Peptide Science
·16 min read
The Collagen Comeback
What injectable peptides and biostimulators can, and can't, do for aging skin, and how genomics and AI turn guesswork into a plan.
By Tony Medrano, LongevityPlan.AI
If you are over 40, successful, and faintly annoyed every time a "youth-restoring peptide" ad interrupts your podcast, this article is written for you. Not because the science is fake — some of it is unusually good — but because the gap between what a molecule does in a fibroblast culture and what a syringe does to your face is where most marketing lives, and where most money is wasted. The goal here is to close that gap with data.
The aesthetic-injectables market has quietly become one of the most data-rich corners of preventive medicine. The same fibroblast that builds your skin builds your tendons and the matrix around your heart, so the biology of "looking older" turns out to be a readable proxy for the biology of being older. What follows is a buyer's guide, not an investor's deck: how the leading injectable peptides and collagen biostimulators actually work, who responds to them and why your genes have a vote, how the major companies differentiate, and how a personalized, sensor-and-genome-driven model can tell you whether any of it is worth your time before you book the appointment.
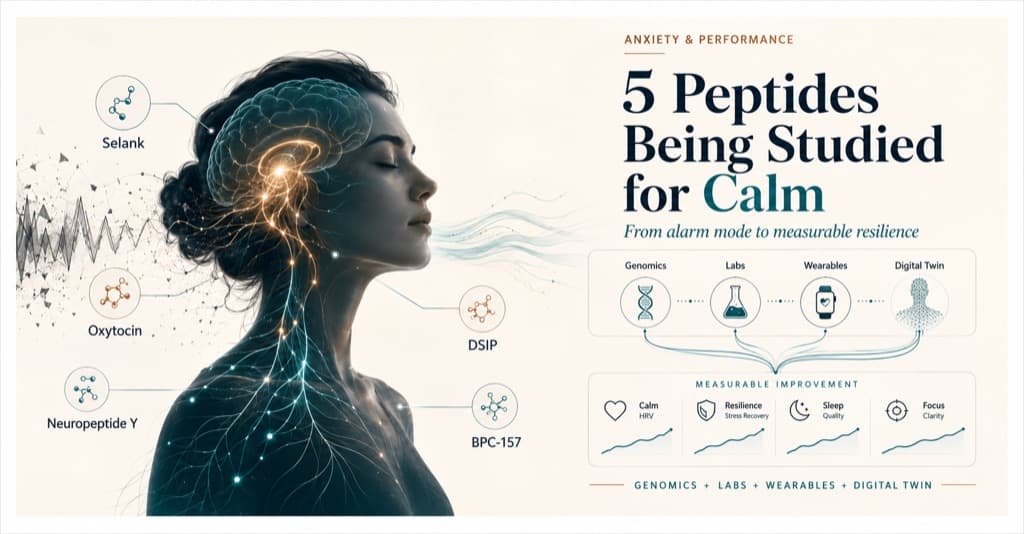
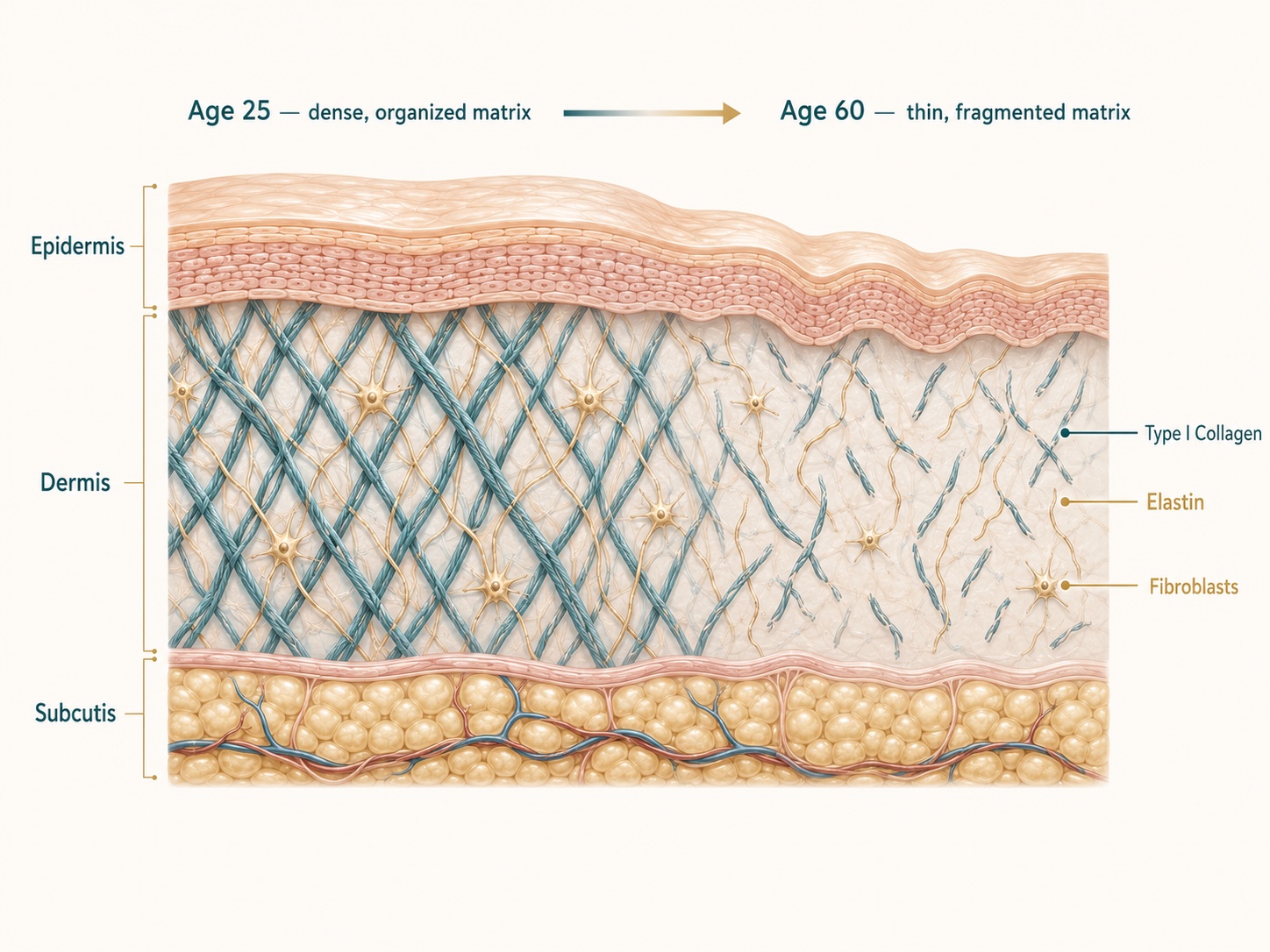
Figure 1. How Skin Loses Collagen With Age: The Dermal Matrix Explained
Skin is mostly collagen-rich connective tissue built by fibroblasts. With age, the type I collagen scaffold thins and fragments — the visible result is fine lines, laxity, and crepiness.
