Cardiovascular Health
·15 min read
Nitric Oxide: The Longevity and Cardiovascular Optimization Molecule You Stopped Making
Nitric oxide built the science of how blood vessels open, won a Nobel Prize, and quietly fades by roughly half before most of us turn fifty. The data on why it matters, and a skeptic's guide to getting it back, measured rather than guessed.
By Tony Medrano, CEO & Founder, LongevityPlan.AI
There is a gas in your bloodstream right now that decides whether your arteries relax or stiffen, whether oxygen reaches your working muscles, and whether the lining of your blood vessels stays smooth or starts collecting plaque. You make less of it every decade. By the time most people reach their forties or fifties, endothelial-function tests suggest they generate only about half the nitric oxide they did in their twenties. Almost nobody notices—until something downstream breaks.
That is an unusual thing to say with confidence in longevity science, a field often long on enthusiasm and short on mechanisms. Nitric oxide (NO) is different. Its biology is not a wellness hypothesis; it is well established enough that three pharmacologists shared the 1998 Nobel Prize for it, and it underpins drugs in cardiac wards and neonatal intensive-care units tonight. So the useful questions are no longer whether NO matters. They are more personal: how much are you making, why your number differs from the person next to you, and what the evidence actually supports doing about it.
This is a brief for the skeptic—the executive who has heard one too many "miracle molecule" pitches, the physician who wants the citation before the claim, the master's athlete chasing another good decade, and the reader who has gained weight, lost a step, or simply wants the next thirty years to be lived rather than merely survived. We will separate the proven from the promising, say plainly what the science cannot yet support, and show how measurement, genetics, and AI turn "eat your vegetables" into an actual plan.
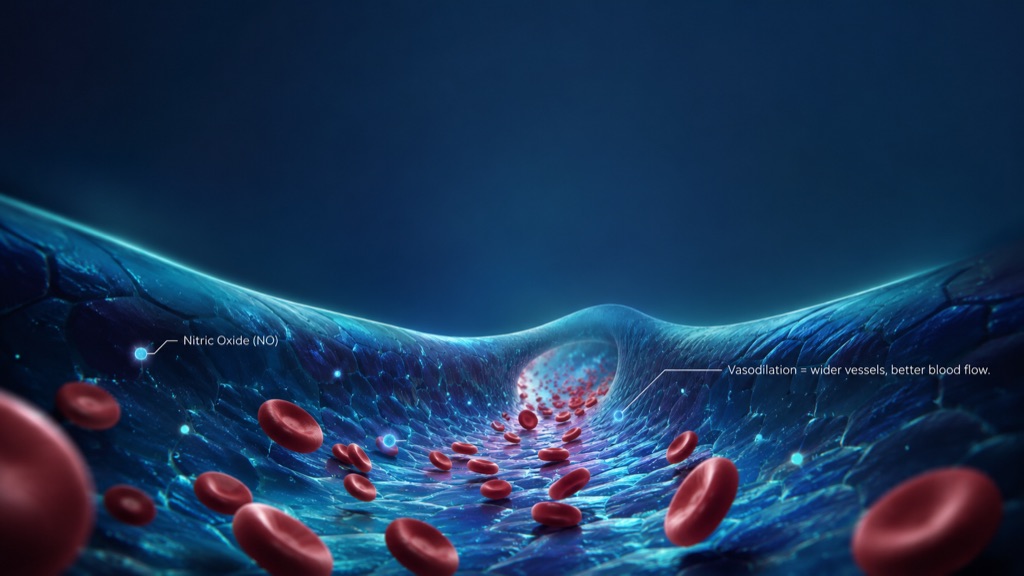
Nitric oxide signals blood vessels to relax and widen, improving circulation and oxygen delivery throughout the body. Production falls by roughly half by age 40–50, making it one of longevity's most overlooked—and most measurable—variables.
An irony of fate
Start with the most famous name in science. In the autumn of 1896, a few weeks before he died, Alfred Nobel—the man whose fortune came from taming nitroglycerin into dynamite—was suffering from angina, the chest pain of a heart starved of blood. His doctors prescribed the remedy of the day: nitroglycerin, taken internally. Nobel found the coincidence almost too much to bear, writing to a friend that it was the irony of fate to be ordered to swallow the very compound he had spent his life detonating. He declined it.
