Peptide Science
·14 min read
When Peptides Meet: The Science of Synergy, Interference, and the Combinations That Don't Belong in the Same Syringe
A buyer's guide to peptide interactions, from GLP-1 stacks to growth-hormone pairings, and how your genome and an AI Digital Twin determine what actually works for you.
By Tony Medrano, LongevityPlan.AI
Ask a chemist what happens when you put two peptides into the same body, and you will get a more interesting answer than you expect. It is not "they add up." Sometimes one peptide makes the other two to ten times stronger. Sometimes one quietly cancels the other out. And in a few cases—usually involving a drug your physician already prescribed—two well-meaning molecules can hand you a hypoglycemic episode at the worst possible moment, like during a board presentation or the back half of a long ride.
This is the question that matters most for anyone now exploring Peptide Therapy as part of a longevity strategy, and it is the one most "stack guides" on the internet skip. In earlier issues of this newsletter, I have written about individual peptides—the BPC-157 and TB-500 repair pairing, the five peptides every endurance athlete should understand, and the best peptides for inflammation. Readers kept asking the obvious follow-up: Okay, but can I take them together? So let us answer it properly, with data, with the scientists who built this field, and without the hand-waving.
The honest headline: peptides absolutely interact with one another—and with your existing medications—but they do so according to a logic that differs from that of the small-molecule pills most of us grew up with. Understanding that logic is the difference between a stack that compounds your results and one that compounds your risk.
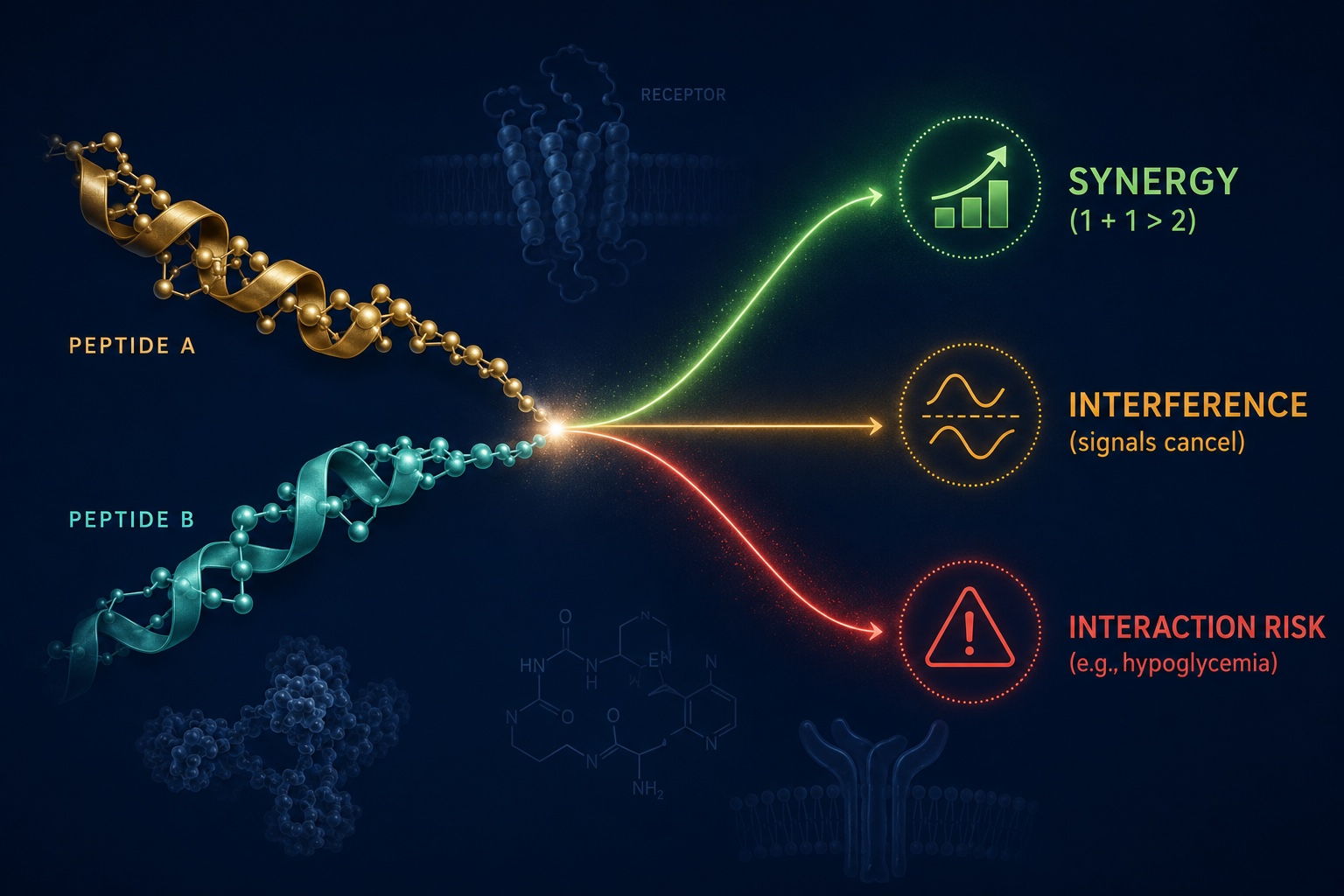
Do Peptides Interact With Each Other? How Synergy, Interference, and Drug Safety Work in the Human Body
Peptides rarely simply "add up." When two are combined in the body, the result can be synergy, interference, or a genuine safety interaction — and which one you get depends on the molecules, the dose, and the person.
1. Why peptides don't play by small-molecule rules
When you swallow a typical pharmaceutical—a statin, an antidepressant, a blood thinner—much of the drug-interaction drama happens in the liver, where a family of enzymes called cytochrome P450 (CYP450) chews drugs up. Two drugs that compete for the same enzyme can spike or crater each other's blood levels. That is the classic "grapefruit juice" interaction.
Most therapeutic peptides largely sidestep this machinery. They are chains of amino acids, so the body disposes of them the way it disposes of dietary protein: peptidases and proteases snip them apart into fragments and amino acids, with little to no involvement of the CYP450 system.[1] The GLP-1 receptor agonists that have reshaped metabolic medicine—semaglutide, liraglutide, dulaglutide—are eliminated this way and, accordingly, show minimal classic metabolic drug-drug interactions.[3] That is genuinely good news, and it is part of why this class has been deployed so widely and so safely.
But "low CYP risk" is not the same as "no interactions," and this is where the consumer guides go wrong. A rigorous 2025 follow-up analysis of every therapeutic peptide approved between 2021 and 2024, published in Clinical and Translational Science, found that peptides can still act on drug transporters: the small peptide danicopan, for example, raised exposure of the cholesterol drug rosuvastatin by roughly 2.25-fold and the antihistamine fexofenadine by 1.62-fold by inhibiting transporter proteins.[1] Peptides interact—they simply do it through different doors.
There is also a chemistry problem that small molecules rarely face: peptides are fragile and finicky. Few people understand this better than Professor David Craik of the University of Queensland's Institute for Molecular Bioscience, who discovered cyclotides—the largest known family of circular proteins—and who directs the Australian Research Council Centre of Excellence for Innovations in Peptide and Protein Science. Craik's life's work is essentially a meditation on peptide stability: cyclotides survive boiling and resist enzymatic degradation precisely because nature locked them into a "cyclic cystine knot," a circular backbone cross-linked by a knotted arrangement of disulfide bonds.[21] His group grafts useful drug sequences onto these ultra-stable scaffolds specifically to overcome the two great weaknesses of ordinary peptides—poor bioavailability and rapid breakdown in the body.[22]
The practical takeaway for the buyer: a peptide's behavior depends on its exact structure, its pH, its solubility, and the company it keeps. Two peptides that are each fine on their own can be chemically incompatible in the same vial. That single fact undermines a lot of "mix-it-yourself" advice, and we will return to it.