1. Why Skin Collagen Collapses — The Mechanism Worth Understanding First
Skin is mostly a collagen-rich connective tissue, produced and maintained by dermal fibroblasts.[1] The single most useful mental model of skin aging comes from Gary J. Fisher, the Harry Helfman Professor of Molecular Dermatology at the University of Michigan, who has spent three decades dissecting how that matrix falls apart.[2] His group's central finding is deceptively simple: in aged skin, the enzyme matrix metalloproteinase-1 (MMP-1) is chronically elevated, and MMP-1 initiates the fragmentation of type I collagen fibrils that give skin its strength.[3]
The elegant part is the feedback loop. Fibroblasts are mechanically attached to intact collagen, much like a tent staked to firm ground. When collagen fragments, the fibroblast loses its anchor, retracts, and collapses — and a collapsed fibroblast makes less new collagen and more MMP-1.[4] The Michigan team calls this "fibroblast collapse," and they have shown the cycle is self-reinforcing: damaged collagen begets oxidative stress, which begets more MMP-1, which begets more damage.[5] To prove causation rather than correlation, the group engineered a mouse expressing human MMP-1 in its skin fibroblasts; at six months, it spontaneously developed the hallmarks of aged human skin — fragmented collagen, contracted fibroblasts, reduced collagen output.[6]
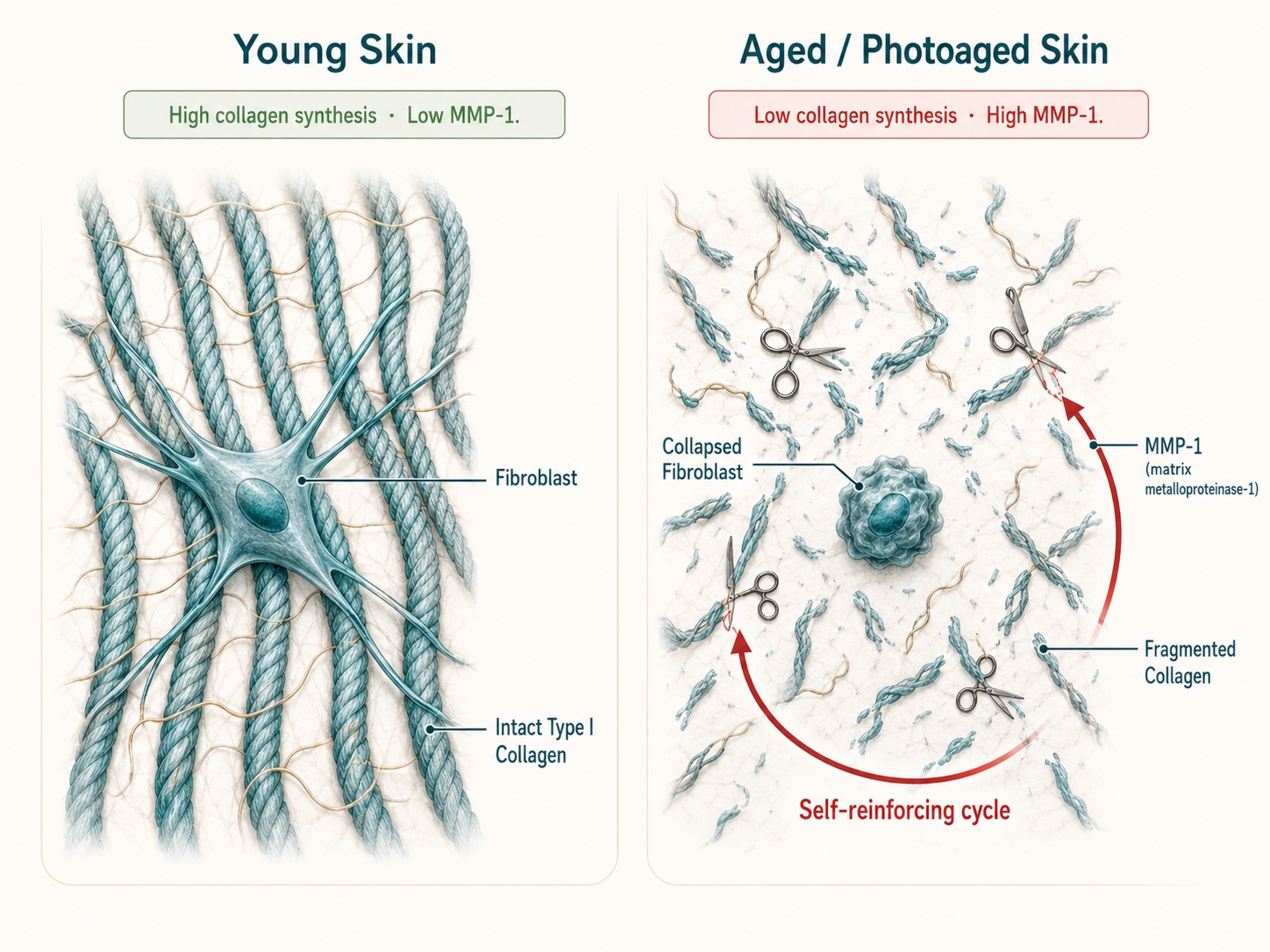
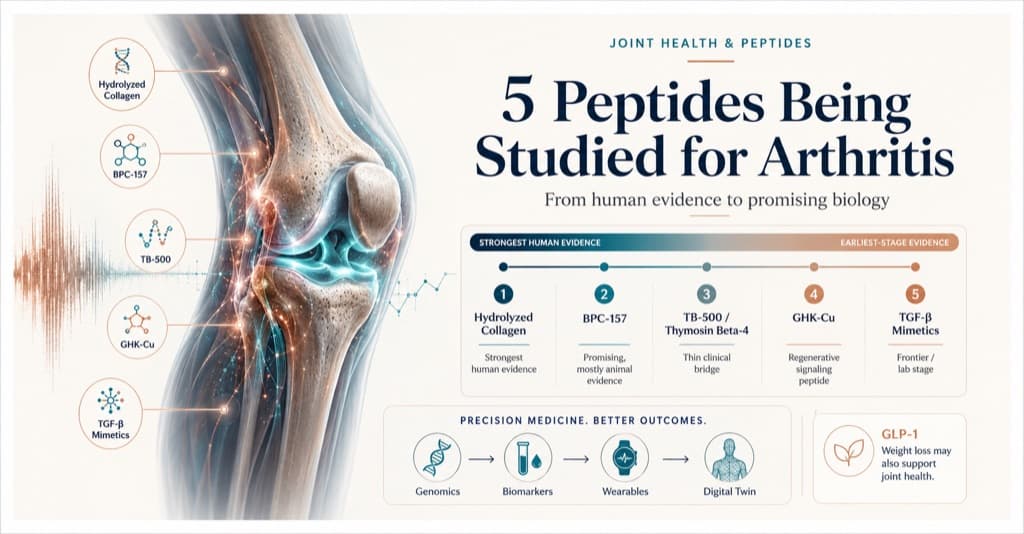
Figure 2. The Fibroblast Collapse Cycle: How MMP-1 Drives Skin Aging
The "fibroblast collapse" model: once collagen fragments, fibroblasts lose their anchor, retract, and make less collagen and more MMP-1 — a loop that feeds itself. Re-stretching the cell or adding fresh matrix is how injectables interrupt it.
The practical implication: any intervention that re-stretches fibroblasts or supplies fresh structural matrix can, in principle, restart collagen production. This is the mechanistic logic shared by microneedling, biostimulatory fillers, and several injectable peptides.
