since 2000. Swan's summary of what this means for men's health more broadly was blunt: "This clearly cannot continue unchecked."
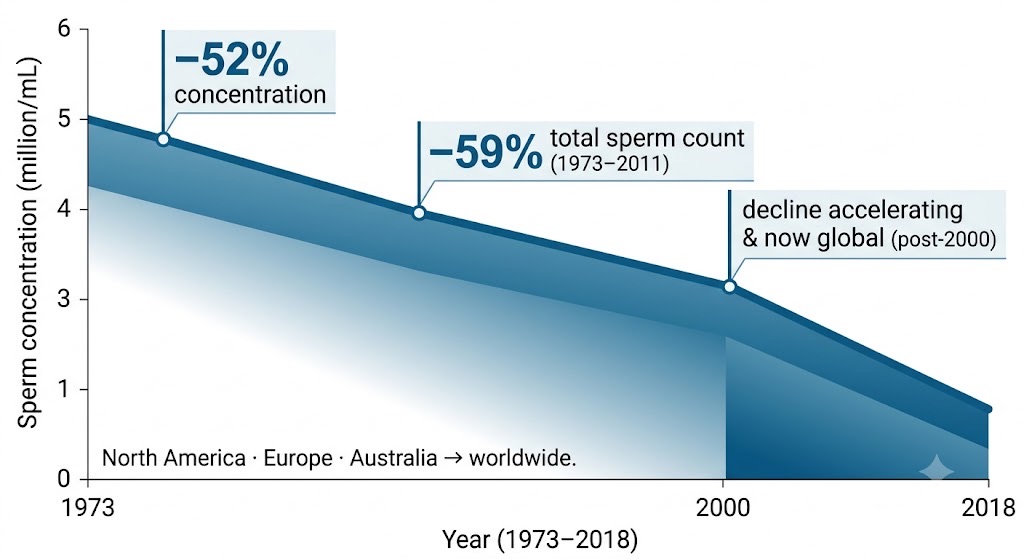
Across five decades, sperm concentration in Western men fell about 52% and total count about 59% — with no sign of leveling off. Subsequent analyses have extended the worldwide decline, and it has accelerated since 2000.
None of this is a reason to panic-buy a hazmat suit, and the honest version of the story includes genuine scientific debate about effect sizes and measurement. It is, however, a reason to treat avoidable exposure as a free lever. The economic framing is what tends to land with executives: Leonardo Trasande of NYU has estimated that endocrine-disrupting chemical exposure costs the United States on the order of $340 billion a year — about 2.3% of GDP — in disease burden and lost productivity, versus roughly $217 billion in the European Union. Trasande's read of his own data: "the tremendous economic as well as human health costs of endocrine-disrupting chemicals."
This is where a generation of newer organizations has quietly built infrastructure that the regulators never did. The Environmental Working Group and the Silent Spring Institute maintain product and exposure databases; the Green Science Policy Institute works upstream on flame-retardant and "forever chemical" policy; the Endocrine Society, whose EDC Scientific Statements were shaped by researchers including Andrea Gore and Jerrold Heindel, translates the mechanism into clinical guidance; and the U.S. National Institute of Environmental Health Sciences — long associated with toxicologist Linda Birnbaum — funds the science that makes any of this measurable. For the individual, the most interesting development is the at-home exposure test. Million Marker, an innovative direct-to-consumer venture, lets you quantify your own urinary phthalate and BPA metabolites — turning "I should probably use less plastic" into an actual before-and-after number. That is the EDC story made personal, which is the only version that changes behavior.
The obesogen wrinkle: chemicals that may also make you fat
One more thread ties Force One directly to Force Three. In 2006, developmental biologist Bruce Blumberg at UC Irvine, with Felix Grün, coined the term obesogen after showing that the organotin compound tributyltin could drive weight gain and fat-cell formation in mice by hijacking the PPARγ and RXRα nuclear receptors that govern fat storage. The hypothesis — advanced by scientists such as Heindel and popularized by metabolic-health communicator Robert Lustig — is that certain environmental chemicals can nudge the body's fat set-point independent of calories. The field is still maturing and not without critics. But it matters here because fat is not a passive bystander in male hormones. Fat is an endocrine organ. Which brings us to the cycle.