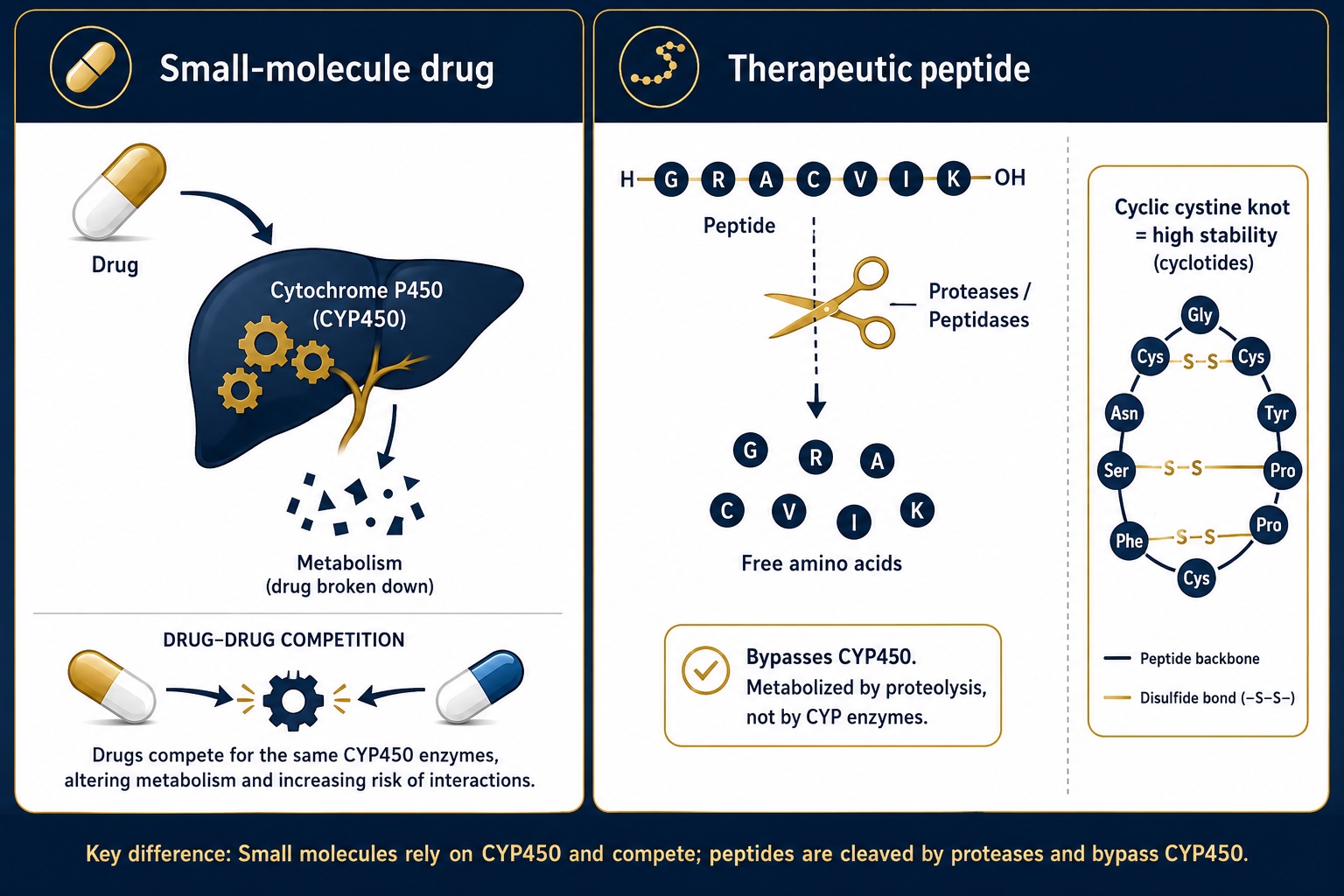
Why Peptides Bypass CYP450: Protease Metabolism vs. Liver Enzymes and the Cyclic Cystine Knot
Most peptides are cleared by proteases rather than the liver's CYP450 enzymes, lowering classic drug-interaction risk — but their fragile chemistry and structures like the ultra-stable cyclic cystine knot, still govern how they behave together.
2. The synergists: when 1 + 1 is greater than 2
The most important peptide-interaction story in modern medicine is not a warning. It is a triumph—and it has made some drug developers very rich. The entire frontier of metabolic medicine is, at bottom, a story about combining peptide activities on purpose.
Growth-hormone pairings: the original "stack"
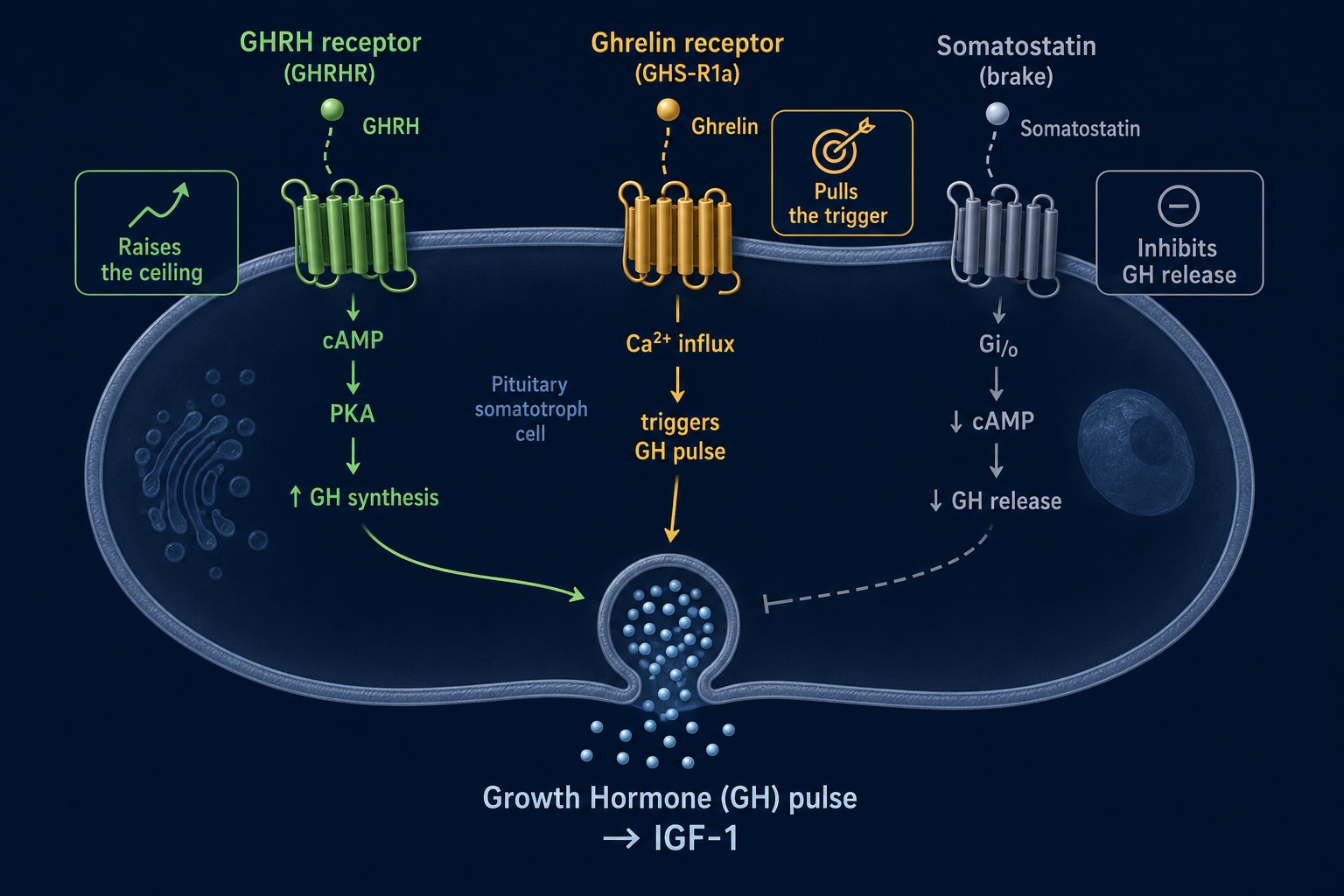
Start with the combination that built the peptide-clinic industry: a growth-hormone-releasing hormone (GHRH) analog paired with a growth-hormone-releasing peptide (GHRP). The biology is elegant. Your pituitary's somatotroph cells carry two separate "go" switches. The GHRH receptor works through a cAMP pathway that raises the ceiling on how much growth hormone a cell can release. The ghrelin receptor (GHS-R1a) works through a calcium pathway that triggers the actual pulse. Hit both switches at once and you get a release of growth hormone that is substantially larger than either compound produces alone—a true synergy documented in the GHRH-plus-GHRP literature since the 1990s.[12]
This is why the pairing of a long-acting GHRH analog with the selective secretagogue ipamorelin became a clinic staple. Ipamorelin earned its place because, in the foundational 1998 characterization by Raun and colleagues, it stimulated growth hormone cleanly—without the cortisol and prolactin spikes that plagued earlier secretagogues.[11] Pair a "primer" that sustains the signal for days with a "trigger" that delivers a clean pulse, and the two cover each other's weaknesses. It is the tortoise and the hare running as relay partners rather than competitors.