This is also why a beautiful counterpoint exists in science. The Michigan group and longtime collaborator Sewon Kang — now chair of dermatology at Johns Hopkins — documented years ago that topical retinoic acid (vitamin A) stimulates collagen accumulation in naturally aged human skin, the first proof that the collapse is partly reversible with the right signal.[7] Injectable approaches are, in a sense, more aggressive versions of that same idea: deliver the signal directly to the dermis.
2. The Reason "What Works for Her Won't Work for You": Your Genes Have a Vote
Here is the uncomfortable fact that the before-and-after photos never mention. Two people can receive the identical injection and get measurably different results, and a meaningful share of that difference is written in their DNA. The collagen system is governed by genes that vary substantially across individuals.
On the build side, the COL1A1 and COL1A2 genes encode the chains of type I collagen, and common polymorphisms in these loci affect skin structure and elasticity.[8] On the demolition side, promoter variants in the MMP1 and MMP3 genes raise baseline collagen-degrading activity; in the German SALIA cohort of older women, these variants tracked with a shared susceptibility to both skin wrinkling and lung aging — the same demolition enzyme, two organs.[9] Researchers have begun pooling these variants into polygenic risk scores for wrinkle severity, demonstrating that genetic load interacts with menopause, UV exposure, and even hydration to set an individual's trajectory.[10]
This matters for peptide response specifically. If your MMP1 promoter runs hot, a biostimulator that builds collagen is fighting a faster demolition crew, and your maintenance interval should be shorter. If your TGF-β/Smad signaling — the pathway that switches on COL1A1 and switches off MMP1 — is genetically blunted, the same product may underperform.[11] Pharmacogenomics adds a second layer: how you metabolize the carrier, clear the byproducts, and handle copper or nucleotide loads is also heritable.