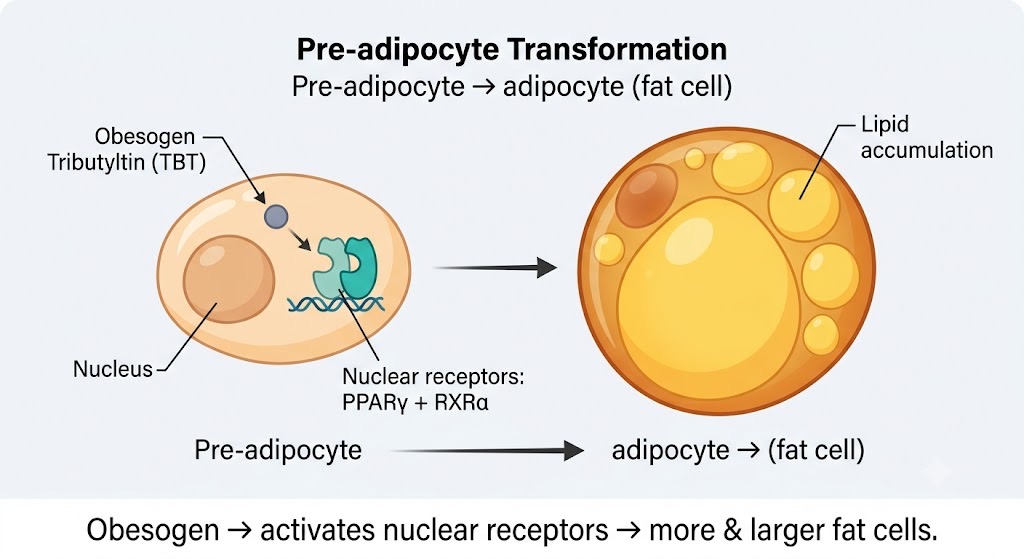
Some chemicals don't just disrupt hormones — they may reprogram fat storage. "Obesogens" like tributyltin flip the PPARγ/RXRα switch that turns precursor cells into fat cells, nudging the body's fat set-point independent of calories.
Force Two: fatherhood — the decline that's supposed to happen
Now for the most misread item on the list. Not every testosterone dip is a malfunction; some are features. In 2011, anthropologists Lee Gettler, Christopher Kuzawa, and Thomas McDade published a uniquely powerful study in PNAS. Using the Cebu Longitudinal Health and Nutrition Survey in the Philippines, they followed 624 young men before they had children and watched what happened next. Two things stood out. First, men who started with higher testosterone were more likely to become partnered fathers — so high T helps you get to the starting line. Second, and more importantly, after becoming fathers, men's testosterone dropped substantially, with the steepest declines in the men most involved in hands-on care of newborns.
This is not pathology. It is the human version of a pattern seen across species in which males help raise young: testosterone is high during mate-seeking and competition, then steps down to make room for caregiving. As Kuzawa framed it, "Human fathers are biologically wired to help with the job." The mechanism is partly reversible; complementary research has examined how testosterone behaves as children grow and as pair bonds change, and the new-father neuroendocrine adaptation is also studied by scientists such as Darby Saxbe and, in the human behavioral-endocrinology tradition, Peter Gray.