GHRH + GHRP Synergy Explained: How Two Pituitary Receptors Amplify Growth Hormone Release
The classic growth-hormone "stack" works because a GHRH analog and a GHRP (such as ipamorelin) hit two independent receptors — one raises GH capacity, the other triggers the pulse — producing a release larger than either achieves alone.
Incretin co-agonism: combination inside a single molecule
The most consequential synergy of the decade took the combination idea one step further—and folded two peptide actions into a single engineered molecule. Tirzepatide, Eli Lilly's blockbuster, is a dual agonist that activates both the GLP-1 and GIP receptors. In the head-to-head SURPASS-2 trial against semaglutide, all three tirzepatide doses delivered superior reductions in glucose and weight, with low rates of hypoglycemia of roughly 0.2–1.7%.[6] Adding GIP pharmacology to GLP-1 therapy, the investigators concluded, was the advantage.
No one has done more to illuminate this biology than Professor Daniel Drucker of the Lunenfeld-Tanenbaum Research Institute at Mount Sinai Hospital in Toronto, who holds the Banting and Best–Novo Nordisk Chair in Incretin Biology and whose lab helped define how these gut hormones work.[7] Speaking with the cardiologist and digital-medicine pioneer Eric Topol, Drucker made a candid admission about just how strange and powerful these combinations are: at the GIP level, he noted, two of the most effective obesity drugs appear to have "opposite effect," and yet both work spectacularly—"I don't think we fully understand."[8] That intellectual humility from the field's leading figure is worth sitting with. Combination peptide pharmacology is outrunning our mechanistic explanations.
The synergy keeps compounding. Novo Nordisk's CagriSema pairs the amylin-receptor agonist cagrilintide with semaglutide in a single weekly injection. In the 68-week REDEFINE 1 trial, the combination produced up to 22.7% weight loss, versus 16.1% for semaglutide alone and 11.8% for cagrilintide alone—two peptides that, together, beat either by itself.[13] "By combining semaglutide and cagrilintide," said Novo Nordisk's head of development Martin Holst Lange, "we're seeing superior outcomes... beyond those achieved with each therapy individually."[14] And Lilly's triple agonist retatrutide—hitting GLP-1, GIP, and glucagon receptors at once—reached 24.2% mean weight loss at 48 weeks in its phase 2 obesity data, reportedly without yet hitting a plateau.[9]
The lesson the pharmaceutical industry is teaching us, at the cost of billions in R&D, is that thoughtful peptide combination is one of the most powerful tools in medicine. The operative word is thoughtful.
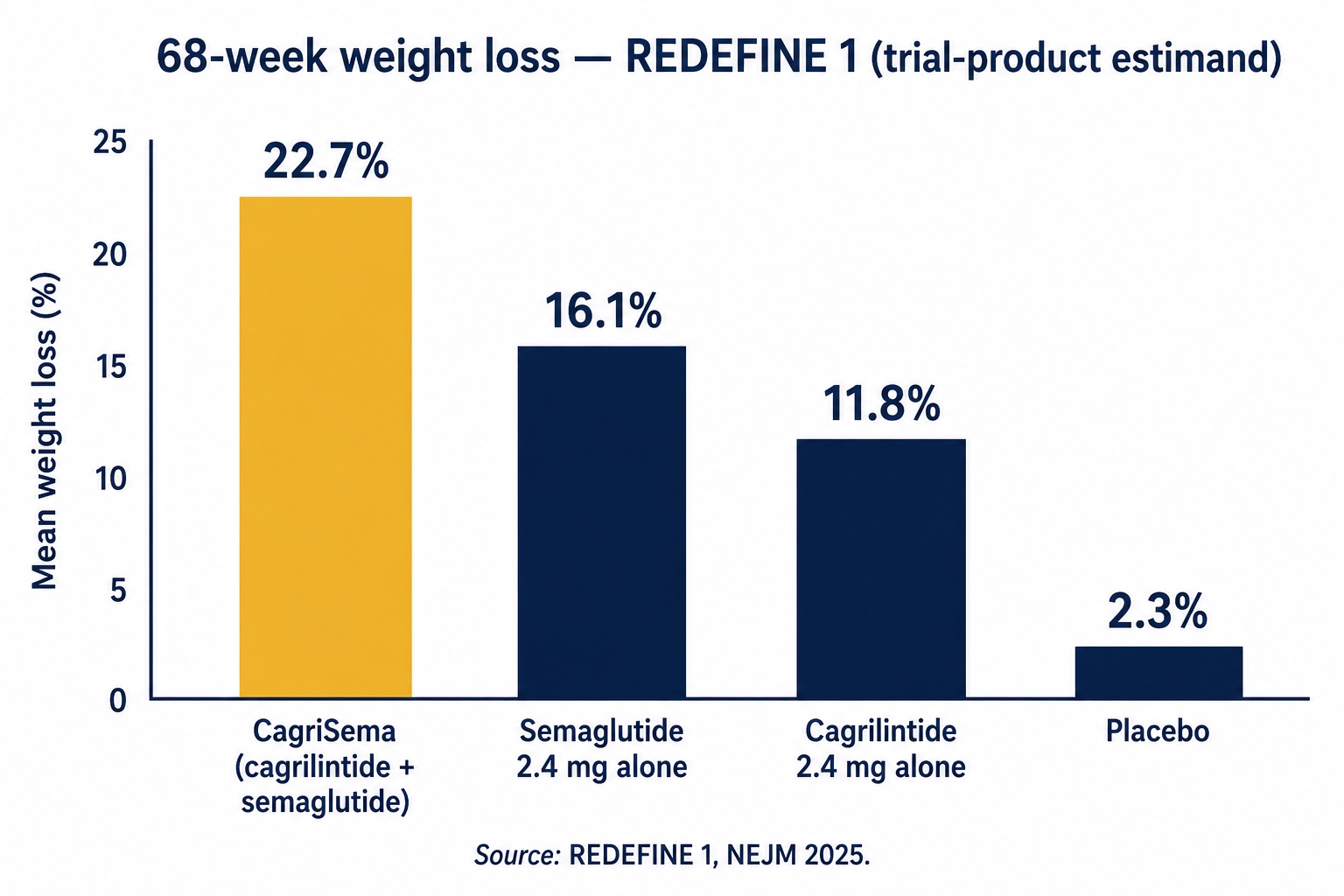
CagriSema vs. Semaglutide vs. Cagrilintide: REDEFINE 1 Weight-Loss Results for Combination Peptide Therapy
Real synergy is engineered and trial-tested: in REDEFINE 1, the two-peptide combination CagriSema outperformed either component alone — the principle behind why "thoughtful" combination, not "more," is what works.