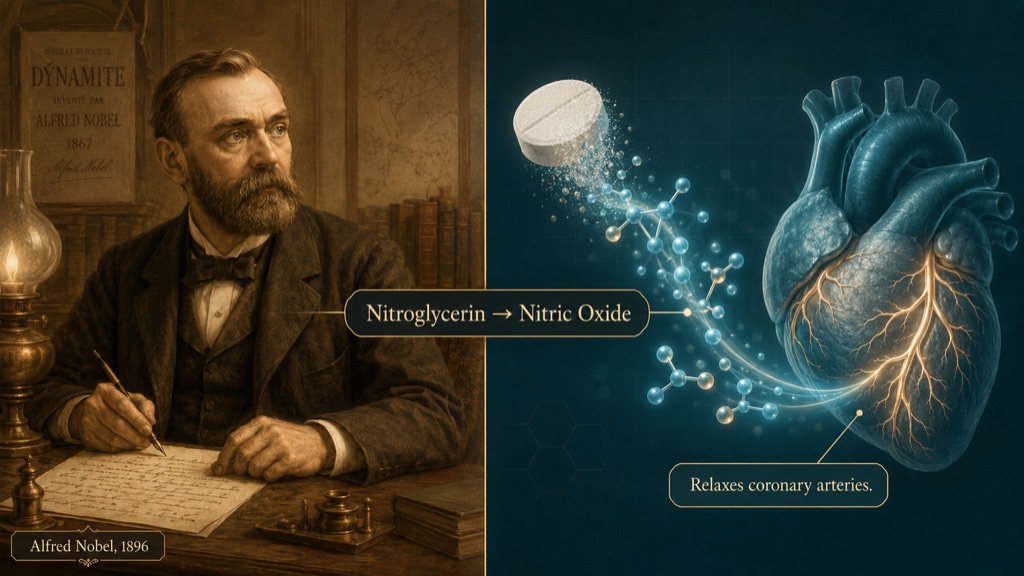
An irony of fate: Alfred Nobel was prescribed nitroglycerin for his failing heart in 1896—never knowing it worked by releasing nitric oxide, the discovery that would win a Nobel Prize a century later.
Nobel never learned why nitroglycerin eased a failing heart. It took another century. Nitroglycerin works because the body converts it into nitric oxide, which relaxes the smooth muscle in blood vessels and allows oxygen-rich blood to flow. Robert F. Furchgott, working in Brooklyn, had spent years puzzled by contradictory results—the same drug relaxing a vessel one day and contracting it the next—until, in 1980, he showed that the difference depended on whether the vessel's delicate inner lining, the endothelium, was intact. He named the unknown culprit "endothelium-derived relaxing factor." Ferid Murad, chasing the same ghost through nitroglycerin's chemistry, had already found in 1977 that it released nitric oxide. Louis J. Ignarro at UCLA closed the loop: the mysterious factor and nitric oxide were one and the same. The Nobel committee called signaling by a gas that crosses from one cell to regulate another an entirely new principle for signaling in biological systems.
A fairness footnote scientists still debate: Salvador Moncada, then at the Wellcome labs in London, made foundational contributions to the identification of NO and was conspicuously left off the prize—proof that even the cleanest scientific stories have contested authorship. But the through-line for a longevity reader is Nobel's irony made literal: the molecule that explained a nineteenth-century heart drug is the same one trending downward in your bloodstream right now.
Two factories, and why one of them lives in your mouth
Your body makes nitric oxide in two ways, and knowing both is the difference between a real plan and folk wisdom.