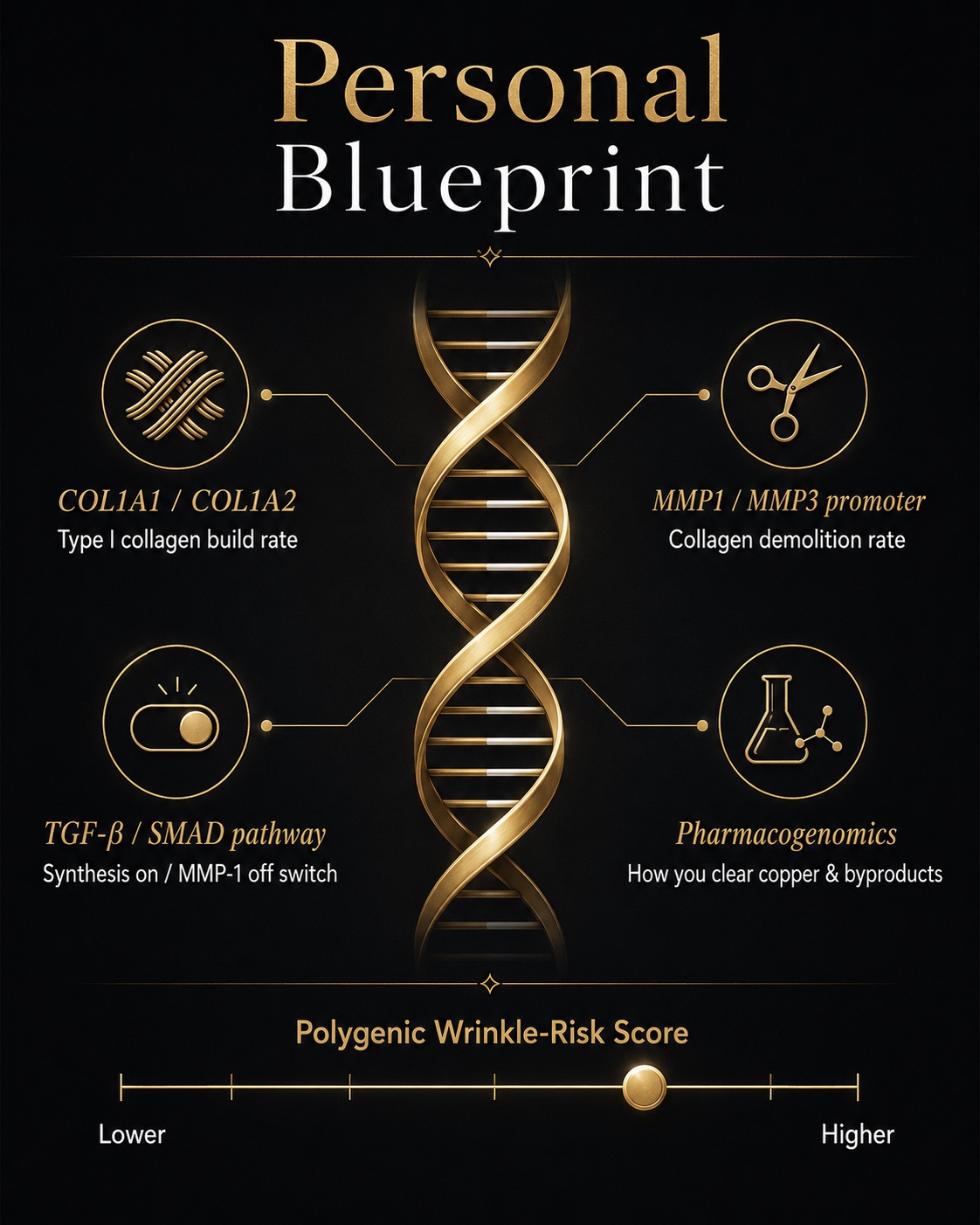
Figure 3. The Genes That Control Skin Collagen: COL1A1, MMP1, and Your Wrinkle Risk Score
Your collagen destiny is partly genetic. Variants in collagen-building genes (COL1A1), collagen-degrading genes (MMP1), and the TGF-β signaling switch combine into a polygenic risk score — and help predict who responds to which injectable, and how often.
This is where genomic profiling stops being a novelty and becomes a planning tool. Saliva-based services such as The Genomics Company position genomic interpretation as the missing input that explains "why certain diets never worked for you" — and the same logic applies to why a given injectable will or won't earn its place in your regimen.[12] A baseline genome is the natural foundation for what LongevityPlan.AI calls a Digital Twin for Predictive Peptide Performance™: a model that ingests your fixed genetic blueprint and then layers in changeable data to forecast response before a needle is involved. We will return to how that twin is built.
3. The Injectable Toolkit: A Buyer's Guide by Mechanism
"Injectable peptides for wrinkles" is a marketing umbrella covering at least four distinct mechanisms, with very different evidence quality. A skeptical buyer should sort them by what they actually do to the dermis, not by brand.