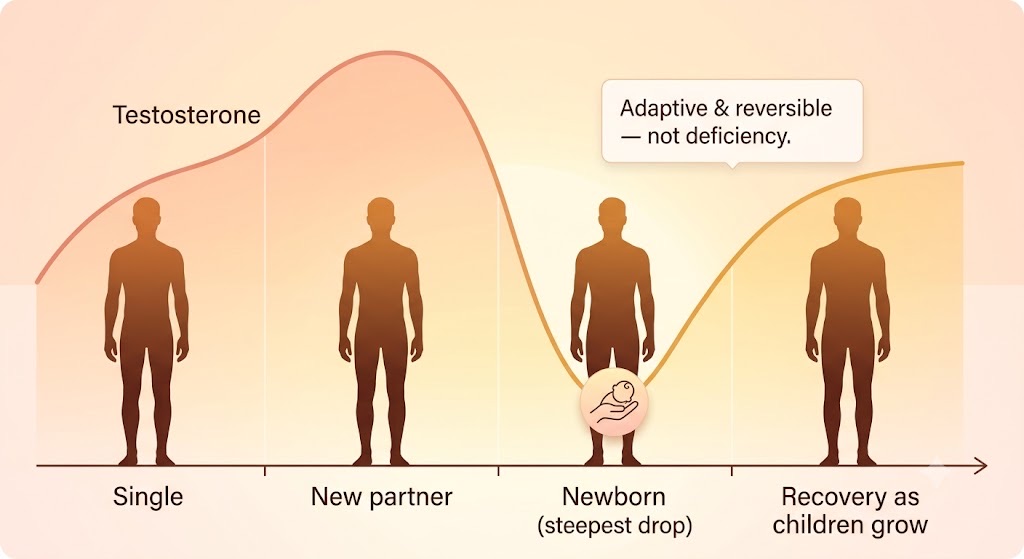
Not every dip is a defect. New fatherhood lowers testosterone by design — most in the most hands-on dads — then tends to recover. Context decides whether a number is a problem.
Why does this belong in a longevity article? Because it is the cleanest possible illustration of the central point: context determines whether a number is a problem. A 38-year-old founder with a six-month-old at home and a testosterone reading 15% below his pre-baby baseline is not necessarily "deficient" — he may be biologically on schedule. A 58-year-old with the same reading, a widening waistline, and rising fasting insulin is telling a different story entirely. Identical lab value; opposite clinical meaning. No algorithm and no clinician can tell them apart without the surrounding data. This is the difference between a number and a narrative — and it is exactly what longevity planning exists to supply.
Force Three: the fat cell that eats your testosterone
Of the three forces, obesity is the most mechanistically airtight, the most personally modifiable, and — good news for the skeptic — the most reversible. Adipose tissue is not inert storage; it is a hormone factory, and one of its products is the enzyme aromatase (gene name CYP19A1), which converts testosterone into estradiol. The more visceral fat a man carries, the more aromatase activity, the more testosterone is siphoned into estrogen. That extra estradiol then feeds back to the brain, suppressing the GnRH and luteinizing-hormone signals that tell the testes to make testosterone in the first place. Less testosterone means easier fat gain; more fat means more aromatase; more aromatase means even less testosterone. Endocrinologists call it the hypogonadal-obesity cycle, and it is a genuine vicious circle.
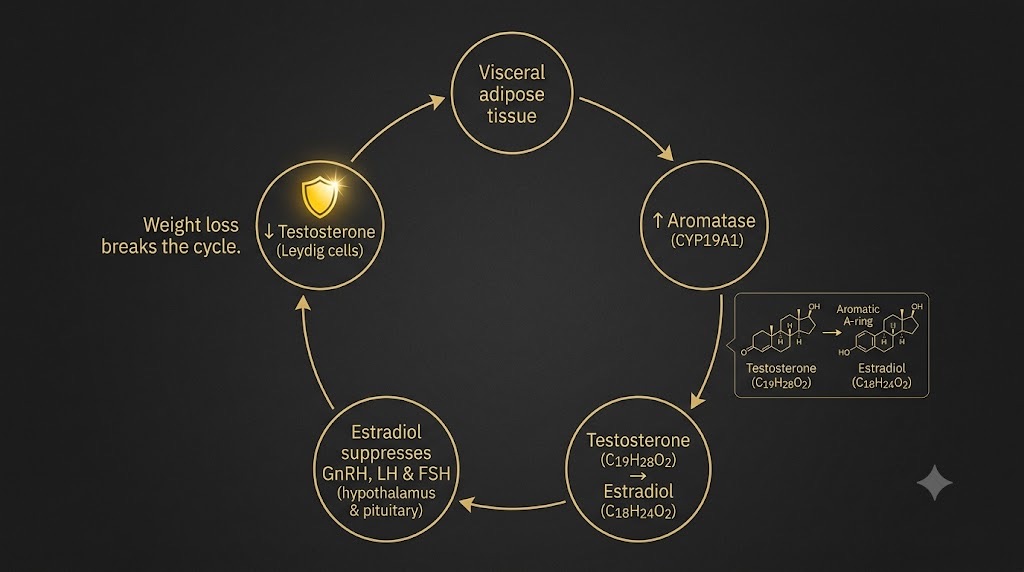
Fat is a hormone organ. Aromatase in adipose tissue converts testosterone into estradiol, which suppresses the brain signals that drive testosterone production — a self-reinforcing loop that losing visceral fat can break.