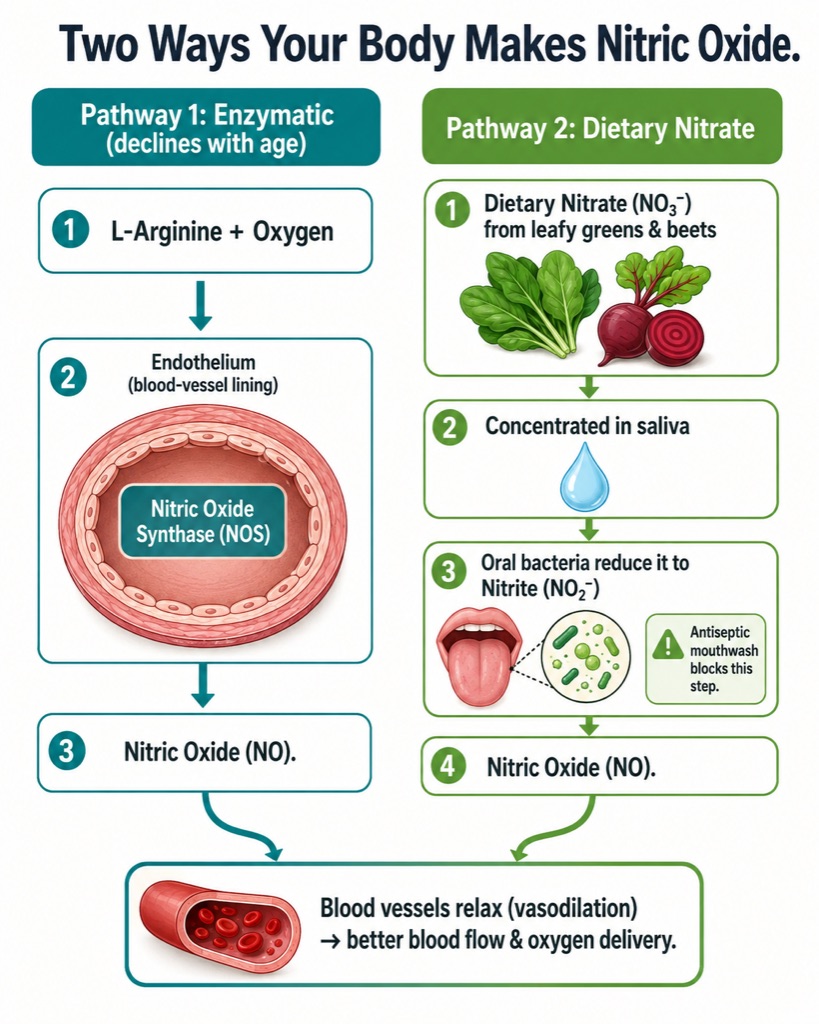
Two ways your body makes nitric oxide: the enzymatic L-arginine/NOS pathway inside your blood vessels, and the dietary nitrate pathway that depends on friendly oral bacteria—which is why antiseptic mouthwash can quietly blunt your levels.
The first is the classical enzymatic route: an enzyme called nitric oxide synthase (NOS) combines the amino acid L-arginine with oxygen to produce NO on demand inside the endothelium. This pathway fails first with age because it depends on healthy endothelial cells and adequate cofactors. Starved of those cofactors, the enzyme "uncouples" and starts producing damaging free radicals instead of NO, which is exactly why simply swallowing more L-arginine so often disappoints. As biochemist Nathan S. Bryan puts it, feeding arginine to someone whose enzyme has broken is like adding fuel to a car with a blown engine.
The second factory is the one most people have never heard of, and it is the best news for prevention. At Karolinska Institutet, Jon O. Lundberg and Eddie Weitzberg established that dietary nitrate—the inorganic kind abundant in beetroot, arugula, and spinach—is not an inert dead end. Their 2008 review in Nature Reviews Drug Discovery, with the University of Maryland's Mark T. Gladwin, mapped the nitrate–nitrite–NO pathway: nitrate you eat is concentrated in your saliva, reduced to nitrite by friendly bacteria on your tongue, then converted to NO—an alternative source that works best precisely where the enzymatic route struggles, in low-oxygen, acidic, hard-working tissue. Jay L. Zweier's 1995 finding that NO could form from nitrite in oxygen-starved heart tissue without any enzyme at all had cracked the door; the Karolinska group walked through it.
The twist that delights audiences and unsettles dentists: this backup factory is outsourced to oral bacteria. Research has since linked antiseptic mouthwash—which scrubs out those nitrate-reducing microbes—to blunted NO production and higher blood pressure. The molecule of cardiovascular youth, it turns out, can be partly undone by the wrong rinse.
The aging curve nobody is tracking
Here is the data that should reframe how you think about your forties. Endothelial function—the vessel lining's ability to make NO—declines on the order of 10 to 12 percent per decade beginning as early as the twenties, so that by age 40 to 50, a typical person produces roughly half their youthful output. A 2025 review of cardiovascular aging frames this declining NO bioavailability as a central driver of the endothelial dysfunction, arterial stiffening, and weakening cardiac performance that define vascular system aging.