3. The saboteurs: redundancy, competition, and desensitization
If synergy is the upside, the mirror image is interference—and it is the part of "stacking" most enthusiasts ignore because it is invisible. You do not feel two peptides canceling each other out; you simply feel less than you paid for.
Three failure modes dominate. The first is receptor competition: two peptides targeting the same receptor can crowd each other out, so that a "more is better" stack delivers no more signal than a single well-chosen agent. The second is redundancy: stacking two compounds that drive the same downstream pathway (say, two different growth-hormone secretagogues that both lean on the same pulse) can hit a physiological ceiling, where the body's own brakes—somatostatin, in the GH axis—simply clamp down harder. The third, and most underappreciated, is receptor desensitization: chronic over-stimulation of a receptor causes the cell to pull receptors off its surface, blunting the response over time.
Here, again, the precision-engineering frontier is instructive. Part of what makes tirzepatide remarkable is that it activates the GLP-1 receptor in a way that produces less receptor desensitization than native GLP-1—a structural subtlety revealed by cryo-electron-microscopy studies of how the molecule docks.[6] The amount of signal you get is not just about how much peptide you push in; it is about how the receptor responds, recycles, and fatigues. A naive stack that simply piles agonists on top of one another can accelerate exactly the desensitization it is trying to overcome.
This is why "interference" deserves equal billing with "synergy" in any serious conversation about combining peptides. The difference between the two is not the dose. It is the design.
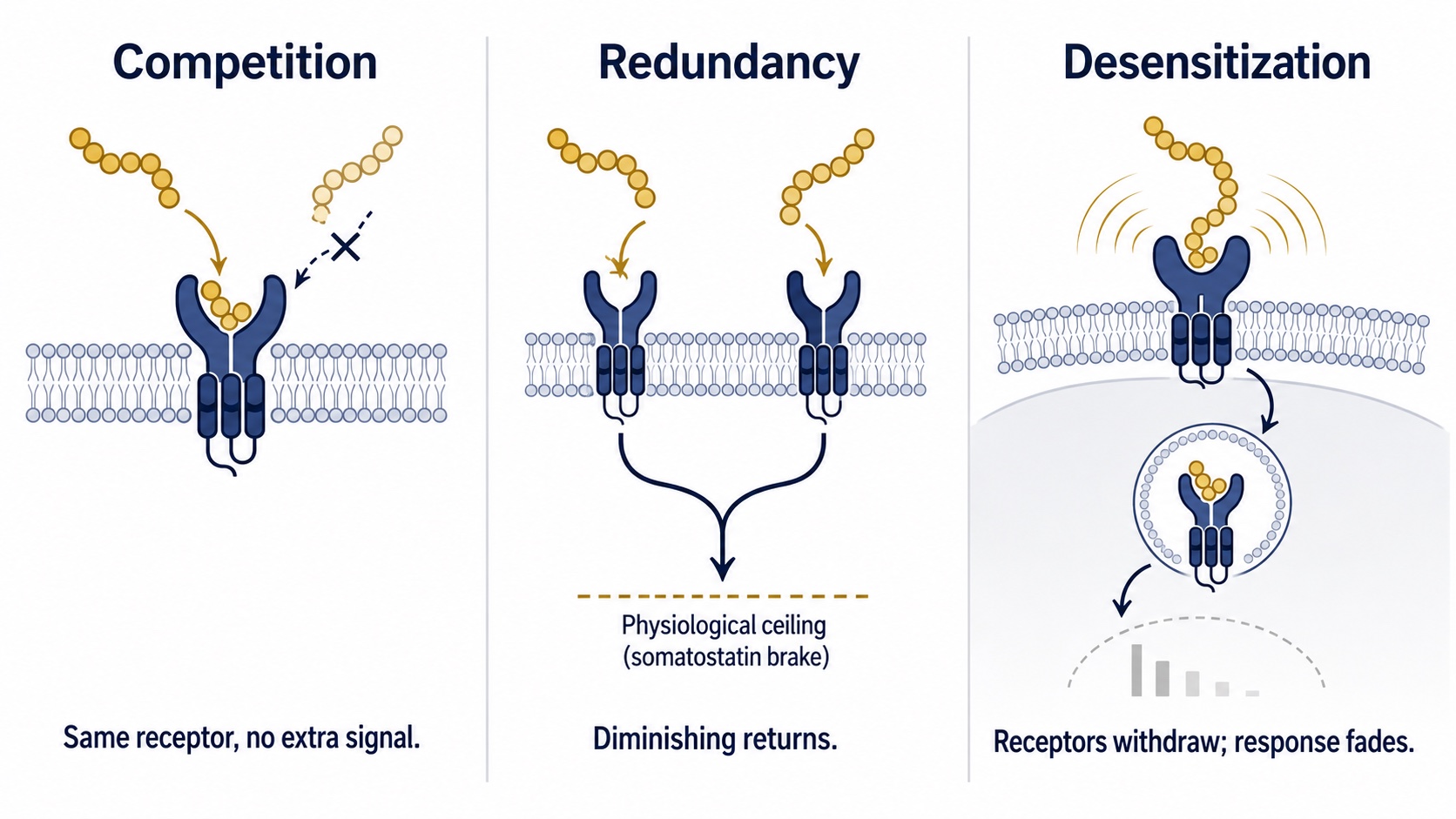
How Peptide Stacks Fail: Receptor Competition, Pathway Redundancy, and Receptor Desensitization
The invisible downside of careless stacking: combinations can compete for the same receptor, hit a physiological ceiling, or accelerate the very receptor desensitization they're trying to overcome.
4. The pairings that warrant real caution
Now the part that protects you. Some interactions are not about diminishing returns—they are about safety. The clearest and most clinically documented examples involve GLP-1-class peptides, because those are the peptides most likely to sit alongside other prescriptions in a real person's medicine cabinet.