3a. Copper Peptides (GHK-Cu): The Genome Re-Setter
GHK-Cu (glycyl-L-histidyl-L-lysine) is a tripeptide that occurs naturally in human plasma, where its concentration falls from roughly 200 ng/mL at age 20 to about 80 ng/mL by age 60 — a decline that parallels the loss of healing capacity.[13] Bound to copper as GHK-Cu, it was first characterized by biochemist Loren Pickart. The French group of Maquart demonstrated that at vanishingly low, non-toxic concentrations (1–10 nanomolar), GHK-Cu stimulates both the synthesis and the controlled breakdown of collagen and glycosaminoglycans, behaving as a master regulator of remodeling rather than a blunt growth signal.[14]
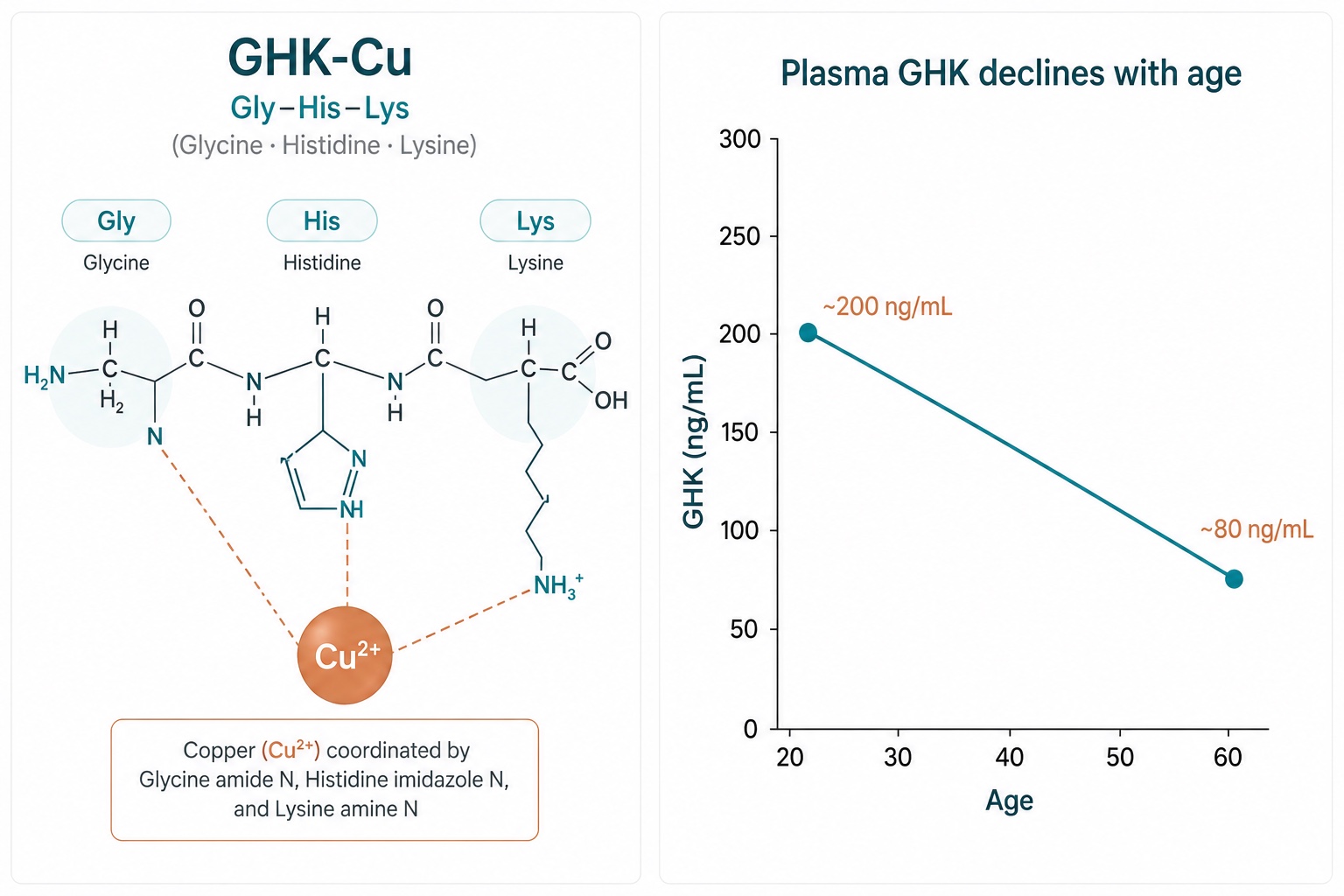
Figure 4. GHK-Cu Copper Peptide Structure and Its Decline With Age
GHK-Cu is a naturally occurring copper-binding tripeptide (Gly–His–Lys + Cu²⁺). Plasma levels fall from about 200 ng/mL at age 20 to roughly 80 ng/mL by 60 — part of why healing and collagen renewal slow down.
The headline claim — that GHK-Cu can "reset" gene expression toward a younger state — has a real basis. Gene-profiling analysis attributed to Pickart and Margolina found that GHK influences the expression of a large fraction of human genes, shifting damaged or aged cells toward a more youthful pattern.[15] The honest caveat: the strongest GHK-Cu evidence is topical and cosmetic. In a controlled study, a GHK-Cu cream improved skin density and reduced fine lines and laxity over 3 months in women with photoaging.[16] Injectable and mesotherapy GHK-Cu protocols are widely offered but rest on a thinner randomized-trial base, and copper peptides can paradoxically upregulate MMPs at certain doses — the so-called "copper uglies" reported anecdotally.[17] A data-first stance: GHK-Cu is real biology with good topical evidence and promising but immature injectable evidence.