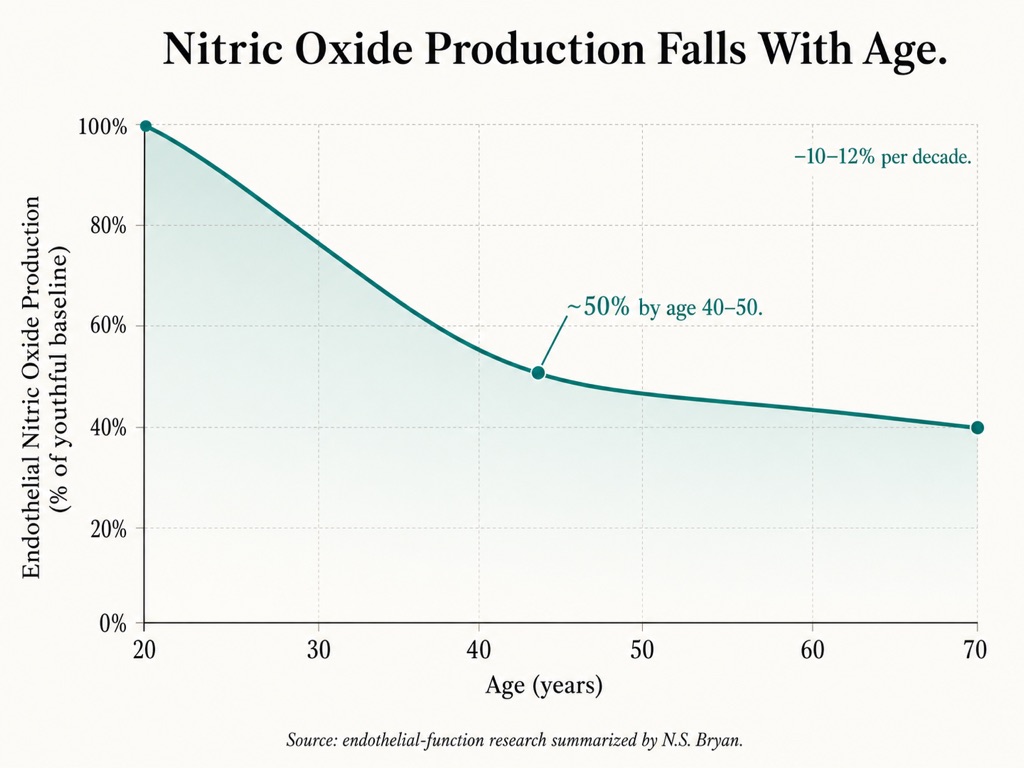
The decline nobody tracks: endothelial nitric oxide production drops about 10–12% per decade, leaving most people at roughly half their youthful output by their forties or fifties.
Why does this matter more than a single lab value? Because the loss of NO shows up before the disease does. When endothelial cells stop making enough of it, adhesion molecules switch on, cholesterol begins to stick and accumulate in the vessel wall, and the slow machinery of atherosclerosis starts—often years before any blockage appears on a scan. Bryan, who has spent nearly three decades on this molecule, calls it the foundational molecule for health and longevity, tying NO deficiency to four shared culprits behind the diseases of aging: reduced blood flow, runaway inflammation, oxidative stress, and immune dysfunction.
None of this requires believing NO is magic. It requires noticing that a measurable, modifiable variable is quietly trending down in nearly everyone, and almost no one is watching it.
What the evidence supports—and what it doesn't
Credibility comes from saying the unglamorous parts out loud, so let us grade the human-trial evidence honestly.
Blood pressure and vascular function: strong
Dietary nitrate reliably lowers blood pressure and improves vascular markers, with larger effects in older adults whose baseline NO is lower. In one crossover study, nitrate-rich beetroot juice produced a bigger rise in plasma nitrite and a bigger blood-pressure drop in adults aged 50–70 than in those aged 18–30—the people with the most to gain responded the most. Even in patients with COPD, a single dose lowered resting diastolic pressure. This is the most robust and most relevant finding for a longevity audience.
Exercise economy: strong, with an honest ceiling
The University of Exeter group—Andrew M. Jones with Stephen J. Bailey, Paul Winyard, the late Nigel Benjamin, and colleagues—showed in a landmark 2009 trial that beetroot juice reduced the oxygen cost of submaximal exercise and extended time to exhaustion by roughly 16 percent. That is genuinely unusual: most interventions make you fitter by making you work harder, while nitrate makes the same work cheaper. Jones, who calls NO essential to life itself, built a career on the principle that anything which helps make people more economical during exercise can lift performance.

Nitrate doesn't make you work harder—it makes the same work cheaper. Beetroot-derived nitrate lowers the oxygen cost of exercise, with the biggest gains in everyday and masters athletes rather than in already-elite athletes.
