Longevity
·16 min read
The Muscle You Keep: How Powerful are GLP-1s + Creatine?
GLP-1 medicines are the most effective weight-loss tools in a century, and they've made creatine and a class of molecules called peptides the most important conversation in longevity. Here's what the data actually say.
By Tony Medrano, LongevityPlan.AI
For most of modern medicine, "losing weight" was a goal so hard to reach that no one worried much about what kind of weight was leaving. That era ended. Semaglutide and tirzepatide now produce weight loss approaching what surgery delivers, at a population scale, and that success has surfaced a question that used to be academic: when the scale drops fast, how much of the loss is fat, and how much is the muscle and bone you spend the rest of your life depending on?
This article is not a market survey and not a sales pitch. It is a practical, evidence-first guide for the reader who is skeptical, over forty, possibly on, or considering, a GLP-1 medicine, and who wants to age with strength rather than simply weigh less. We will follow the data wherever it leads, including when it undercuts the tidiest story. Two unglamorous tools keep recurring in the literature: creatine monohydrate, a compound studied for more than a century, and peptides, a category that ranges from the rigorously proven (GLP-1 itself is a peptide) to the largely unproven and, in many cases, illegal to sell. Sorting one from the other is most of the job.
What the Scale Hides: fat vs. lean mass in GLP-1 weight loss
The number on the scale can't tell you what kind of weight is left. The whole question of muscle-sparing longevity lives in the gap between total weight and body composition, and that gap is where planning earns its keep.
01 / The inflection point: what GLP-1s actually subtract
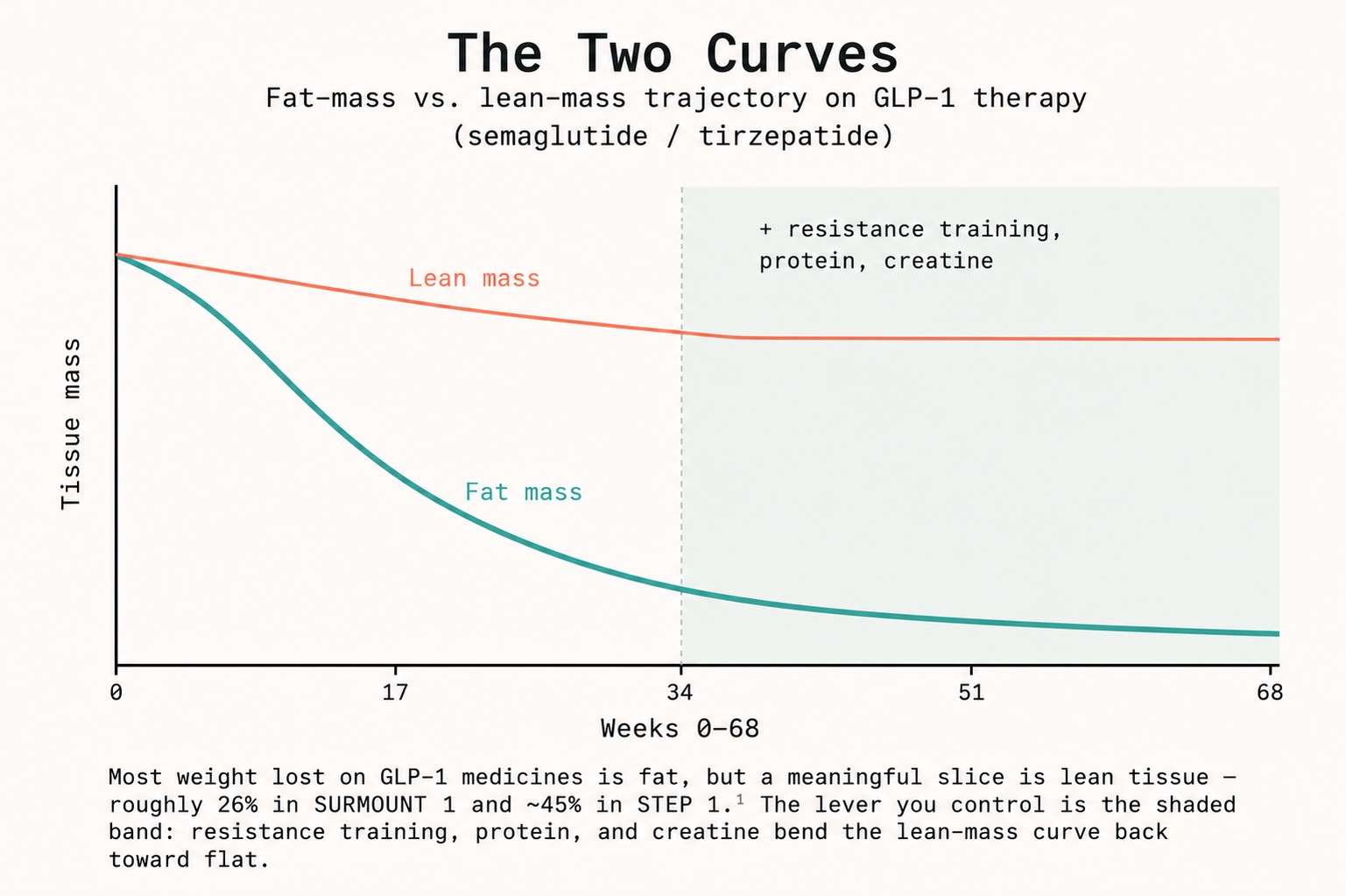
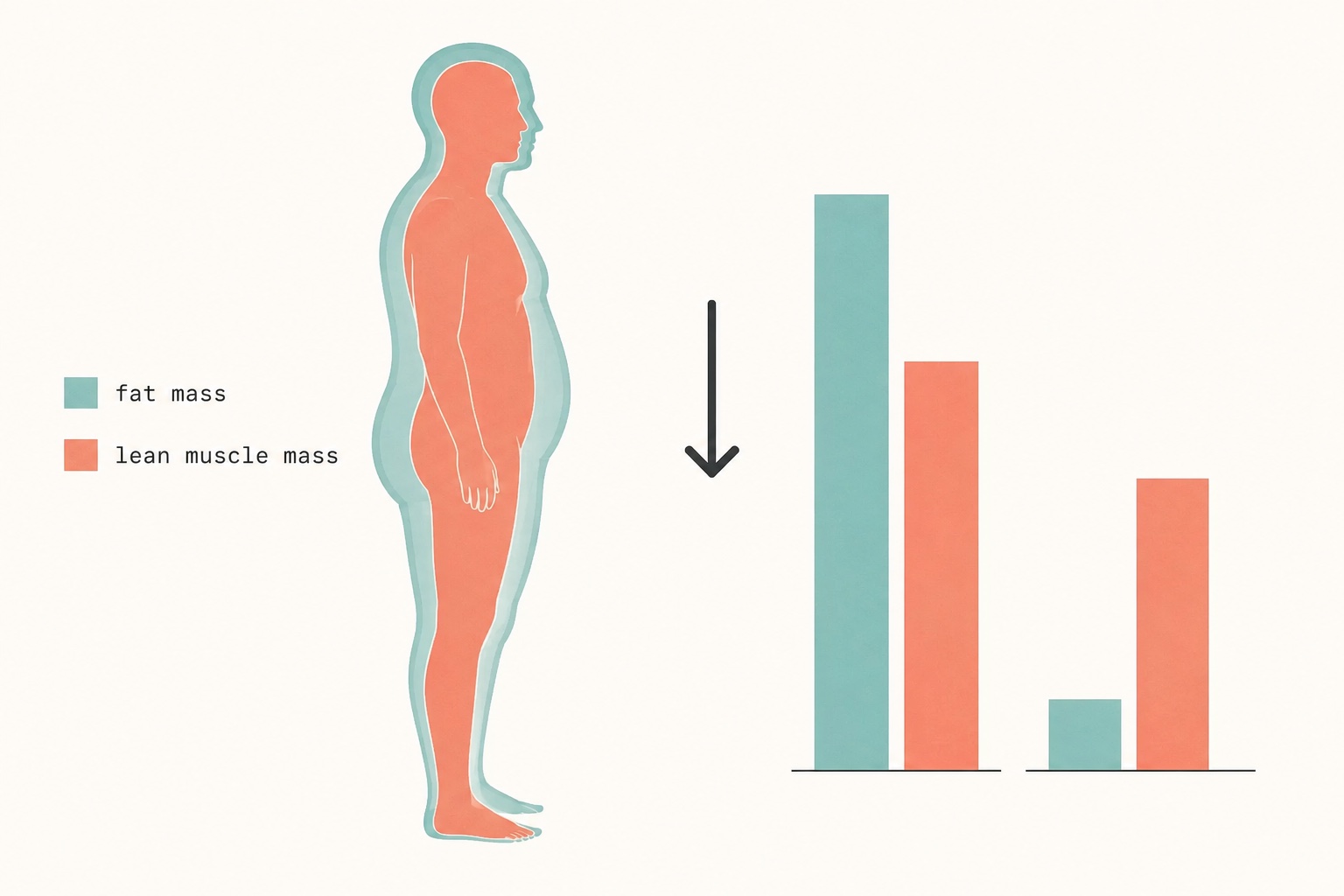
Start with the numbers, because the numbers are where the panic and the reassurance both come from. In the STEP 1 trial of semaglutide, participants lost about 15 kg; of that total, roughly 45% of the weight lost came from lean mass.[1] In SURMOUNT 1, tirzepatide drove larger total weight loss (over 20% at the top dose), but the fraction attributable to lean mass was lower, on the order of 25 to 26%.[1][2] Older agents look worse: liraglutide has been associated with lean-mass loss of up to 60% of total weight lost.[1] Across the major trials, a reasonable summary is that lean tissue accounts for roughly one-quarter to (at the high end) two-fifths of the weight lost.[3]
~45% Fraction of weight lost from lean mass, STEP 1, semaglutide
~26% Fraction from lean mass, SURMOUNT 1, tirzepatide (top dose)