3b. Polynucleotides and PDRN: Salmon DNA as a Fibroblast Fuel and Signal
The fastest-growing category in 2026 is also one of the more elegantly mechanistic. Polynucleotides (PN) and polydeoxyribonucleotides (PDRN) are purified, fragmented DNA chains — derived from salmon or trout — that do two things at once. They serve as raw nucleotide "building blocks" that fibroblasts use directly via the DNA salvage pathway, and they act as agonists at the A2A adenosine receptor, triggering a signaling cascade that upregulates collagen and elastin synthesis, dampens inflammatory cytokine levels, and improves microcirculation via VEGF.[18] Structural support and receptor-level signaling in one molecule, which distinguishes PDRN from simpler hydrators.[19]
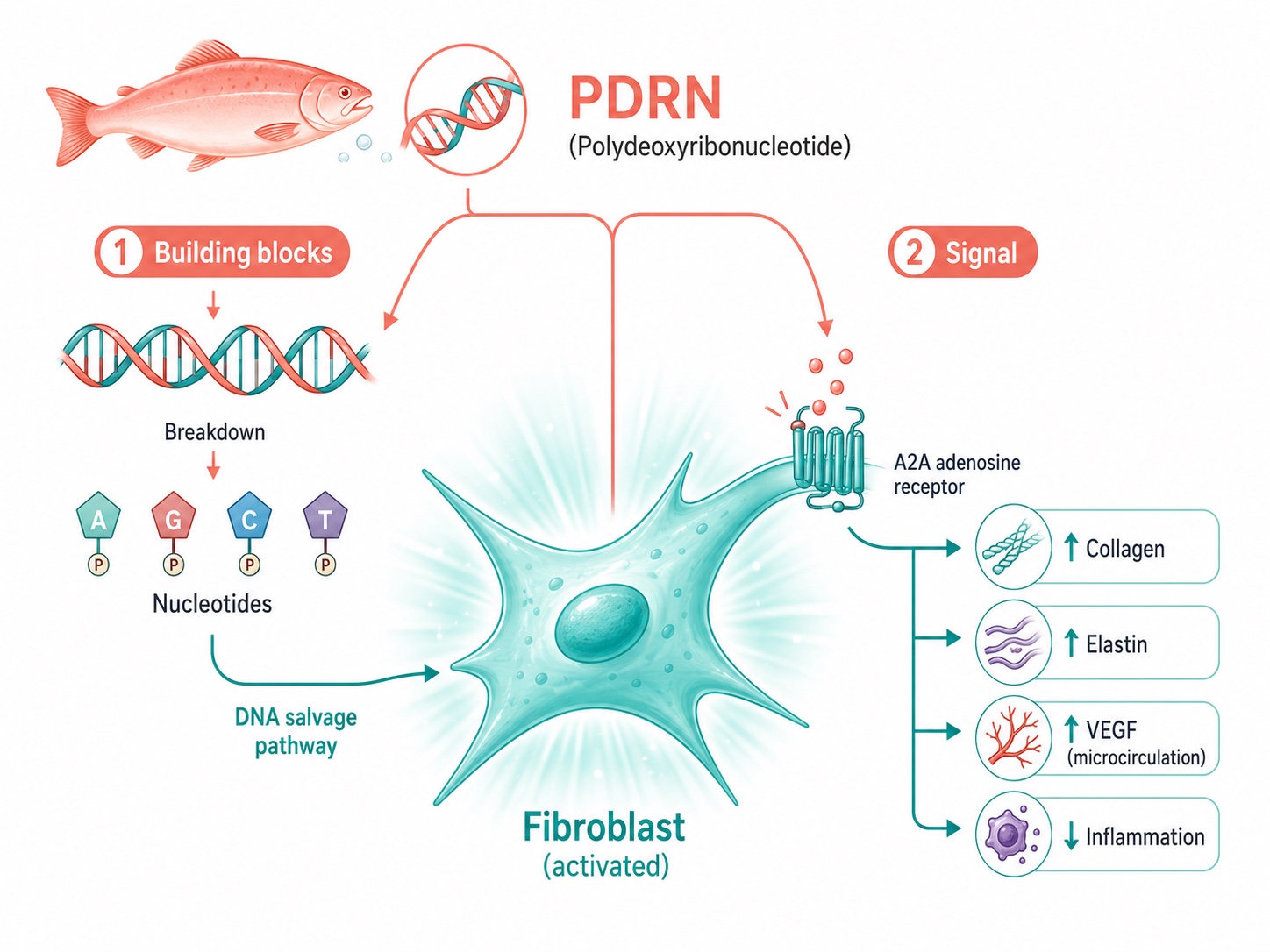
Figure 5. How PDRN (Salmon DNA) Polynucleotides Stimulate Fibroblasts: Dual Mechanism
Polynucleotide injectables work two ways at once: purified salmon or trout DNA supplies raw nucleotides fibroblasts reuse to build collagen, while activating the A2A adenosine receptor to boost collagen, elastin, and blood supply — and calm inflammation.
The category's pedigree is unusually deep. The Italian biopharmaceutical company Mastelli pioneered polynucleotide therapeutics decades ago and markets the Plinest line using a proprietary high-purification process (PN-HPT) that strips out immunogenic proteins.[20] Clinically, the PDRN series of three to four sessions produces dermal-density gains measurable by 20 MHz high-frequency ultrasound, with collagen remodeling continuing for months after the final session.[21] Competitors have crowded in: South Korea's PharmaResearch (Rejuran) popularized salmon-DNA PN across Asia, and Promoitalia's Nucleofill family targets specific zones such as the delicate under-eye. In several major markets, salmon-DNA "skin boosters" are now reported as the most-requested injectable after botulinum toxin — a striking shift away from the overfilled hyaluronic-acid look toward biological regeneration.[22]
3c. Hyaluronic-Acid Bioremodeling (Profhilo): The Scaffold That Wakes the Cell
Not every injectable that builds collagen is a "peptide," and the skeptical buyer should know the difference. Profhilo, from Italy's IBSA Derma, is pure hyaluronic acid — but stabilized by a patented thermal process (NAHYCO) that links high-molecular-weight HA (1,100–1,400 kDa) and low-molecular-weight HA (80–100 kDa) into hybrid cooperative complexes without chemical crosslinkers, at a high concentration of 64 mg per 2 mL syringe.[23] Rather than adding volume, it spreads horizontally through the dermis and re-establishes matrix homeostasis. In vitro, the hybrid complex raised the expression of type I, III, IV, and VII collagens and elastin beyond what either HA fraction achieved alone.[24] A systematic review of nine studies covering 278 participants supports its effect on laxity, elasticity, hydration, and density, and worldwide postmarketing data across more than 40,000 treated patients describe a reassuring safety profile.[25] It is included here precisely because it is the cleanest example of "scaffold biology" — give the fibroblast something to grip, and it gets back to work, exactly as the fibroblast-collapse model predicts.