That science did not stay in the lab. By the time researchers in Sweden and Exeter had published, beetroot shots had become a fixture of elite endurance camps—so mainstream that World Athletics itself now publishes guidance on nitrate and oxygen cost, and double-blind trials have tested beetroot juice in elite distance runners. But the same literature reports the honest ceiling: highly trained endurance athletes with a VO₂max above about 65 ml/kg/min often show little benefit, presumably because their NO systems already operate near optimal. The practical reading is almost the opposite of the usual sales pitch—the deconditioned 55-year-old has far more to gain here than the sub-elite marathoner.
Brain blood flow and cognition: promising but unsettled
Here discipline matters most. Because nitrate boosts cerebral blood flow, it is a plausible cognitive aid, and some acute studies in older adults are encouraging. But a 13-week randomized trial in overweight and obese older adults found that escalating doses of beetroot juice did not meaningfully change cognition or cerebral blood flow. The story is biologically reasonable and commercially tempting; the trial data are mixed. A reader told otherwise is being sold to, not informed.
Proof that this is real medicine
The clearest evidence that NO is a serious therapeutic lever—not a wellness garnish—sits in the hospital, and it loops straight back to Nobel's angina. Inhaled nitric oxide selectively relaxes the blood vessels of the lungs, and since the FDA cleared Mallinckrodt's INOmax in December 1999, it has been the standard of care for newborns with hypoxic respiratory failure, improving oxygenation and reducing the need for ECMO. A condition affecting roughly 2 in 1,000 births is routinely managed today by delivering this molecule one breath at a time.
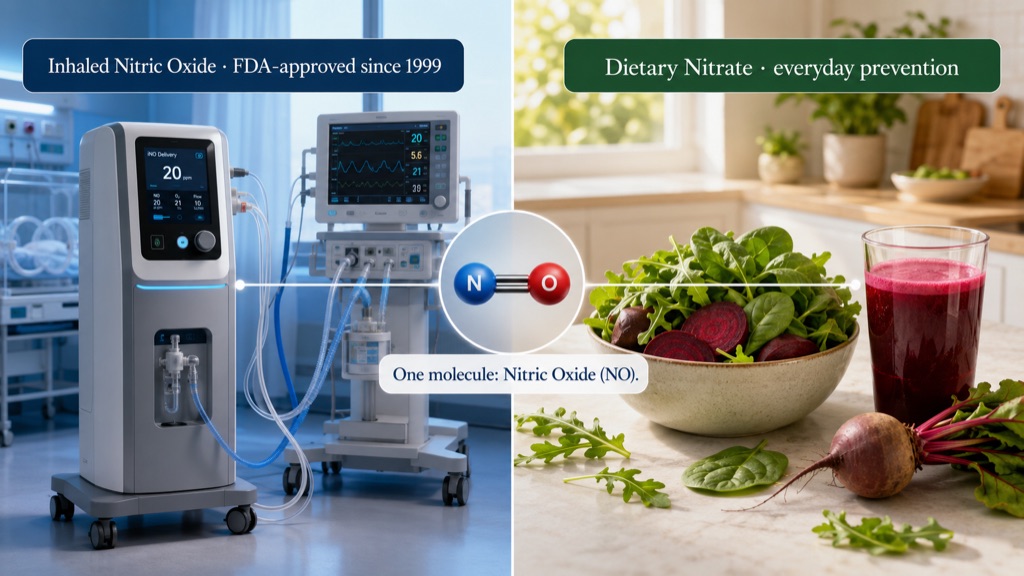
From the ICU to the kitchen: inhaled nitric oxide has been hospital-standard for newborns since 1999—proof that this molecule is real medicine, not just a wellness trend.
The frontier now is engineering. Traditional inhaled NO meant high-pressure gas cylinders and heavy logistics. Two newer companies rewrote that. VERO Biotech's Genosyl, FDA-approved in 2019, is the first tankless delivery system, portable enough to use outside the ICU. Beyond Air went further: its LungFit PH, approved in 2022, generates nitric oxide on demand from ordinary room air, using a plasma chamber that draws about the power of a 60-watt bulb to ionize the nitrogen and oxygen you are already breathing, then filters out the toxic byproduct—no tanks at all. A molecule once delivered from a steel cylinder is now conjured from air on a hospital cart. Meanwhile, Gladwin, now dean at the University of Maryland School of Medicine, has built a body of work on NO's dark mirror: in sickle cell disease, free hemoglobin scavenges nitric oxide, creating a state of NO resistance that underlies international trials still running today.