The numbers are stark. In one frequently cited dataset, the prevalence of secondary hypogonadism among obese men rose from about 7.4% in those with a BMI of 30–35 to roughly 59% in those with a BMI above 50. The flip side is the encouraging part: because the cycle is driven by fat mass, removing fat mass partially reverses it. Sustained weight loss raises endogenous testosterone — and the rapid, substantial weight loss now achievable with GLP-1 medicines such as semaglutide (Novo Nordisk) and tirzepatide (Eli Lilly) has reopened the question of how much of "low T" in heavier men is metabolic rather than gonadal, and therefore fixable without ever touching exogenous hormones. It also reframes the multi-billion-dollar testosterone-gel market — built on products like AbbVie's AndroGel — as, in many men, a treatment for a downstream symptom of a problem that lives in the adipocyte.
The practical lesson is almost old-fashioned: for a large share of men, the single highest-yield testosterone intervention is not a syringe. It is losing visceral fat, sleeping enough to protect the morning testosterone pulse, and lifting heavy things. The reason to measure first is to find out which man you are — the one whose hormones will rebound with weight loss, or the one with a genuine primary problem who needs more.
Why three men with identical labs need three different plans: the genetics layer
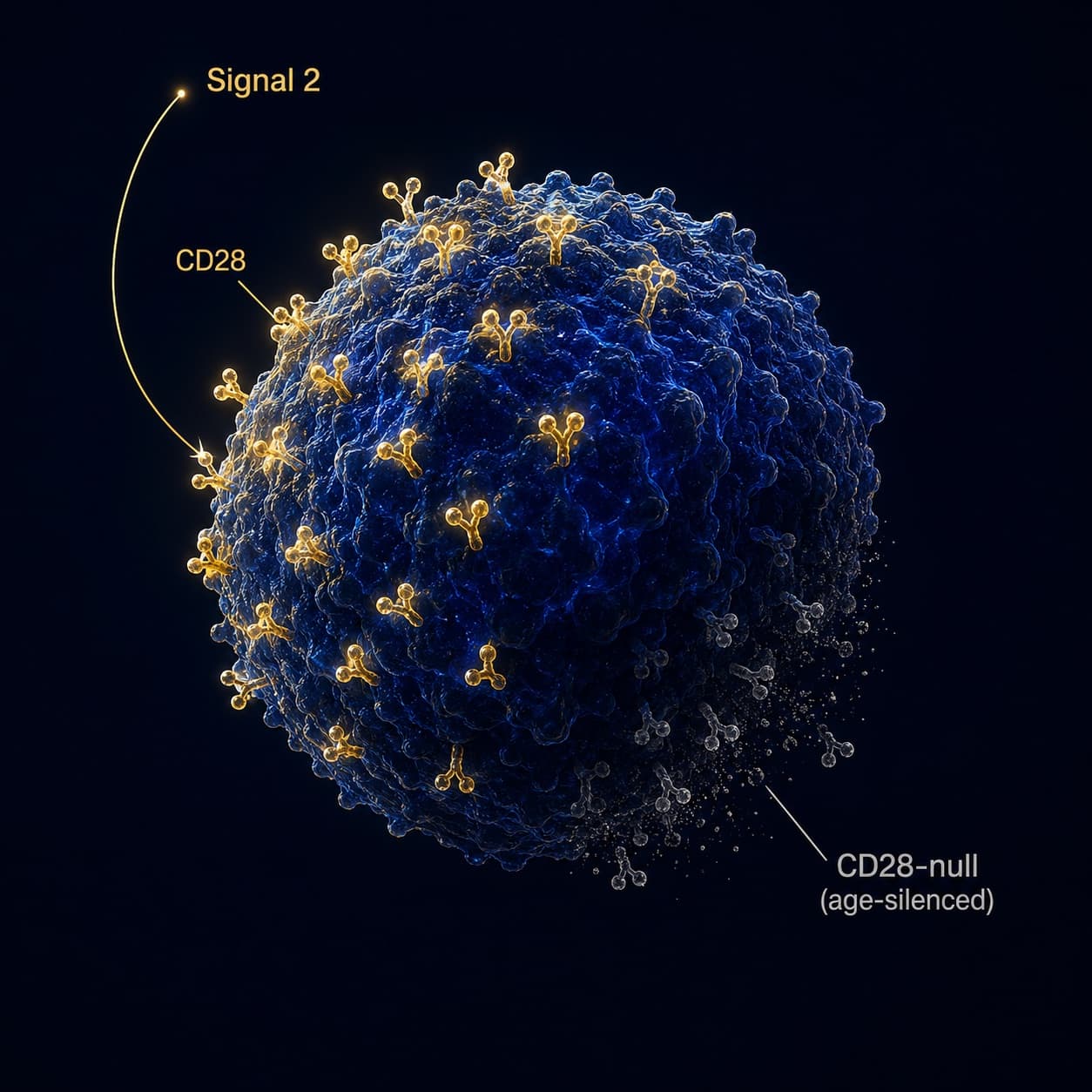
So far, we have three population-level forces. Here is the reason they never land identically on any two individuals — and the scientific foundation of personalized longevity planning. Testosterone is only as useful as your cells' ability to hear it, and that hearing is partly written in your DNA. The androgen receptor gene carries a variable stretch of CAG repeats; the length of that stretch tunes how strongly the receptor responds to a given amount of testosterone. Shorter repeats generally mean a more sensitive receptor — greater androgenic effect per unit hormone — while longer repeats blunt it. Research by Michael Zitzmann and colleagues has even shown that this same polymorphism, together with body weight, modulates how men respond to — and tolerate — testosterone therapy itself.
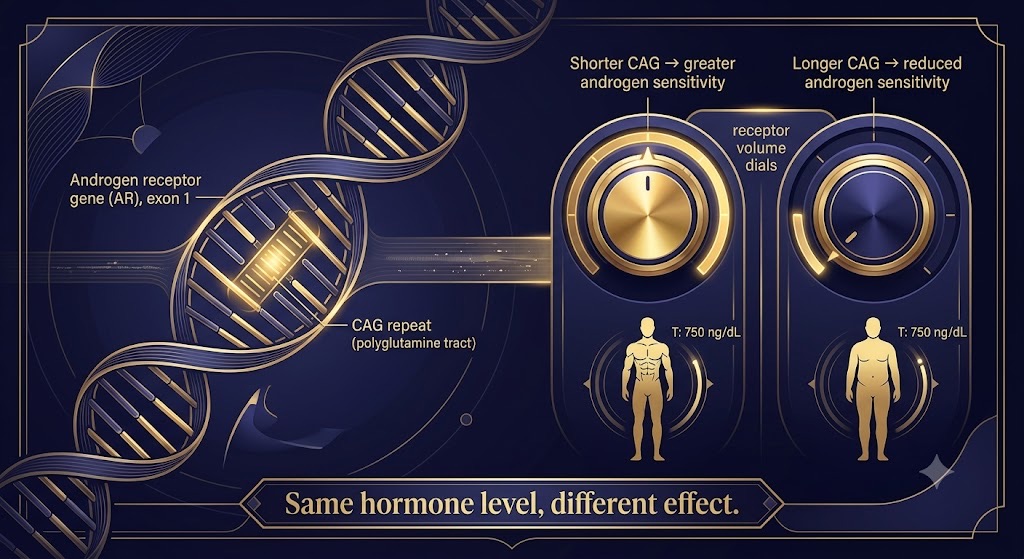
Two men with the same testosterone can live in different bodies. The CAG repeat in the androgen receptor gene tunes how loudly each cell "hears" the hormone — which is why population reference ranges can't personalize a plan.