~8% Lean mass adults lose per decade after roughly age 40, unaided
Now the counterweight, because honest reporting requires it. The same primer literature that catalogs those losses stresses that a DEXA "lean mass" reading is a blunt proxy: it does not equal muscle, and it cannot tell you whether the muscle that remains is weaker or simply lighter.[1] In most trials, because fat loss outpaces lean loss, the proportion of the body that is lean tissue actually improves, body composition gets better, not worse.[3][4] A 2026 pre-clinical and proof-of-concept human study in Cell Reports Medicine reported that in obese mice, GLP-1 medicines predominantly reduced fat, that loss of liver mass exceeded muscle loss among lean tissues, and that relative muscle strength and running performance improved even as absolute mass fell.[5] Clinicians at Massachusetts General Hospital have made the measured version of this point: the data do not show GLP-1s causing a uniquely high level of lean-mass loss compared with other routes to the same weight loss; the drugs are one tool among many.[6]
So the alarmist framing ("Ozempic melts your muscle") and the dismissive framing ("it's all just normal") are both wrong. The accurate framing is conditional. Who you are determines whether the muscle loss matters. A 2026 routine-care analysis of more than 670,000 GLP-1 users found that those who lost the most lean tissue were disproportionately people with baseline musculoskeletal pain and reduced exercise tolerance, in other words, the patients least able to defend their muscle in the first place.[7] And the arithmetic of aging is unforgiving: adults already shed up to 8% of lean mass per decade beginning around age 40, so layering rapid pharmacological weight loss on top of that baseline is most consequential for older and frailer people.[8]
The question was never whether GLP-1s reduce lean mass. It is whether your remaining muscle still does its job, and whether you defended it on the way down.
Most weight lost on GLP-1 medicines is fat, but a meaningful slice is lean tissue, roughly 26% in SURMOUNT 1 and ~45% in STEP 1.[1] The lever you control is the shaded band: resistance training, protein, and creatine bend the lean-mass curve back toward flat.
02 / Why muscle is the organ that decides how you age
It is easy to think of muscle as cosmetic. Physiologically, it is closer to an endocrine and metabolic organ that also happens to move your skeleton. Skeletal muscle is the body's largest sink for glucose disposal, a reservoir of amino acids the body draws on during illness, and the single best-correlated tissue with independence in later life. Grip strength and walking speed are among the most durable predictors of all-cause mortality we have. This is why obesity-medicine specialists increasingly frame the goal not as weight loss but as fat loss with muscle and bone preservation, a meaningfully harder target.