The takeaway for the skeptic is simple. When the science is strong enough to anchor neonatal intensive care and multinational trials, the consumer-facing version—eat the nitrate, protect the bacteria, watch the number—deserves a serious look rather than a reflexive eye-roll. The question is only how to do it precisely.
The fix isn't a product. It's a system.
This is where LongevityPlan.AI's core argument enters, and it is not a sales pitch—it is an epistemology. Almost everyone's NO is trending down, but the rate, the cause, and the right response differ from person to person. One person eats plenty of greens but has scrubbed their mouth barren with mouthwash; another has the bacteria but lacks the cofactors that keep the enzyme coupled; a third simply inherited a lower baseline. Hand all three the same scoop of beet powder, and you are guessing. A precision approach replaces that guess in three moves: measure, personalize, model.
1. Measure it
Inexpensive saliva test strips from companies such as Berkeley Life and HumanN provide a rough, same-day readout of whether your nitrate-to-NO pipeline is working and let you retest after a change to see whether anything actually moved. They are not laboratory assays, but they convert an invisible variable into a number you can watch—and a number you can watch is a number you can improve. More rigorous endothelial-function testing, increasingly bundled into longevity diagnostics from services like Function Health, Lifeforce, and Superpower, turns "I feel fine" into a tracked trajectory.
2. Personalize it
Two people on an identical protocol can get different results, and increasingly, we can explain why. Common variants in the gene for endothelial NO synthase (NOS3) influence how efficiently the enzymatic pathway runs; cofactor and metabolic variants shape whether that enzyme stays coupled. This is the logic behind genetic pathway testing of the kind offered by The Genomics Company—reading the single-nucleotide variants that govern how your specific biology handles a given input. That genetic layer is the natural foundation for a Digital Twin for Predictive Peptide Performance™: the same vascular, growth-hormone-axis, and GLP-1 loci that shape NO synthesis also shape how individuals respond to Peptide Therapy, so building the model on DNA first means it reasons about your response curve rather than a population average.
3. Model it
Genetics sets the baseline; the rest moves daily, and that is a job for software. A Cardiorespiratory Digital Twin™ is a living model of your physiology assembled from many streams at once. At the sensor layer, wearables track heart rate, variability, sleep, and activity; periodic labs add nitrite, lipids, and inflammatory markers; saliva strips add a direct NO readout. Fusing these into multi-modal health data is harder than it sounds, because each device speaks its own dialect and timescale. The intelligence layer is where it pays off: through predictive modeling, the system can connect a falling NO strip and a creeping blood-pressure trend to the likely culprit—a new mouthwash, a stretch of low-vegetable travel meals, a medication that may be dampening the pathway—and propose the smallest effective change. It flags when you sit in the responder zone and when, like a near-elite athlete, your effort belongs elsewhere. This is decision support, not autopilot: the model surfaces patterns and the Coach / Practitioner and Athlete / Patient decide together, each cycle of data tightening the next call—the mechanism behind genuine AI-powered coaching improvements.
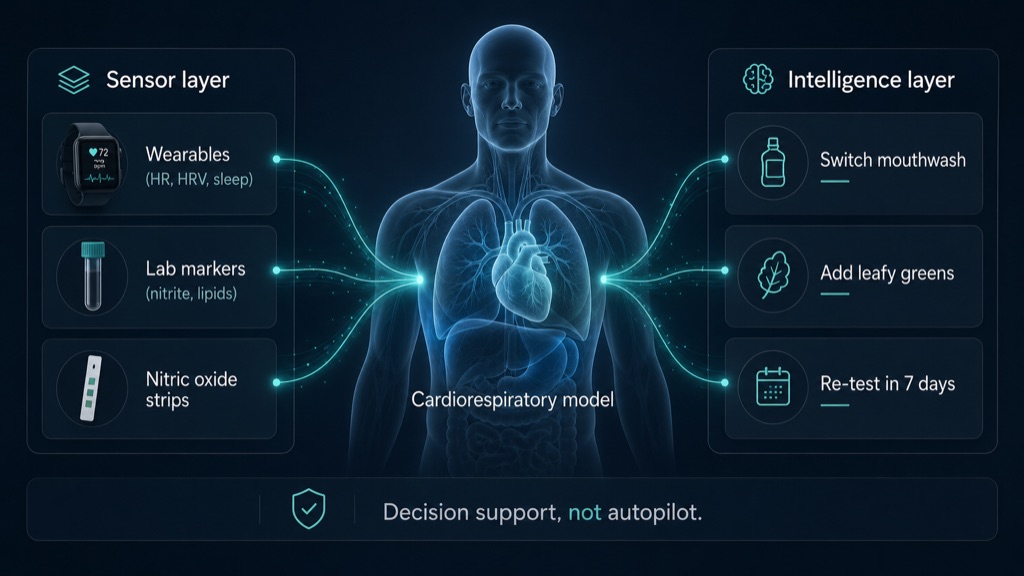
The intelligence layer at work: a living digital model fuses wearables, labs, and nitric oxide readings, then flags the smallest effective change—decision support that a coach and patient act on together, not autopilot.