Translate that from the journal: two men with identical 450 ng/dL readings can live in different bodies. One feels and functions like a man at 600; the other, like a man at 350. Reference ranges built on populations cannot resolve that — only the individual's genome plus phenotype can. This is precisely the gap that functional-genomics services are built to close. The Genomics Company, for example, pairs a clinical-grade DNA test with practitioner interpretation across body systems, including hormones, and its concierge "Genome Itinerary" goes so far as to sequence supplements, dietary patterns, and even Peptide Therapy choices and timing to an individual's genetic cascade. Genetics tells you which detox pathways clear EDCs efficiently, how your nervous system metabolizes stress, and — critically for this audience — how sensitively your tissues read androgens in the first place.
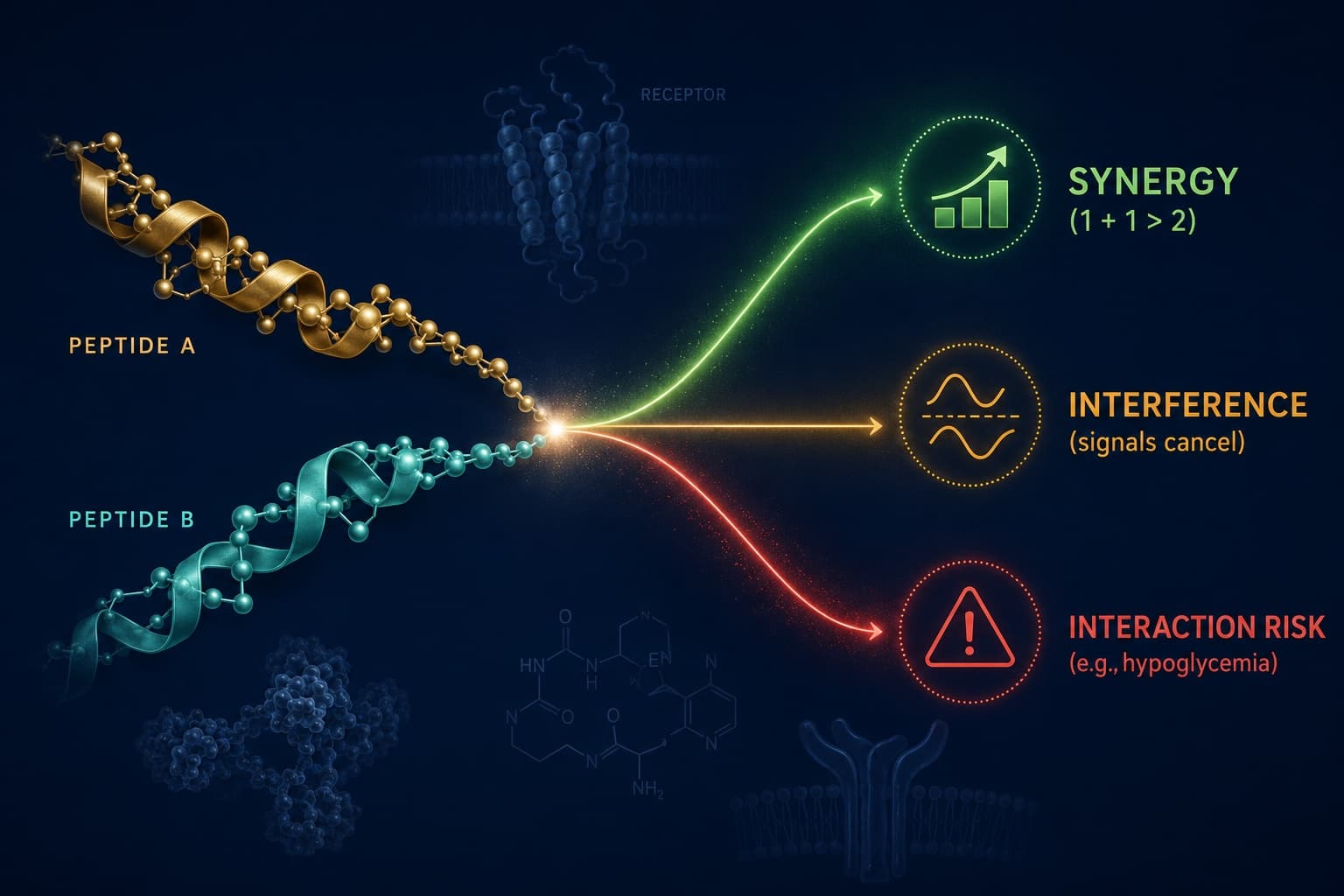