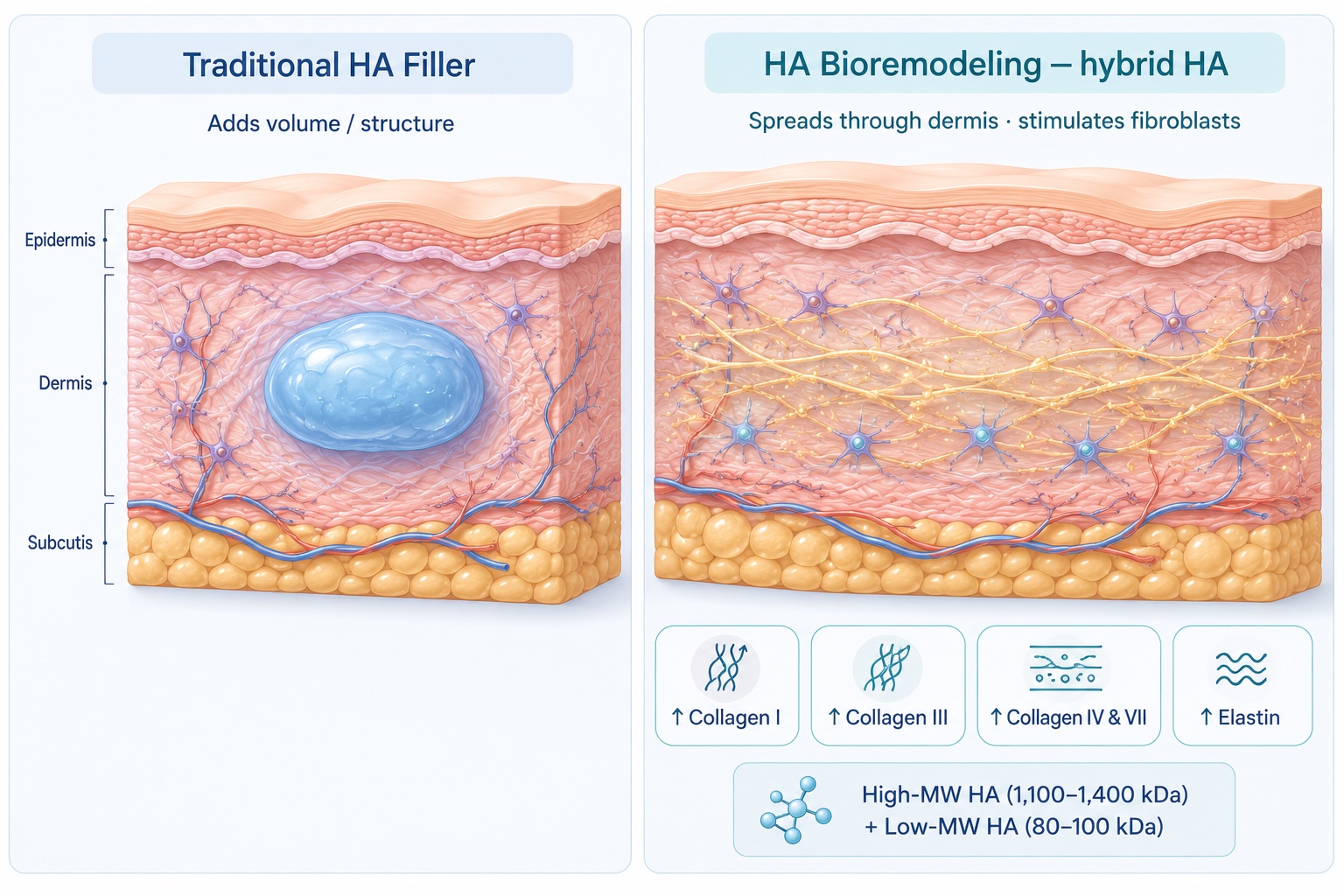
Figure 6. Hyaluronic Acid Bioremodeling vs. Traditional Filler: Two Different Jobs
Bioremodeling is not the same as filling. A hybrid of high- and low-molecular-weight hyaluronic acid spreads through the dermis and signals fibroblasts to rebuild collagen (types I, III, IV, VII) and elastin — improving skin quality rather than adding volume.