GLP-1 plus insulin or sulfonylureas: the hypoglycemia trap
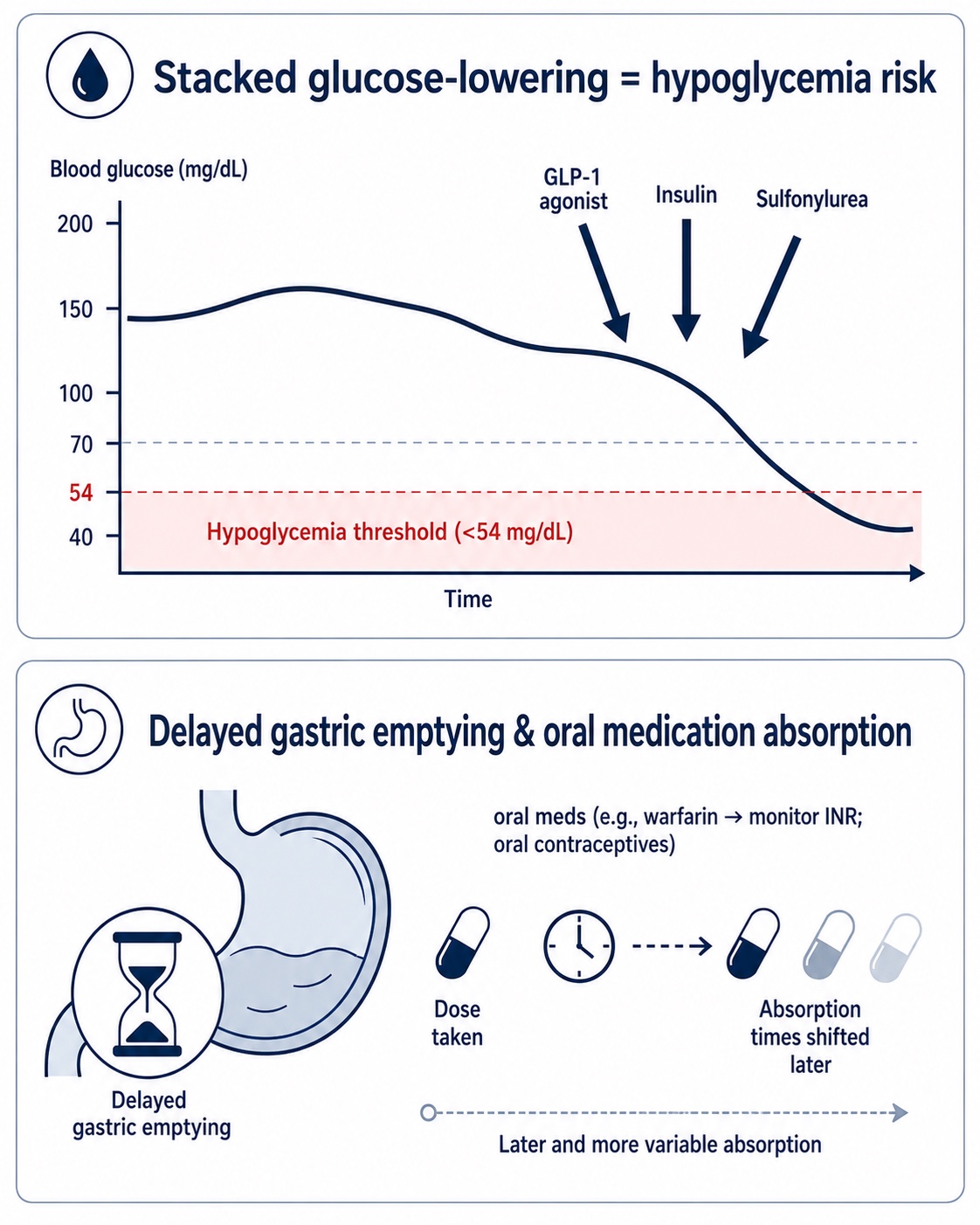
This is the single most important interaction in this article, and it is not exotic. GLP-1 receptor agonists lower glucose. So do insulin and the older "secretagogue" diabetes drugs called sulfonylureas (glipizide, glyburide, and relatives). Layer a GLP-1 agonist on top of either without adjusting the dose, and you can drive blood sugar dangerously low. The clinical literature is unambiguous: concomitant use of insulin or insulin secretagogues with GLP-1 therapy potentiates the risk of hypoglycemia, and patients on these combinations require education and monitoring.[3] This is not a reason to avoid the combination—physicians use it deliberately and successfully every day—but it is a reason that "I added a peptide I bought online to the medication my doctor prescribed" is a sentence that should never be spoken.
The gastric-emptying effect: a timing problem hiding in plain sight
GLP-1 peptides slow the rate at which your stomach empties. That is part of how they curb appetite—and it is also why they quietly change the absorption of other things you swallow. Oxford's 2024 review of GLP-1 effects on gut motility clearly lays out the mechanism and its consequences.[4] Practically, this means oral medications can be absorbed more slowly or unpredictably. Co-administration with warfarin, for instance, can delay the blood thinner's peak and warrants closer monitoring of clotting (INR); oral contraceptives and acetaminophen are generally recommended to be taken with timing offsets from the injection.[5] If you are an executive juggling a half-dozen prescriptions, the interaction that gets you is rarely dramatic. It is a slow drift in a drug level you assumed was stable.
GLP-1 Drug Interactions: Hypoglycemia Risk With Insulin or Sulfonylureas and Delayed Gastric Emptying
The interactions most likely to harm a real person aren't peptide-on-peptide — they're peptide-on-prescription: GLP-1 agonists added to insulin or sulfonylureas can drive glucose dangerously low, and slowed stomach emptying can shift how oral drugs are absorbed.
Stacking sedation, immune signaling, and the unknown
Beyond the metabolic peptides, much of the "wellness peptide" market—compounds marketed for sleep, healing, cognition, or pigmentation—has limited human interaction data. When you combine multiple immune-modulating or vasoactive peptides, or layer sedating peptides on top of other central nervous system agents, you are operating in a zone where controlled trials simply have not been run. The responsible posture there is not bravado; it is humility, supervision, and the assumption that absence of evidence is not evidence of safety.
5. The chemistry problem—and the regulatory reality
Even when two peptides are pharmacologically compatible, they may not be physically compatible. Combining peptides in a single injection raises real questions of pH, solubility, and stability—the very fragility issues that David Craik's stability research exists to solve. A peptide that is stable at one pH can aggregate or degrade when mixed with another that requires a different formulation. This is precision pharmacy, not kitchen chemistry, and it is one reason why the source of your peptide matters as much as the molecule itself.
Which brings us to the regulatory landscape, because it is shifting fast, and the headlines mislead. In April 2026, the U.S. Food and Drug Administration removed BPC-157, TB-500, and CJC-1295 from "Category 2" of its 503A bulk-substances list—the category flagging safety concerns—after the substances' nominations were withdrawn.[19] Crucially, the FDA did not move them to the approved Category 1 list, and none is an FDA-approved drug with a recognized monograph; they sit in a regulatory gray zone, neither clearly prohibited nor authorized.[20] The agency's Pharmacy Compounding Advisory Committee is scheduled to meet on July 23–24, 2026, to formally evaluate whether BPC-157, KPV, TB-500, MOTs-C, and several others should join the compounding list, with a public docket (FDA-2025-N-6895) collecting the scientific evidence.[18]
Why does this belong in an article about interactions? Because the biggest interaction risk for many consumers is not peptide-on-peptide—it is peptide-on-impurity. Research-only products are not manufactured to pharmaceutical standards and may skip the stability, potency, and endotoxin testing that injectable drugs require.[19] When you do not know exactly what is in the vial, you cannot reason about how it will interact with anything. A clean, tested, single-source product is the precondition for every other safety judgment in this piece.
6. The variable nobody can buy around: your genome
Here is the uncomfortable truth that the supplement aisle and the boutique clinic are equally reluctant to tell you: the same peptide, at the same dose, in two different people, can produce wildly different results—and a meaningful share of that difference is written in your DNA.
The evidence is now hard to dismiss. In April 2026, scientists at the 23andMe Research Institute published a genome-wide association study in Nature of nearly 27,885 people on GLP-1 receptor agonists. They identified a missense variant in the GLP1R gene—the gene encoding the very receptor these drugs target—significantly associated with greater weight-loss efficacy (P = 2.9 × 10⁻¹⁰), worth roughly an additional 0.76 kg of weight loss per copy of the effect allele. They also linked variants in GLP1R and GIPR to nausea and vomiting, with the GIPR association showing up only in people taking tirzepatide—the drug that also hits the GIP receptor.[16] In plain English: your genotype helps predict both how well a peptide works and how sick it makes you, and which genes matter depends on which peptide you take.
A separate 2025 study in Obesity drove the point home with startling effect sizes. Among 112 patients on semaglutide, carriers of the rs6923761 "A" variant in GLP1R lost weight faster than non-carriers—and when sex was layered in, women homozygous for the A allele lost weight at more than double the rate of men carrying the G allele (about 1.89% versus under 1% of body weight per month).[15] Two people on the identical drug, identical dose, twice the result—decided substantially before either walked into the clinic.
This is the scientific foundation for treating genetics as the bedrock of any serious peptide plan. Genomic assessment—the kind offered by dedicated partners such as The Genomics Company—is not a luxury add-on. It is the first data layer, the one that tells you whether a given Peptide Therapy is likely to be a strong match, a weak match, or a side-effect risk for your particular biology before you spend a dollar or take a single injection. Everyone is different; the peptide market's dirty secret is that it sells the same protocol to everyone anyway.