That genetic baseline is the bedrock layer of what we call a Digital Twin for Predictive Peptide Performance™: a personalized model in which your fixed genome (the intelligence layer) is fused with the continuous stream from your wearables, labs, and body-composition scans (the sensor layer) so that predictive modeling can forecast how you specifically will respond to a given protocol — before you spend a year and a small fortune finding out by trial and error. A peptide or hormone protocol that transforms a man with a sensitive androgen receptor and clean clearance pathways may do very little for a man whose genetics route the same molecule straight to the exits. The twin is how you tell those men apart on paper, rather than in hindsight.
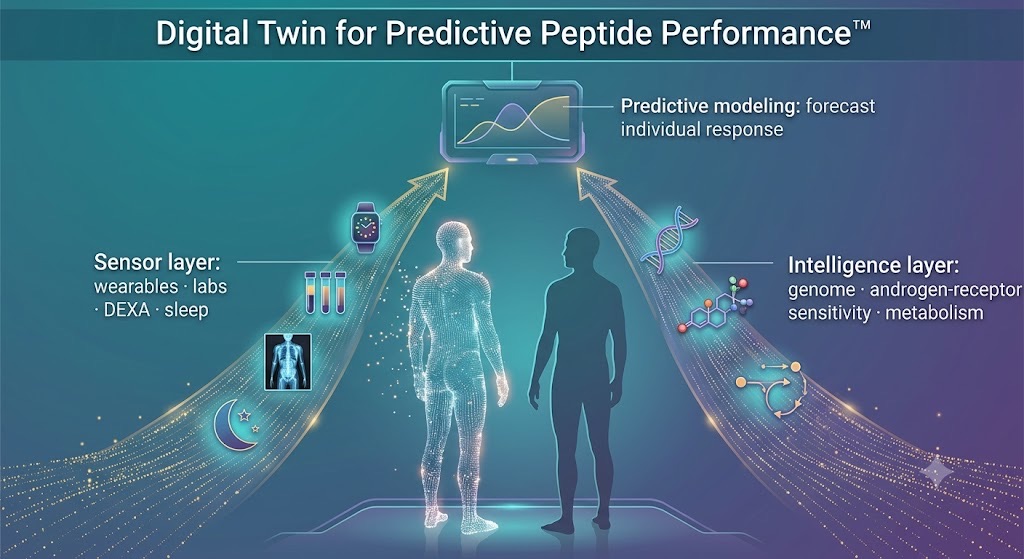
A digital twin fuses your fixed genome (the intelligence layer) with your live data stream (the sensor layer) to predict how you — specifically — will respond to a protocol, before a year of trial and error does it for you.