The point generalizes well beyond people on medication. The endurance athlete returning from injury, the executive who spent a decade trading training time for travel, the 68-year-old recovering from a hip procedure, and the patient down 40 pounds on tirzepatide are facing the same underlying biology: muscle is built and defended through a combination of mechanical signal (resistance training), substrate (adequate protein), and cellular energy availability. Remove any leg of that tripod, as a strong appetite suppressant can, by quietly cutting protein intake, and the structure weakens. Researchers, including McMaster University's Stuart Phillips and the University of Illinois's Nicholas Burd have spent careers showing that muscle protein synthesis is exquisitely sensitive to protein dose, leucine content, and the presence of a training stimulus, the variables most at risk when total food intake drops.[9]
This is also where the longevity framing earns its keep. The same multimodal health data that flags a falling lean-mass trajectory, a slipping grip-strength reading, a declining step cadence, a drop in logged protein intake, is exactly the data a thoughtful plan would act on before the loss becomes a fall or a fracture. Planning for the downside of an otherwise excellent therapy is not pessimism; it is the entire idea of preventive medicine.
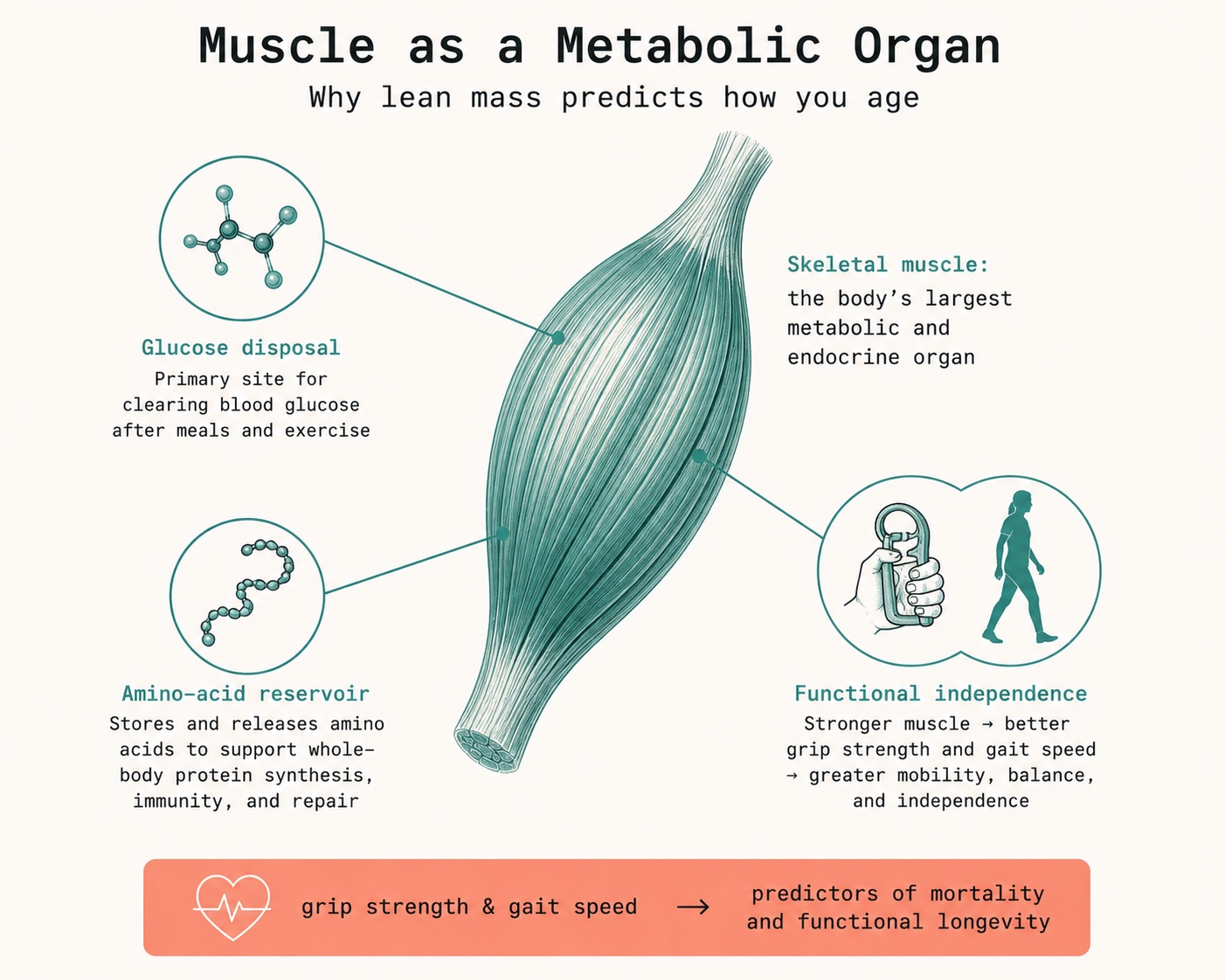
Muscle isn't cosmetic. It is the body's largest glucose sink, its amino-acid reserve, and the tissue most tightly linked to independence in later life, which is why the goal is fat loss with muscle and bone preserved, a harder target than weight loss alone.[9]
03 / Creatine: the most-evidenced lever you're probably under-using
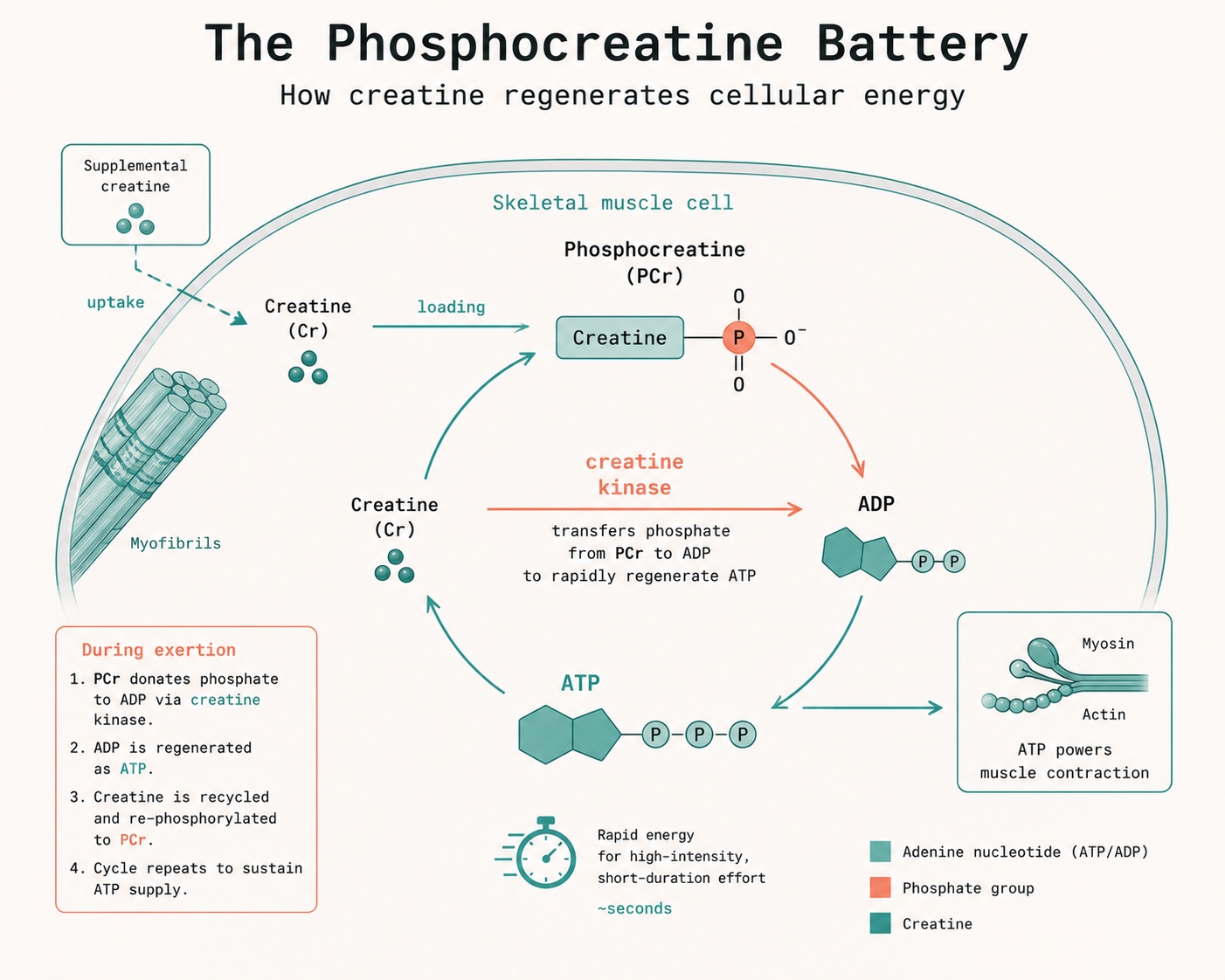
If you set out to design the least glamorous, most reliable muscle-support compound, you would land near creatine monohydrate. It is not a hormone, not a steroid, and, contrary to a myth that refuses to die, not a kidney hazard in healthy people.[10] It is an organic acid your body already makes and stores mostly in muscle, where it buffers the rapid regeneration of ATP, the cell's energy currency. Supplementation raises intramuscular phosphocreatine stores, which lets you do slightly more work in training, and it draws water into muscle cells in a way that supports the signaling environment for protein synthesis.