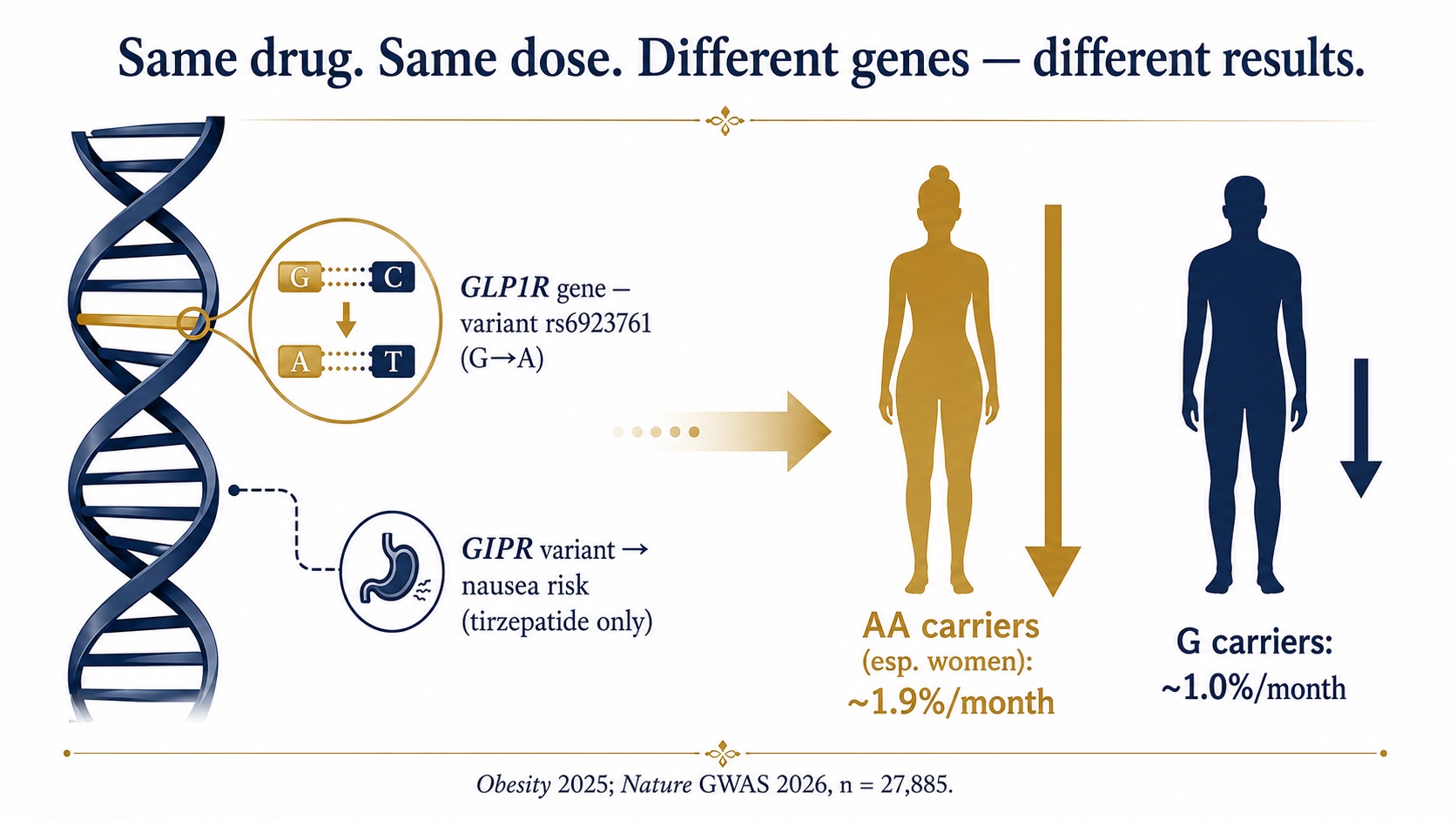
Pharmacogenomics of GLP-1 Therapy: How the GLP1R rs6923761 Variant Changes Peptide Weight-Loss Response
Your genome is the variable no protocol can buy around: variants in GLP1R — and, for tirzepatide, GIPR — measurably change both how well a peptide works and how sick it makes you, which is why genetics is the foundation of a personalized plan.
7. From data to decision: the Digital Twin for Predictive Peptide Performance™
If genetics is the bedrock, it is still only one input. The reason peptide interactions are so hard to reason about intuitively is that the relevant variables—genotype, current medications, hormones, sleep, training load, recovery, inflammation, glucose dynamics—do not live in a single place. They live across your multi-modal health data, scattered between a lab report, a wearable, a pharmacy record, and a genome file that have never spoken to each other.
This is exactly the integration problem that AI was built to solve, and it is the core of how LongevityPlan.AI approaches the question. A Digital Twin for Predictive Peptide Performance™ is a personalized, computational model of you—an extension of the broader Cardiorespiratory Digital Twin™ concept—that fuses these streams so that a peptide decision can be modeled before it is made. The architecture has two halves. The sensor layer ingests the raw signal: genomic variants, bloodwork, continuous glucose and heart-rate data, sleep architecture, and the medication list. The intelligence layer turns that signal into foresight, using predictive modeling to flag the synergies worth pursuing and the interactions worth avoiding—the GLP-1-plus-sulfonylurea hypoglycemia trap, the genotype that predicts a poor response, the gastric-emptying shift that will quietly move a warfarin level.
The point is not to replace clinical judgment but to inform it. In a well-run program, the twin becomes a shared decision surface between the Coach / Practitioner and the Athlete / Patient—a way to run "what-if" scenarios on a model instead of on a person, and to convert vague optimism into specific, testable, AI-powered coaching improvements that get refined as new data arrives.
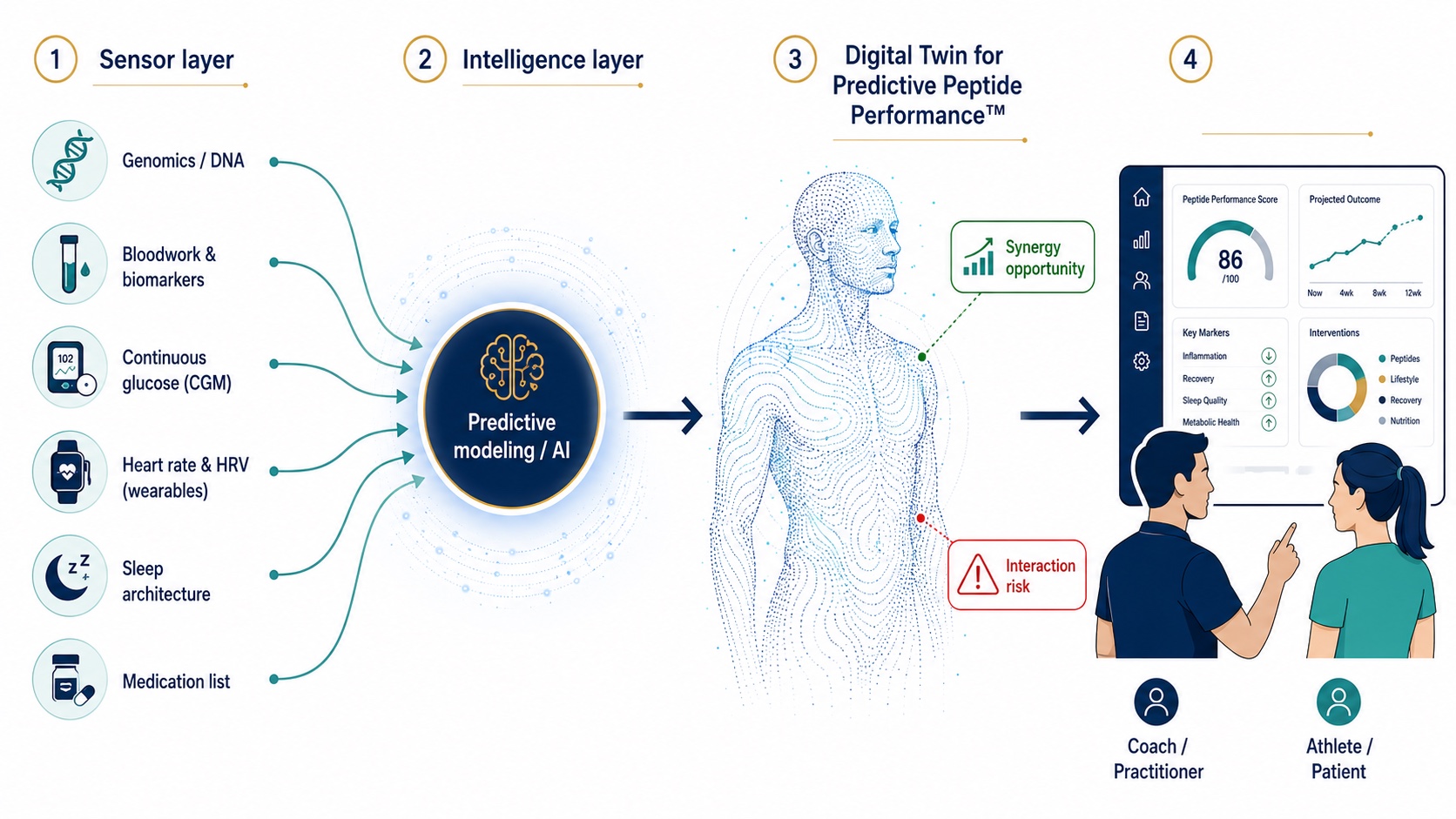
Digital Twin for Predictive Peptide Performance: AI Architecture From Sensor Layer to Personalized Coaching
A Digital Twin for Predictive Peptide Performance™ fuses multimodal health data through an intelligence layer, enabling a peptide decision to be modeled — and its risks flagged — before it's ever made.