A skeptic's operating manual
If you take nothing else from this brief, take the checklist. It is deliberately unglamorous.

A skeptic's checklist: food first, supplement the gaps, protect your oral microbiome, rethink L-arginine, and calibrate to your own age, fitness, and genetics.
- Food first. The Exeter studies used beetroot juice because it is a concentrated, reliable source of nitrate, but arugula, spinach, and other leafy greens deliver the same raw material—and whole-food sources appear to beat nitrate salts alone. Eat the rainbow; the green part is doing quite a cardiovascular work.
- Supplement where diet genuinely falls short. Standardized products—Berkeley Life's nitrate capsules, HumanN's SuperBeets and Neo40, Bryan's N1O1 line—exist because hitting consistent nitrate targets through food is hard, and dose consistency is what the trials measured. A tool, not a talisman.
- Protect the bacteria doing the work. Daily antiseptic mouthwash may be undercutting the very pathway you are trying to support—one of the cheapest fixes in the entire field.
- Be wary of L-arginine if you already have vascular issues. When the enzymatic pathway is uncoupled, more arginine can disappoint—the intuitive supplement is the wrong one, and the nitrate pathway is the smarter target.
- Calibrate to yourself. If you are already very fit, temper performance expectations and play the long vascular game; if you are over 40, deconditioned, or carrying extra weight, you are likely in the group that responds most.
Notice what this is not: a promise of reversed aging or a single product that fixes everything. It is a set of measured, individualized adjustments to a variable that genuinely declines and genuinely matters. That restraint is the point—and it is what a thoughtful Peptide Longevity Plan™ is built to deliver, whether for one person or scaled across a Corporate Wellness Program.
The next decade
Nitric oxide is a rare thing in longevity: a target with a Nobel Prize behind it, hospital-grade therapeutics on one end and a grocery-aisle intervention on the other, and a decline curve so consistent it is almost a clock. What has been missing is not the science but the system—a way to know your own number, understand why it is yours, and adjust with precision rather than hope.
That is the shift worth planning for. The reader who measures NO at 45, understands their NOS3 variants, protects their oral microbiome, and lets a model watch the trend is not chasing a fad; they are doing for their cardiovascular system what a pension does for money. Alfred Nobel was given the molecule that could have helped his failing heart, but he turned it down, never knowing what it was. We have no such excuse. The molecule you stopped making is the one you can decide, deliberately and with data, to start making again—and the best time to build that plan, as with most things in a serious Longevity Club, was a decade ago. The second-best time is before the next test strip turns the wrong color.
Sign up for FREE daily Longevity Club Workshops, or join the Affiliate Program (pays 20%).
About the Author
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data and leverages proprietary Digital Twin for Predictive Peptide Performance™ technology, wearable data, and biomarker data to deliver personalized optimization and longevity recommendations. A 3x technology/AI company CEO with 2 successful exits, Tony has completed 3 Full Ironman Triathlons (140.6 mi) since 2019. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University, and has worked with the US Olympic Team, the NBA, NFL, MLB, NASA, Google, Microsoft, and Netflix, among others. He also served as a US Navy Officer commanding an emergency response team aboard a destroyer.
Disclaimer: This article is for educational purposes and is not medical advice, diagnosis, or treatment. Health decisions should be made with a qualified clinician who can interpret your individual results.
Endnotes
- The Nobel Prize in Physiology or Medicine 1998, Press Release and Ceremony materials, NobelPrize.org—awarded to Robert F. Furchgott, Louis J. Ignarro, and Ferid Murad "for their discoveries concerning nitric oxide as a signaling molecule in the cardiovascular system."
- Ferid Murad—1998 Nobel Laureate for Nitric Oxide Research, Mayo Clinic Proceedings (2004); Murad's 1977 work on nitroglycerin and NO.