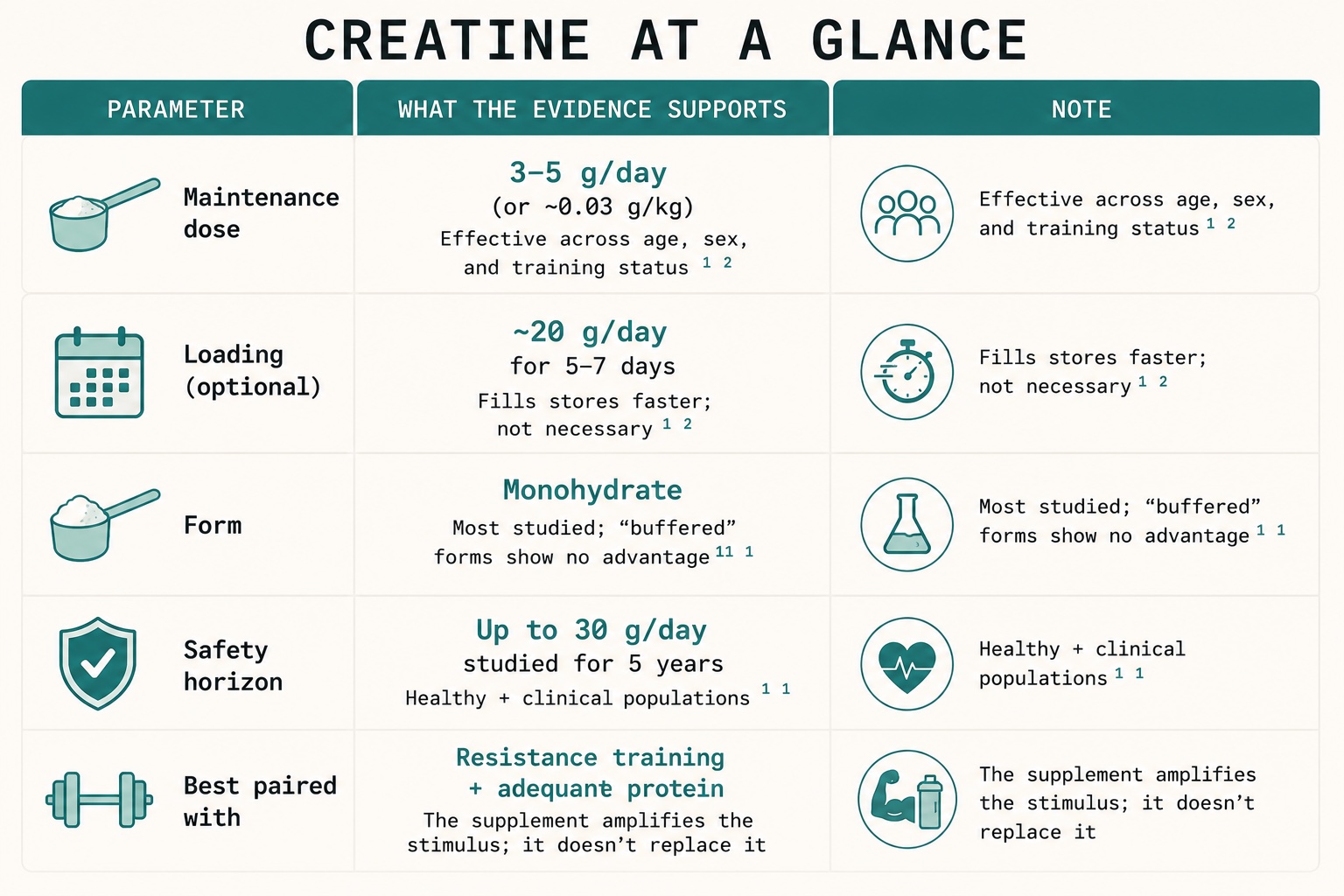
The evidence is unusually mature. The International Society of Sports Nutrition's position stand, authored by a group including Texas A&M's Richard Kreider and the University of Regina's Darren Candow, concluded that creatine monohydrate is the most effective ergogenic nutritional supplement available for increasing high-intensity exercise capacity and lean mass during training, with a favorable safety profile.[11] On dosing, the practical consensus is refreshingly simple: a maintenance dose of 3 to 5 grams per day is effective for almost everyone, an optional loading phase (around 20 g/day for 5 to 7 days) fills stores faster but isn't required, and you would have to eat more than a kilogram of meat to get 5 grams from food.[12] On safety, supplementation up to 30 g/day for as long as five years has been studied without adverse effects in healthy and clinical populations spanning infants to the elderly.[11]
Crucially for an older audience, the benefit is not confined to athletes. A meta-analytic and consensus literature, much of it from Candow, Brandon University's Scott Forbes, and the University of Novi Sad's Sergej Ostojic, supports creatine combined with resistance training to augment lean tissue and strength in older adults, the exact population most exposed to sarcopenia.[13] That convergence, a cheap, safe, lifespan-friendly compound that happens to do most of its work in precisely the tissue GLP-1 patients are trying to protect, is what moved creatine from the gym to the clinic.
04 / Creatine in the GLP-1 era: the mechanistic case (and its honest limits)
In 2026, a perspective paper by Felipe Ribeiro, Scott Forbes, Darren Candow, Chad Kerksick and colleagues did something the field had been circling: it asked, directly and in print, whether creatine can help preserve muscle in people on incretin-based medicines.[14] Their answer is appropriately disciplined. They note that up to 40% of GLP-1-driven weight loss may derive from fat-free mass, that preserving it is an emerging clinical priority, and that creatine, given its established effects on muscle mass, strength, and cellular energetics, is a promising adjunct. They are equally clear about what they are not claiming: there are, as yet, no randomized trials of creatine specifically in GLP-1 users. The mechanistic case is strong; the direct outcome data do not yet exist.[15]
That candor is the point, not a weakness. It is exactly the difference between marketing and science, and it is the standard this newsletter tries to hold. The reasonable read for an individual is this: creatine is low-risk, inexpensive, supported by decades of safety data, and mechanistically aligned with the problem, so the expected value of adding it during a calorie deficit is favorable, provided it sits on top of the two interventions that actually do the heavy lifting.
The hierarchy that the evidence supports
-
Resistance training, 2 to 3 times per week. The mechanical signal that tells the body to keep muscle. Non-negotiable.
-
Adequate protein. Harder to hit when appetite is suppressed; often the first thing that silently falls.
-
Creatine, 3 to 5 g/day. The amplifier, cheap, safe, and aligned with the goal, but an add-on, not a substitute for the first two.