The buyer's guide: turning four decades of decline into a personal plan
If you are an over-40 executive, a clinician who is tired of one-size-fits-all reference ranges, a returning athlete, or simply someone who intends to be strong at 80, here is the skeptic's version of what the evidence actually supports — stripped of supplement-aisle theater.
1. Measure correctly, then measure again.
Morning, fasted, standardized assay, repeated. Always interpreted with SHBG, LH, FSH, and estradiol, so you can distinguish a testes problem from a brain-signal problem from a binding-protein artifact. Comprehensive testing platforms have made this radically more accessible: Function Health gives members access to 160+ lab biomarkers a year — including testosterone, free-testosterone context, and the full upstream hormone panel — tracked over time in one place, while Superpower offers a 100+ biomarker baseline with AI-generated interpretation for roughly the price of a gym membership. The point is not the brand; it is the longitudinal trend line. One reading is gossip; a trend is data.
2. Attack the modifiable forces in order of leverage.
For most men the ranking is unglamorous and correct: visceral fat first (it breaks the aromatase cycle), then sleep (which protects the nocturnal-to-morning testosterone rise), then resistance training and protein, then avoidable EDC exposure — swapping plastic food storage for glass, skipping the receipt, choosing fragrance-free, and, if you want the feedback loop, quantifying the change with an at-home exposure test. These are not competing religions. They are levers with different magnitudes, and your data tells you which one is yours.
3. Know which dips are normal.
New fatherhood lowers testosterone by design, and it tends to return to baseline. Don't medicalize biology. Conversely, don't dismiss a genuine decline as "just stress" when the trend, the symptoms, and the metabolic markers all point in the same direction.
4. Personalize before you optimize.
Layer your genome onto your phenotype so that any intervention — from training periodization to Peptide Therapy — is matched to how your receptors and clearance pathways actually behave. This is the entire premise of a digital-twin approach to longevity: the model carries the context a single lab value never can, and the Coach / Practitioner and Athlete / Patient make decisions from the same evidence base.
How the field compares.
It is worth being clear-eyed about where each kind of company sits, because they are solving different slices of the problem. Reference laboratories and instrument makers — Quest, Labcorp, Thermo Fisher — fixed the measurement so a number means the same thing everywhere. Comprehensive testing memberships, such as Function Health and Superpower, fixed access and longitudinality, putting a wide biomarker panel and AI interpretation in consumers' hands. Exposure-testing innovators like Million Marker fixed the blind spot around the chemicals themselves. Functional-genomics providers add the individualization layer. And pharma — Novo Nordisk, Eli Lilly, AbbVie — supplies the heavy-duty interventions for the cases where lifestyle is necessary but not sufficient. A digital-twin platform's job is to be the connective tissue: to fuse those data streams into one model of one person, so the plan is built around the patient rather than the population.
The decades-long decline in male testosterone is real, it is multi-causal, and a good chunk of it traces to forces no individual chose. But "you didn't cause it" and "you can't influence it" are different sentences. The chemistry is partly avoidable, the fat is reversible, the fatherhood dip is temporary, and your genetics are knowable. For the person willing to trade guesswork for data, that is not a doom story. It is a to-do list — and the best time to start a longevity plan is, reliably, about a decade before you think you need one.
Sign up for FREE daily Longevity Club Workshops, or join the Affiliate Program (pays 20%).
About the Author
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data and leverages proprietary Digital Twin for Predictive Peptide Performance™ technology, wearable data, and biomarker data to deliver personalized optimization and longevity recommendations. A 3x technology/AI company CEO with 2 successful exits, Tony has completed 3 Full Ironman Triathlons (140.6 mi) since 2019. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University, and has worked with the US Olympic Team, the NBA, NFL, MLB, NASA, Google, Microsoft, and Netflix, among others. He also served as a US Navy Officer commanding an emergency response team aboard a destroyer.
Disclaimer: This article is for educational purposes and is not medical advice, diagnosis, or treatment. Testosterone, peptide, and hormone decisions should be made with a qualified clinician who can interpret your individual results. Reference ranges, assays, and products are described as of publication and may change.