And the same AI revolution is now upstream, in how the peptides themselves are discovered. Generative models—variational autoencoders, transformers, and diffusion models—are being used to design novel peptide sequences with target properties built in.[24] In October 2025, the AI-driven biotech Insilico Medicine reported using its generative-biologics engine to design peptides targeting the GLP-1 receptor in roughly 72 hours, a timeline that would have been unthinkable a decade ago.[23] The field is moving from discovering peptides we stumble upon to designing peptides—and peptide combinations—to specification. The decision tools on the consumer side have to keep pace.
8. A skeptic's buyer's guide
If you are an over-40 executive, an aspirational master's athlete, or someone rebuilding after injury or illness and weighing whether peptides belong in your Peptide Longevity Plan™, here is a framework that respects both your ambition and your safety. It is deliberately not a dosing protocol—those belong to your physician—but a set of questions that separate signal from sales pitch.
- Start with your genome and your medication list, not the peptide. Genotyping and a full reconciliation of what you already take is the cheapest risk-reduction you will ever buy. The most dangerous interactions are with the drugs you already have.
- Demand to know the source and the testing. If a provider cannot tell you whether the product is third-party tested for potency, purity, and endotoxins, you cannot reason about interactions, because you do not know what is in the vial.[19]
- Treat "stacking" claims as hypotheses, not facts. Ask whether a proposed combination has a mechanistic rationale (different receptors, complementary pathways) or is simply two things sold together. The CagriSema and tirzepatide stories show that real synergy is engineered and trial-tested—not assumed.[13]
- Respect the gray zone. Many popular peptides are not FDA-approved and sit in active regulatory review.[18] That is a reason for medical supervision, not a reason to route around it.
- Measure, then adjust. Longevity is a data discipline. A plan that does not track outcomes—glucose, body composition, recovery, biomarkers—is a belief system, not a protocol.
This is the same evidence-first posture that informs the protocols at Stanford Athletics, the U.S. Olympic program, and NASA's human-performance work, and the one championed by clinicians like Eric Topol and Peter Attia: precision over averages, prevention over reaction, and personalization over one-size-fits-all. It is also why our Corporate Wellness Program and Longevity Club are built around individual data rather than blanket protocols—because the entire premise of this article is that your peptide is not your colleague's peptide.
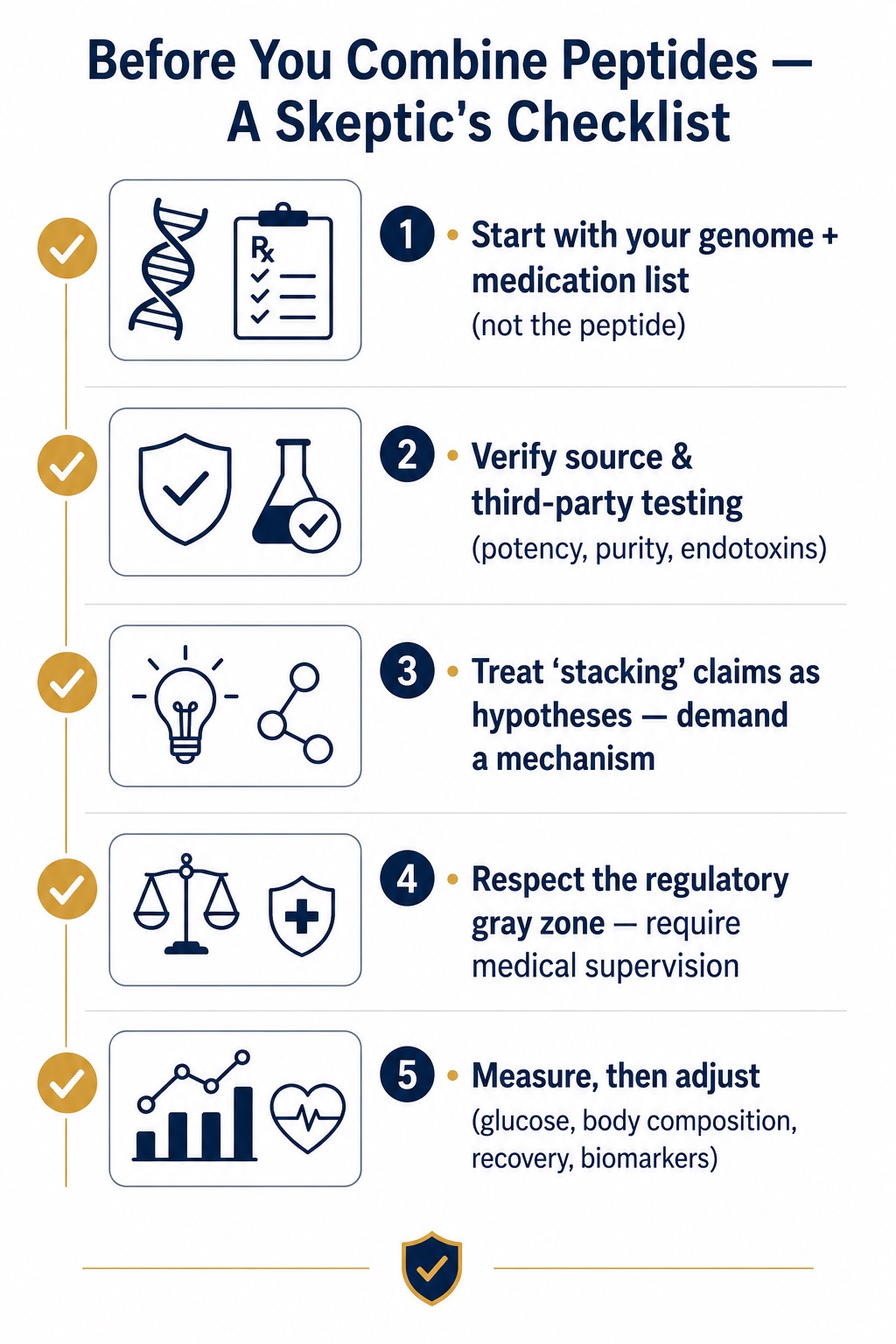
Peptide Therapy Buyer's Guide: A 5-Step Safety and Personalization Checklist for Longevity Planning
Longevity is a data discipline. These five questions separate an evidence-based Peptide Longevity Plan™ from a sales pitch — and keep personalization, sourcing, and supervision at the center.