A 2025 joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association and The Obesity Society codified the lifestyle layer: strength training at least three times weekly plus at least 150 minutes of aerobic activity, alongside protein-forward nutrition, for patients on incretin therapy.[16]
It is worth noting why this matters commercially as well as clinically, because the two are converging. A wave of pharmaceutical programs now explicitly targets muscle preservation alongside GLP-1s, combinations pairing incretins with myostatin/activin, apelin and related pathways from companies including Eli Lilly, Novo Nordisk, Regeneron, BioAge Labs, and others, plus selective agents such as bimagrumab studied in combination with semaglutide.[3][17] When Lilly, Novo, Amgen, Pfizer, and AbbVie are all spending to defend lean mass, the signal is unambiguous: the industry agrees the muscle question is real. The individual's version of that strategy, train, eat protein, supplement creatine, and measure, is available today, at a rounding error of the cost.
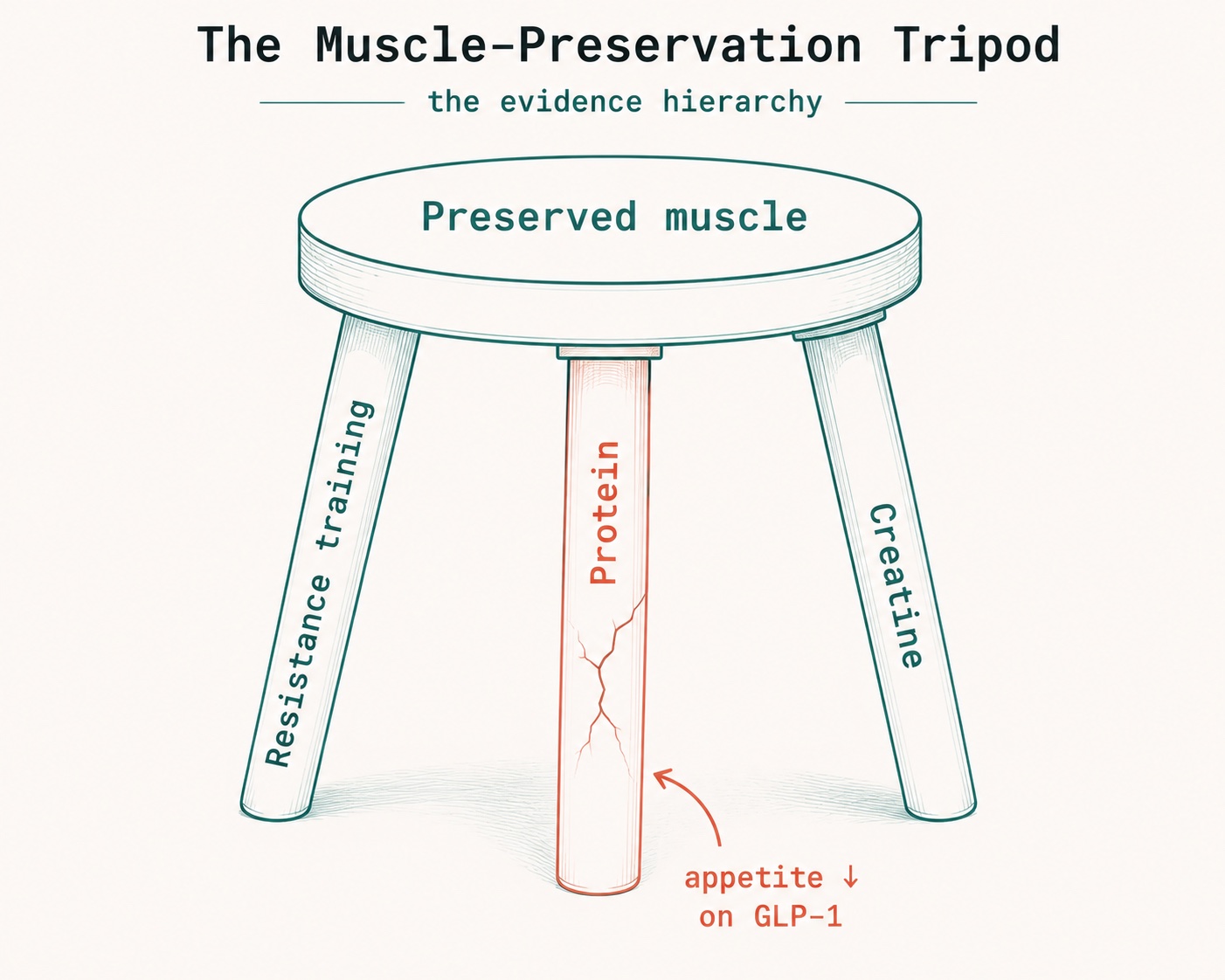
The order is the message. Training and protein do the structural work; creatine is the amplifier on top. Because appetite suppression quietly erodes protein intake first, that leg is the one most likely to crack, which is exactly where a measured plan intervenes.[14][16]
05 / Above the neck: creatine, brain energy, and what the data don't yet prove
Muscle is the headline, but creatine's second act is the brain, another tissue that runs hot on ATP and stores phosphocreatine. The interest here is older than the supplement aisle: a landmark 2003 trial by Caroline Rae and colleagues reported that six weeks of creatine improved working memory and a fluid-reasoning task in a sample that included many vegetarians, whose baseline creatine intake is low.[18] More recently, a 2024 study by Gordji-Nejad and colleagues found that a single high dose of creatine changed cerebral high-energy phosphate metabolism and reduced the cognitive deterioration that comes with sleep deprivation, a result of obvious interest to executives, clinicians, and anyone who flies through time zones.[19]
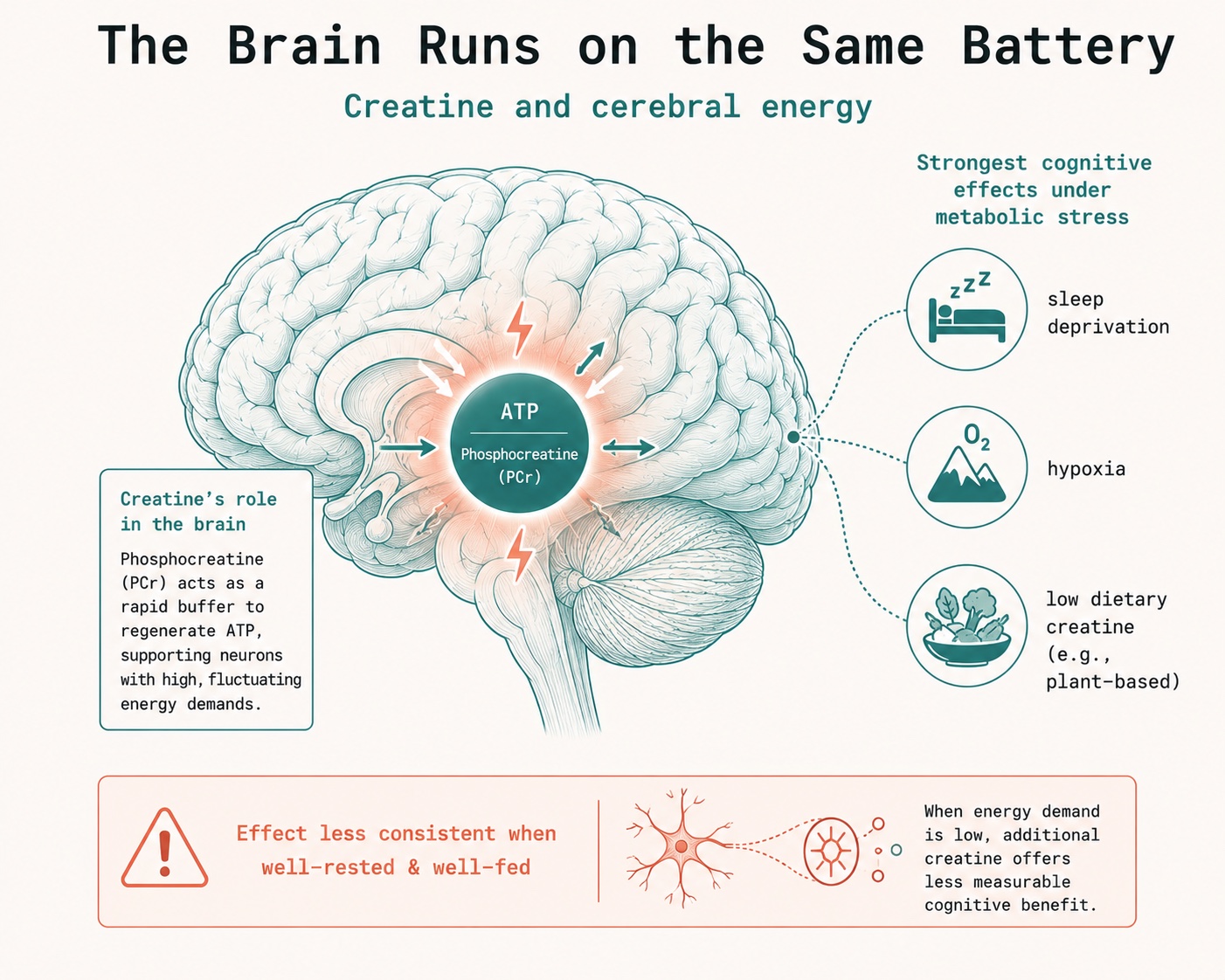
The brain stores phosphocreatine too. Creatine's cognitive benefit is most consistent under metabolic stress, sleep loss, hypoxia, or low baseline intake, and far less certain in the well-rested and well-fed. Promising, not yet settled.[18][20]
Here is where discipline matters again. The cognitive evidence is most consistent under metabolic stress, sleep loss, hypoxia, mental fatigue, or low baseline intake, and far less consistent in well-rested, well-fed people.[20] At least one systematic review has argued the cognitive literature does not yet support a robust general effect, and European regulators have declined to authorize a broad cognition health claim, citing methodological limits in the underlying studies.[20][21] The honest summary: creatine's brain story is biologically plausible and genuinely promising, especially for the sleep-deprived and the plant-based, but it is not yet the settled science that its muscle story is. We flag the gap rather than paper over it, which is the whole reason to read evidence-first writing instead of a supplement label.