- Lundberg J.O., Weitzberg E., Gladwin M.T. "The nitrate–nitrite–nitric oxide pathway in physiology and therapeutics." Nature Reviews Drug Discovery 7:156–167 (2008).
- Bailey S.J., Winyard P., Vanhatalo A., Blackwell J.R., DiMenna F.J., Wilkerson D.P., Tarr J., Benjamin N., Jones A.M. "Dietary nitrate supplementation reduces the O₂ cost of low-intensity exercise and enhances tolerance to high-intensity exercise in humans." Journal of Applied Physiology (2009).
- Jones A.M. "Influence of dietary nitrate on the physiological determinants of exercise performance: a critical review." Applied Physiology, Nutrition, and Metabolism 39(9):1019–28 (2014); interview, MySportScience (2015).
- "The power of beetroots," World Athletics (performance guidance on nitrate and oxygen cost); Balsalobre-Fernández C. et al. "The effects of beetroot juice supplementation on exercise economy… in elite distance runners," PLOS ONE 13(7):e0200517 (2018); Jones A.M., Thompson C., Wylie L.J., Vanhatalo A. "Dietary Nitrate and Physical Performance," Annual Review of Nutrition 38:303–328 (2018), on the VO₂max responder ceiling.
- Jones A.M., Gatorade Sports Science Exchange—"Nitric oxide is a gaseous molecule that is essential to life itself."
- Bryan N.S., interview, Preferred Health Magazine; and lecture/podcast remarks on endothelial decline (~10–12% per decade; ~50% by age 40–50) and the limits of L-arginine supplementation.
- "Declining nitric oxide bioavailability in cardiovascular aging: mechanistic insights and emerging interventions." Journal of Cardiovascular Aging (2025).
- Babateen A.M. et al. "Incremental Doses of Nitrate-Rich Beetroot Juice Do Not Modify Cognitive Function and Cerebral Blood Flow in Overweight and Obese Older Adults: A 13-Week Pilot RCT." Nutrients (2022).
- "Acute Supplementation with Nitrate-Rich Beetroot Juice Causes a Greater Increase in Plasma Nitrite and Reduction in Blood Pressure of Older Compared to Younger Adults." Nutrients (2019).
- "Acute Dietary Nitrate Supplementation and Exercise Performance in COPD: A Double-Blind, Placebo-Controlled, Randomised Pilot Study." PLOS ONE (2015).
- U.S. FDA clearance of INOmax (nitric oxide for inhalation), Mallinckrodt Pharmaceuticals, December 1999; indication for term/near-term neonates with hypoxic respiratory failure and pulmonary hypertension.
- VERO Biotech, Genosyl and Genosyl DS, FDA-approved 2019; first tankless inhaled-NO delivery system. American Journal of Respiratory and Critical Care Medicine case report (2020).
- Beyond Air, Inc. (NASDAQ: XAIR), LungFit PH FDA approval, June 2022—on-demand nitric oxide generated from ambient air via the company's Ionizer technology.
- Gladwin M.T., University of Maryland School of Medicine (Dean, 2022– ); research summaries on nitrite, nitric oxide–hemoglobin interactions, and hemolysis-associated endothelial dysfunction.
- Zweier J.L., Wang P., Samouilov A., Kuppusamy P. "Enzyme-independent formation of nitric oxide in biological tissues." Nature Medicine 1:804–809 (1995).
- Lundberg J.O., Weitzberg E., Cole J.A., Benjamin N. "Nitrate, bacteria and human health." Nature Reviews Microbiology 2:593–602 (2004)—the oral microbiome's role in the enterosalivary nitrate pathway.
- Genetic pathway testing of nitric-oxide, growth-hormone-axis, GLP-1 and related signaling variants (e.g., NOS3 polymorphisms) as a basis for individualized response prediction; The Genomics Company (thegenomicscompany.com).
- Salivary nitric oxide indicator strips and standardized nitrate products: Berkeley Life and HumanN (SuperBeets, Neo40) product documentation; at-home test-and-retest use.
- "The Nobel Prize for nitric oxide: the exclusion of Dr. Salvador Moncada," historical review, PubMed (1999); Nicholls M., European Heart Journal 40(22):1747–1749 (2019).
- Alfred Nobel's letter on being prescribed nitroglycerin ("the irony of fate…"), 1896; NobelPrize.org, "Alfred Nobel's health and his interest in medicine," and the 1998 Nobel ceremony speech connecting nitroglycerin to nitric oxide.