The bottom line
Do peptides interact? Profoundly—sometimes to your enormous benefit, sometimes to your detriment, and sometimes in ways the world's leading incretin scientist will tell you we do not yet fully understand. The combinations that built a new era of metabolic medicine—GLP-1 with GIP, GLP-1 with amylin, GHRH with GHRP—prove that synergy is real and powerful. The hypoglycemia traps and absorption shifts prove the danger is real, too. And the genetics prove that the only honest answer to "which peptides should I combine?" begins with another question: combine them in whom?
The future of this field will not be won by the person with the longest stack. It will be won by the person—and the model—who knows their own biology well enough to choose the right two molecules from a trusted source at the right moment, and to leave the wrong ones out of the syringe. That is not biohacking. That is just good science, applied to a life worth extending.
Endnotes & Sources
- Säll C, et al. "Clinical Significance of Drug–Drug Interaction Studies During Therapeutic Peptide Drug Development: Follow-Up Investigation of Therapeutic Peptides Approved Between 2021 and 2024." Clinical and Translational Science, 2025. https://pmc.ncbi.nlm.nih.gov/articles/PMC12239508/
- "Evaluating Drug–Drug Interaction Risk Associated with Peptide Analogs Using Advanced In Vitro Systems." ScienceDirect, 2025. https://www.sciencedirect.com/science/article/pii/S0090955624119897
- Collins L, Costello RA. "Glucagon-Like Peptide-1 Receptor Agonists." StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK572151/
- "Physiology and Pharmacology of Effects of GLP-1-based Therapies on Gastric, Biliary and Intestinal Motility." Endocrinology (Oxford Academic), 2024;166(1):bqae155. https://academic.oup.com/endo/article/166/1/bqae155/7906037
- "GLP-1 Interactions: Risks, Effects, and Recommendations" and "How Do GLP-1 Receptor Agonists Work?" Endocrinology Advisor, 2025–2026. https://www.endocrinologyadvisor.com/factsheets/glp-1-interactions/
- Frías JP, et al. "Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes" (SURPASS-2). New England Journal of Medicine, 2021;385:503–515. https://www.nejm.org/doi/full/10.1056/NEJMoa2107519 · See also "Structural determinants of dual incretin receptor agonism by tirzepatide," PMC9060465.
- "Q&A with Daniel Drucker." Med (Cell Press), 2024. https://www.cell.com/med/fulltext/S2666-6340(24)00293-9
- Topol E. "Daniel Drucker: Illuminating the GLP-1 Drug's Break Out." Ground Truths, 2024. https://erictopol.substack.com/p/daniel-drucker-illuminating-the-glp
- "Triple Agonism Based Therapies for Obesity" (retatrutide review). PMC12304053. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12304053/ · See also "The discovery and development of GLP-1 based drugs that have revolutionized the treatment of obesity," PNAS, 2024.
- Müller TD, Blüher M, Tschöp MH, DiMarchi RD. "Anti-obesity drug discovery: advances and challenges." Nature Reviews Drug Discovery, 2022;21(3):201–223.
- Raun K, et al. "Ipamorelin, the first selective growth hormone secretagogue." European Journal of Endocrinology, 1998. PMID 9544837.
- Teichman SL, et al. "Prolonged stimulation of growth hormone and IGF-I by CJC-1295." Journal of Clinical Endocrinology & Metabolism, 2006 (single doses in 65 healthy adults; 2–10× GH increase lasting ~6 days). See also Jetté L, et al., PMID 16352683; foundational GHRH+GHRP synergy, PMID 10372741.
- "Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity" (REDEFINE 1). New England Journal of Medicine, 2025; NEJMoa2502081. Reported figures: up to 22.7% weight loss with CagriSema vs 16.1% semaglutide and 11.8% cagrilintide alone at 68 weeks (trial-product estimand). https://www.nejm.org/doi/full/10.1056/NEJMoa2502081
- Novo Nordisk. REDEFINE 1 / REIMAGINE 2 headline results and statements from Martin Holst Lange, EVP & Head of Development, 2025–2026. https://www.novonordisk.com/news-and-media/news-and-ir-materials.html
- Phan C, et al. "A GLP1R gene variant and sex influence the response to semaglutide treatment in patients with severe obesity." Obesity (Silver Spring), 2025;33(7):1237–1242. https://onlinelibrary.wiley.com/doi/10.1002/oby.24300
- "Genetic predictors of GLP1 receptor agonist weight loss and side effects" (23andMe Research Institute; GWAS of 27,885 individuals). Nature, 2026. https://www.nature.com/articles/s41586-026-10330-z
- 23andMe Research. "Unlocking the Genetics of GLP-1 Medications: Why Your DNA Matters," 2026. https://blog.23andme.com/articles/glp-1-medications-why-your-dna-matters
- U.S. FDA. "July 23–24, 2026: Meeting of the Pharmacy Compounding Advisory Committee" (BPC-157, KPV, TB-500, MOTs-C, DSIP/Emideltide, Semax and others; docket FDA-2025-N-6895). https://www.fda.gov/advisory-committees/advisory-committee-calendar/july-23-24-2026-meeting-pharmacy-compounding-advisory-committee-07232026
- "Recent Regulatory Updates on Compounded Peptide Injections." New Drug Loft / VLS Pharmacy, 2026 (FDA removed BPC-157, TB-500, CJC-1295 from Category 2 in April 2026; quality-testing standards for compounded vs research-only product). https://newdrugloft.com/recent-regulatory-updates-on-compounded-peptide-injections/
- "BPC-157 Legal Status 2026: FDA Category 2 Removal, PCAC Review & RUO Access," Loti Labs, 2026; and "FDA's Pep(tide) Rally," FDA Law Blog, April 2026. https://www.thefdalawblog.com/2026/04/fdas-peptide-rally-what-compounders-and-industry-need-to-know-post-1-of-2/
- Professor David Craik, UQ Experts & Institute for Molecular Bioscience profile (cyclotides; cyclic cystine knot; ARC Centre of Excellence in Peptide and Protein Science). https://about.uq.edu.au/experts/456 · https://imb.uq.edu.au/research-groups/craik
- "Harnessing cyclotides to design and develop novel peptide GPCR ligands." RSC Chemical Biology, 2020;1:177. https://pubs.rsc.org/en/content/articlelanding/2020/cb/d0cb00062k
- Insilico Medicine. "Insilico showcases advanced generative biologics engine in breakthrough 72-hour peptide design targeting GLP1R for cardiometabolic disease," October 2025. https://insilico.com/news
- Choudhury C, et al. "In Silico Peptide Design: Methods, Resources, and Role of AI." Journal of Peptide Science, 2025. https://onlinelibrary.wiley.com/doi/10.1002/psc.70063
- "AI-driven bioactive peptide discovery of next-generation metabolic biotherapeutics." Applied Food Research, 2025;5:101291; and "Peptide-based drug design using generative AI," Chemical Communications, 2026.
Disclaimer: This article is educational and is not medical advice. Peptide therapies—including several discussed here—may be unapproved, investigational, or under active FDA review, and combining peptides or adding them to existing prescriptions can carry real risks, including hypoglycemia and altered drug absorption. Decisions about any peptide protocol should be made with a licensed physician using your individual genetics, medications, and clinical history.
Earn while you share. Join the LongevityPlan Affiliate Program and earn 20% on every referral.