06 / The peptide question: signal, hype, and the 2026 rulebook
"Peptide" has become one of the most abused words in wellness, so a definition helps: a peptide is simply a short chain of amino acids. By that definition, the single most successful drug class of the decade, the GLP-1 receptor agonists, are peptides, developed on the foundational biology worked out by scientists including the University of Toronto and Sinai Health's Daniel J. Drucker and the University of Copenhagen's Jens Juul Holst.[22] That is the category at its best: rigorous mechanism, large randomized trials, regulatory approval, and, in Drucker's more recent work, newly mapped anti-inflammatory actions that may help explain GLP-1's benefits well beyond the pancreas.[22]
Then there is the gray market, and the contrast could not be sharper. The repair-and-recovery peptides that dominate biohacking forums, BPC-157 and TB-500 chief among them, have intriguing preclinical data and almost no controlled human trials.[23] Their regulatory status in 2026 is unambiguous and worth stating plainly, because the marketing rarely does:
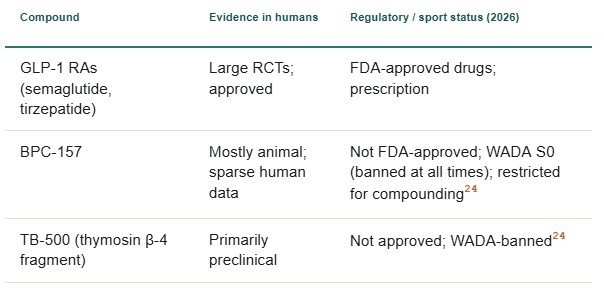
The specifics matter for the exact reader this article serves. For the competitive or tested athlete, BPC-157 and TB-500 sit in WADA category S0, prohibited at all times, and athletes have drawn multi-year bans on non-analytical evidence alone; the U.S. Department of Defense lists BPC-157 as prohibited for service members.[24] For everyone, supply is a problem independent of biology: independent analyses have found mislabeling, incorrect dosing, or contamination in roughly 30% of gray-market peptide samples, and most are sold as "research chemicals" not intended for human use.[24] The regulatory ground is also shifting in real time, an FDA advisory committee is slated to review several peptides in July 2026, and public statements from federal officials have signaled openness to restoring compounding access for a defined list, but as of this writing, the legal status is restrictive, and the human evidence base remains thin.[25] The orthopedic and sports-medicine community is treating this with appropriate caution: the American Orthopedic Society for Sports Medicine is convening experts at its 2026 annual meeting precisely because demand has outrun the data.[26]
Interesting animal data is not the same as proven human therapy. The gap between them is exactly where careful planning lives.
— The consensus position across 2026 sports-medicine commentary
The takeaway is not "peptides are bad." It is that "peptide" spans a vast quality range, and the responsible move, for an Athlete / Patient and for the Coach / Practitioner advising them, is to treat any Peptide Therapy as a prescription-grade medical decision made under supervision with eyes open to evidence, legality, and supply quality, not as a supplement-aisle impulse.
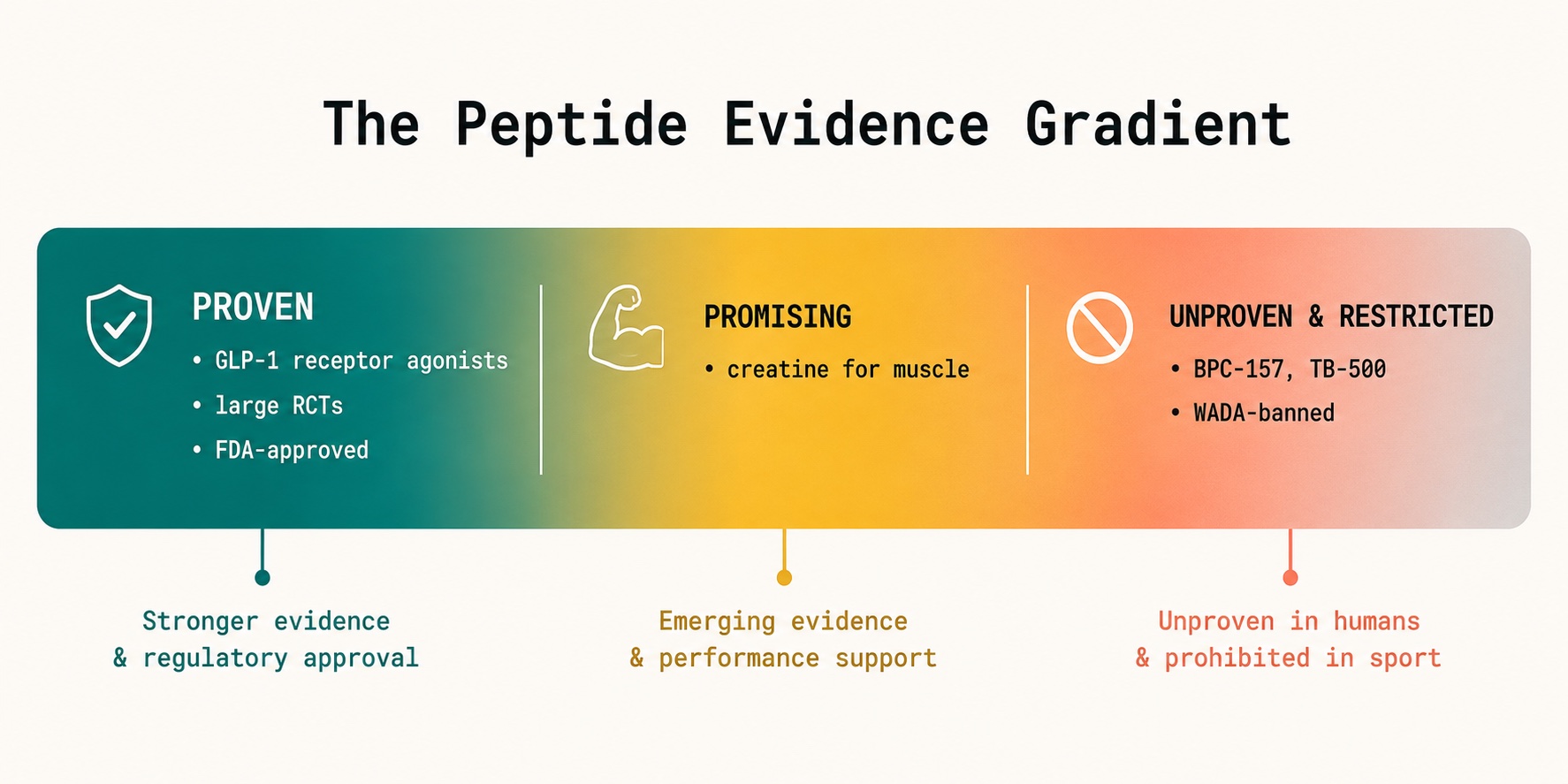
"Peptide" is a category, not a verdict. GLP-1 agonists sit at the proven end with large randomized trials and approval; the repair-peptide gray market sits at the other, mostly preclinical data and prohibited for tested athletes.[24][26]
07 / The buyer's guide: turning all of this into a plan
Everything above is generic until it meets a specific person. The skeptical executive, the masters-category cyclist, the post-surgical 70-year-old, and the patient eight weeks into tirzepatide need different versions of the same logic. A useful plan is built in layers.
Measure before you medicate, and keep measuring
The cheapest mistake in this whole field is acting without a baseline. A defensible starting panel pairs body composition (DEXA or a validated bioimpedance proxy) with function (grip strength, gait speed, a sit-to-stand) and the inputs you control (protein intake, training frequency). This is the sensor layer, the raw, multi-modal health data stream from wearables, labs, and simple in-clinic tests. On its own, it is just numbers. Its value comes from what sits above it.
Translate data into decisions
The intelligence layer is where measurement becomes a plan: where a falling lean-mass slope plus a quietly declining protein log triggers a specific intervention, add a resistance session, raise protein to a target, confirm the 3 to 5 g creatine dose, rather than a vague resolution to "eat better." This is the function of predictive modeling: not to predict the future mystically, but to flag the trajectory early enough that a small adjustment prevents a large loss.
Sequence the levers by evidence, not by novelty
The order is the message. Training and protein first, because they do the work. Creatine next, because it is cheap, safe, and aligned. Prescription pharmacology, including GLP-1s for those who medically qualify and any supervised Peptide Therapy, under a clinician, with the evidence and legal status honestly named. Novelty is not a reason to move something up the list; evidence is.
This is, in miniature, what a Peptide Longevity Plan™ should be: not a list of exotic injections, but a measured, sequenced, supervised strategy in which the proven tools carry the load and the experimental ones are treated with the skepticism they have earned. The same architecture scales from an individual to a Corporate Wellness Program, an employer protecting the functional capacity of an aging, high-value workforce, or to a Longevity Club of members who want their plan managed with the rigor a sports franchise applies to its athletes.
08 / How AI changes the unit of analysis from "average" to "you"
Every statistic in this article is an average, and no one is the average. STEP 1's "45% of weight lost from lean mass" is a population mean that hides enormous individual variation, the 2026 routine-care data showed some patients sliding into a depletive pattern while others preserved muscle entirely, which was largely separable by baseline pain, exercise tolerance, and behavior.[7] The entire promise of AI-driven longevity planning is to collapse that gap: to model your trajectory from your data, not the cohort's.
This is the work of a Cardiorespiratory Digital Twin™, a continuously updated virtual model of an individual's physiology that fuses wearable data streams, lab panels, body composition scans, and training logs into a single representation that can be queried and projected forward. Extended to the muscle-and-medication problem, a Digital Twin for Predictive Peptide Performance™ does something concrete: it simulates how an individual's lean-mass trajectory is likely to respond to a given GLP-1 dose, training frequency, protein target, and creatine protocol, and flags, in advance, whether this person is heading toward the preservation pattern or the depletion pattern, while there is still time to change the inputs.
The same model is what turns a coach's intuition into AI-powered coaching improvements: a Coach / Practitioner sees not a wall of dashboards but a ranked, evidence-weighted set of the few changes most likely to bend this Athlete / Patient's curve. The drug-discovery side of the industry has already industrialized this logic, Eli Lilly, Novo Nordisk, and AI-native firms use machine learning to design and screen the next generation of muscle-sparing molecules, and the consumer-facing tier of the market is racing to bring the same data fusion to individuals. Platforms such as Function Health, Superpower, and Lifeforce have built large followings by establishing comprehensive measurement routines; the frontier now is the intelligence layer that turns those measurements into a personalized, predictive, supervised plan.
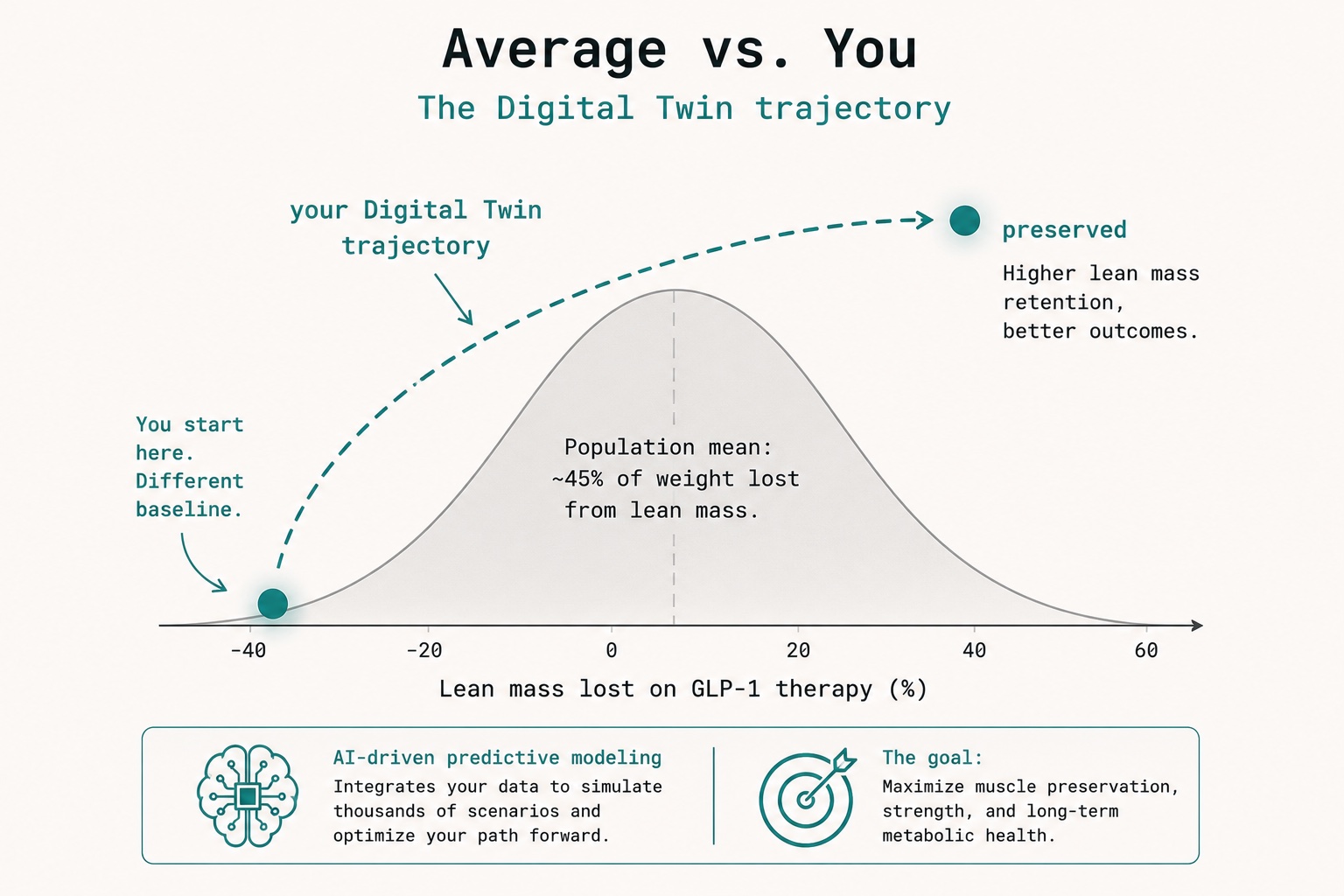
No one is average. A Digital Twin for Predictive Peptide Performance™ models your lean-mass trajectory from your data, flagging the depletion pattern early enough to change the inputs while it still matters.[7]
The honest bottom line
GLP-1 medicines are a genuine breakthrough, and the muscle question they raised is real but manageable. Creatine monohydrate is the rare intervention that is cheap, century-tested, safe, and pointed at exactly the right tissue, a near-default for most people training through a calorie deficit, with a promising-but-unsettled brain story on top. Peptides are a category, not a verdict: GLP-1 is the proof of what rigorous peptide science delivers, and the repair-peptide gray market is the cautionary tale of what happens when demand outruns evidence and law. And the through-line connecting all of it is measurement: the person who tracks lean mass, protein, and strength, and acts on the trend early, keeps the muscle. The person who waits for the number on the scale to look right often does not. Planning, in other words, is the intervention. Everything else is a tool it picks up.
Sign Up for the LongevityPlan Affiliate Program (Pays 20%)
About the Author
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data from athletes and leverages proprietary Digital Twin for Predictive Peptide Performance™ technology, wearable data, and biomarker data to deliver personalized performance optimization and longevity recommendations to athletes, coaches, organizations, businesses, government, and the military. In addition to being a 3x technology / AI company CEO with 2 successful exits, Tony has also finished 3 Full Ironman Triathlons (140.6 mi) since 2019. He has degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University.
Tony has been involved with AI and molecular diagnostic start-ups for 10 years, and also worked with the US Olympic Team, National Basketball Association (NBA), National Football League (NFL), Major League Baseball (MLB), Iditarod, FBI, NASA, U.S. Department of Health and Human Services (HHS), Google, Microsoft, Netflix, Bridgewater Associates, ConocoPhillips, British Petroleum, One Medical, and Jenny Craig, Inc. to provide technology, artificial intelligence and/or molecular diagnostics solutions to their employees.
One of Tony's prior companies provided Conversational AI to health, fitness, and wellness companies; another delivered access to digital libraries of British Petroleum for oil discovery; and his first was a mobile app platform funded by Softbank, which resulted in a case study published by Stanford University Press, and was taught in multiple MBA programs for a decade. Tony loves to teach and mentor; he earned public school teaching credentials in NY and MA and taught inner-city high school students to give back to the underprivileged community in Harlem. He also lectured on entrepreneurship and venture capital to second-year MBA students at Stanford Business School for five years. He co-authored one of the first issued patents for mobile applications. Tony also served as a US Navy Officer commanding an emergency response team on a USN Destroyer. Tony's military-to-CEO career has recently been chosen to air on an episode of "Operation CEO" a documentary by InsideSuccess.TV, which will air on AppleTV, Prime Video & Amazon MGM Studios, YouTubeTV, and other major platforms worldwide in 2026.
#Longevity #Healthspan #GLP1 #Semaglutide #Tirzepatide #MusclePreservation #Sarcopenia #Creatine #Peptides #PrecisionMedicine #DigitalTwin #PreventiveMedicine #ObesityMedicine #ResistanceTraining #Biohacking #AIinHealth #ExecutiveHealth #LongevityPlanAI
Endnotes & sources
Every figure and attribution below was checked against the linked primary or near-primary source. Where the science is contested, both sides are cited deliberately.
- Neeland IJ, et al. "Muscle Mass and Glucagon-Like Peptide-1 Receptor Agonists: Adaptive or Maladaptive Response to Weight Loss?" Circulation (2024). STEP 1 fraction of weight lost from lean mass ~45%; SURMOUNT 1 ~25.7%; liraglutide up to 60%; caveats on lean mass as a proxy. ahajournals.org
- Neeland IJ, et al. "Changes in lean body mass with GLP-1-based therapies and mitigation strategies." Diabetes, Obesity and Metabolism (2024). Trial-by-trial lean-mass fractions. dom-pubs.onlinelibrary.wiley.com
- "Semaglutide and GLP-1: Effects on lean body mass still unclear" (industry overview of STEP/SURMOUNT body-composition data and muscle-preserving drug programs), Drug Discovery Trends (2024). drugdiscoverytrends.com
- "GLP-1s and Lean Mass: What the Research Shows," American Council on Exercise / Univ. of Hong Kong Mendelian-randomization analysis (2025): fat-mass reduction exceeds lean-mass reduction, improving overall body composition. acefitness.org
- "Weight loss with GLP-1 medicines does not result in a disproportionate loss of muscle mass or function in obese mice and humans." Cell Reports Medicine (2026): liver-mass loss exceeds muscle loss among lean tissues; relative strength and running performance improve. cell.com
- "Preserving Lean Body Mass in Patients Taking GLP-1 for Weight Loss," Massachusetts General Hospital, Advances in Motion (2025): GLP-1s not shown to cause uniquely high lean-mass loss vs. other weight-loss routes; exercise + protein best preserve mass. advances.massgeneral.org
- "Greater lean-body-mass decline with tirzepatide than semaglutide in routine care," medRxiv (2026): 670,422 GLP-1 users; baseline musculoskeletal pain and reduced exercise tolerance predict greater lean-mass loss; depletive metabotype defined. medRxiv 2026.04.11.26350687
- Haines M, et al., reported at ENDO 2025, via Healio (2025): adults lose up to ~8% of lean mass per decade from ~age 40; older adults, frailty, and low bone density flagged as higher-risk subgroups on GLP-1s. healio.com
- Representative bodies of work on protein dose, leucine, and the training stimulus for muscle protein synthesis: Stuart Phillips (McMaster University) and Nicholas Burd (University of Illinois). See ISSN protein and creatine position stands for synthesis. jissn.biomedcentral.com
- Antonio J, et al. "Common questions and misconceptions about creatine supplementation." J Int Soc Sports Nutr (2021): creatine is not a steroid/hormone and does not damage kidneys in healthy people. jissn.biomedcentral.com
- Kreider RB, Kalman DS, Antonio J, Ziegenfuss TN, Candow DG, et al. "ISSN position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine." J Int Soc Sports Nutr (2017): most effective ergogenic supplement for high-intensity capacity and lean mass; up to 30 g/day for 5 years studied without adverse effects. PMC5469049
- "Protein and Creatine Supplements Are No Longer Niche," Medscape (2026): 3 to 5 g/day effective for almost everyone; >1 kg of meat needed to obtain ~5 g from diet; 12 to 40% lean-mass range in GLP-1 weight loss. medscape.com
- Bonilla DA, Stout JR, Candow DG, Forbes SC, Ostojic SM, Kreider RB, et al. "The power of creatine plus resistance training for healthy aging." Frontiers in Physiology (2024): consensus that creatine + resistance training enhances muscle and function across age. frontiersin.org
- Ribeiro F, Forbes SC, Candow DG, Kerksick C, et al. "Creatine supplementation for preventing muscle atrophy in patients taking incretin-based pharmacotherapies: a perspective." Journal of Nutritional Physiology / ScienceDirect (2026): up to 40% of GLP-1 weight loss may be fat-free mass; creatine a promising adjunct. sciencedirect.com
- Commentary on the Ribeiro/Candow/Forbes perspective noting it is a mechanistic perspective, not a trial; GLP-1-specific creatine RCT data do not yet exist. jenerise.com
- Joint advisory, American College of Lifestyle Medicine / American Society for Nutrition / Obesity Medicine Association / The Obesity Society (2025): strength training 3 or more times weekly plus 150 or more min/week aerobic activity and protein-forward nutrition for patients on incretin therapy (summarized via Healio). healio.com
- "New GLP-1 Therapies Enhance Quality of Weight Loss by Improving Muscle Preservation," American Diabetes Association, 85th Scientific Sessions (2025): BELIEVE study of bimagrumab + semaglutide; lean mass 15 to 40% of total weight loss. diabetes.org
- Rae C, Digney AL, McEwan SR, Bates TC. "Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial." Proc Biol Sci 270:2147-2150 (2003). Working memory and Raven's matrices improved (5 g/day, 6 weeks). PubMed 14561278
- Gordji-Nejad A, et al. "Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation." Scientific Reports 14:4937 (2024). nature.com
- Xu C, et al. "The effects of creatine supplementation on cognitive function in adults: a systematic review and meta-analysis." Frontiers in Nutrition (2024); and counterpoint systematic review questioning a robust general cognitive effect. frontiersin.org / sciencedirect.com
- EFSA Panel opinion: creatine and improvement in cognitive function, health claim not authorized owing to methodological limitations in the supporting study. PMC11574456
- Daniel J. Drucker, discovery of the biological actions of GLP-1 (University of Toronto; Sinai Health / Lunenfeld-Tanenbaum Research Institute; awards incl. Wolf Prize 2023, Breakthrough Prize 2025); recent work mapping GLP-1 anti-inflammatory mechanisms. GLP-1 biology also foundational to Jens Juul Holst (University of Copenhagen). en.wikipedia.org/wiki/Daniel_J._Drucker
- Vasireddi N, et al. "Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review," HSS Journal (2025); and reviews noting BPC-157 evidence is predominantly preclinical. PMC11859134
- "What's Changing With Peptide Regulation in 2026," Banned Substances Control Group (2026): BPC-157 and TB-500 in WADA class S0 (prohibited at all times); DoD prohibition; ~30% of gray-market samples mislabeled/contaminated; sold as "research chemicals." bscg.org. See also USADA: usada.org/bpc-157
- "FDA July 2026 Peptide Meeting" (advisory review of BPC-157, TB-500 and others; Category 2 compounding status; reinstatement under consideration), Meto (2026); and reporting on federal signals toward restoring compounding access for a defined peptide list. meto.co
- "The Boom of Peptides in Sports Medicine: Do We Know Anything More?" American Orthopaedic Society for Sports Medicine, Sports Medicine Update (Spring 2026); STOP Sports Injury peptide education at the 2026 AOSSM Annual Meeting, Seattle. sportsmed.org
- Tirzepatide vs. semaglutide head-to-head body-composition context (SURMOUNT-5, 2025; Wegovy HD 7.2 mg approval, March 2026): proportional lean-mass loss is similar between agents and tied to magnitude of total weight loss. clinicalnutritioncenter.com
Editorial & medical note. This article is for education, not medical advice. Creatine, protein targets, GLP-1 medicines, and any peptide therapy should be discussed with a qualified clinician, particularly for anyone with kidney disease, on multiple medications, pregnant, or competing under anti-doping rules. Figures cited are population averages and may not reflect any individual's response. The regulatory status of peptides was accurate as of June 2026 and is actively changing. Cardiorespiratory Digital Twin™, Digital Twin for Predictive Peptide Performance™, and Peptide Longevity Plan™ are marks of LongevityPlan.AI.
Earn while you share. Join the LongevityPlan Affiliate Program and earn 20% on every referral.