3d. Poly-L-Lactic Acid (Sculptra): The 25-Year Collagen Factory
The most clinically mature collagen biostimulator is not a peptide at all but a synthetic polymer. Injectable poly-L-lactic acid (PLLA-SCA, marketed as Sculptra by Galderma) has been used in aesthetic dermatology for over 25 years.[26] Its microparticles provoke a controlled, suture-like foreign-body response — recruiting M2-polarized macrophages and activating fibroblasts — that drives gradual neocollagenesis as the polymer breaks down to carbon dioxide and water.[27] The data are quantitative: in one clinical study of 14 subjects, subdermal PLLA increased type I collagen by 65.5% at three months, and ex vivo work showed dose-dependent rises in COL1A1 mRNA alongside a fall in MMP-1 — building collagen and slowing demolition simultaneously.[28]
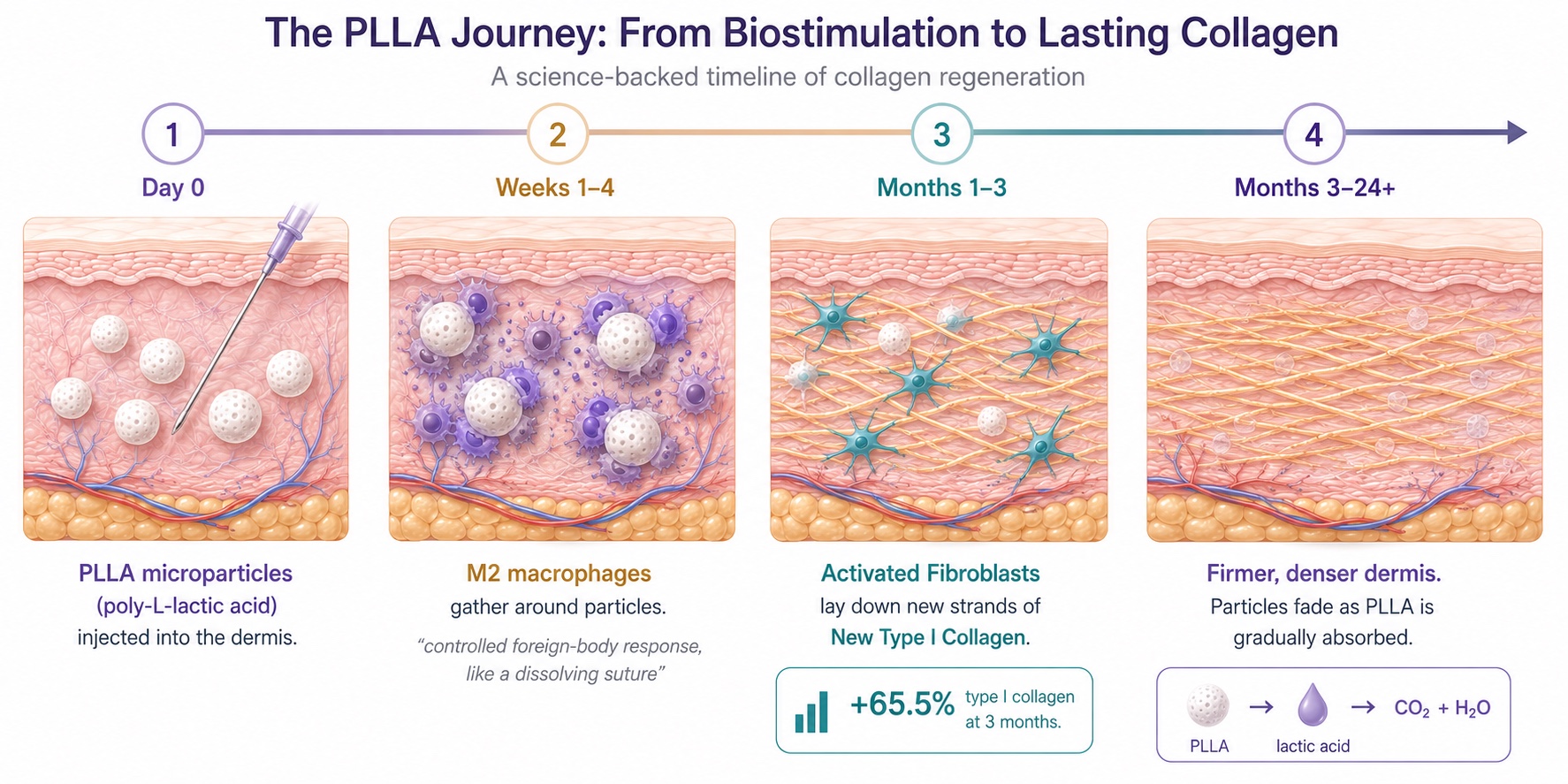
Figure 7. How Poly-L-Lactic Acid Builds New Collagen Over Months
Poly-L-lactic acid doesn't fill — it farms collagen. PLLA microparticles trigger a controlled, suture-like response that recruits macrophages and wakes fibroblasts, which lay down new type I collagen over months as the polymer harmlessly breaks down to CO₂ and water.
W. Philip Werschler, among the cited investigators in this field, identified increased type I collagen in histologic studies of treated skin, and randomized, double-blind work later validated PLLA for overall skin quality.[29] The U.S. Food and Drug Administration's labeled indications now include not only nasolabial folds but fine lines and wrinkles in the cheek region — a meaningful regulatory acknowledgment that a biostimulator can treat wrinkles, not merely volume loss.[30] The trade-off the buyer must accept: results build slowly over months and depend heavily on injector skill, and the product carries clear contraindications, including keloid history and the universal vascular-occlusion risk of any facial injectable.[31]
3e. A Truthful Word on "Anti-Aging Peptide" Hype
Differentiating this brief from the fluffier wellness genre requires saying plainly: several peptides marketed online for skin rejuvenation — including systemic compounds promoted for "turning back time" — lack robust randomized human dermal trials, and some carry regulatory and safety question marks when injected off-label.
The categories above earn their place because each has a defined mechanism and human data.
A molecule with a compelling cell-culture story is a hypothesis, not a result. Hold the rest to the same standard you would hold a new drug, because that is what they are.
4. How the Major Companies Compete — and Where the Innovators Live
The aesthetic-collagen market is a useful case study in how firms address the same demand with different scientific bets. Reading the competitive map by mechanism, rather than by celebrity endorsement, tells you who is investing in what.
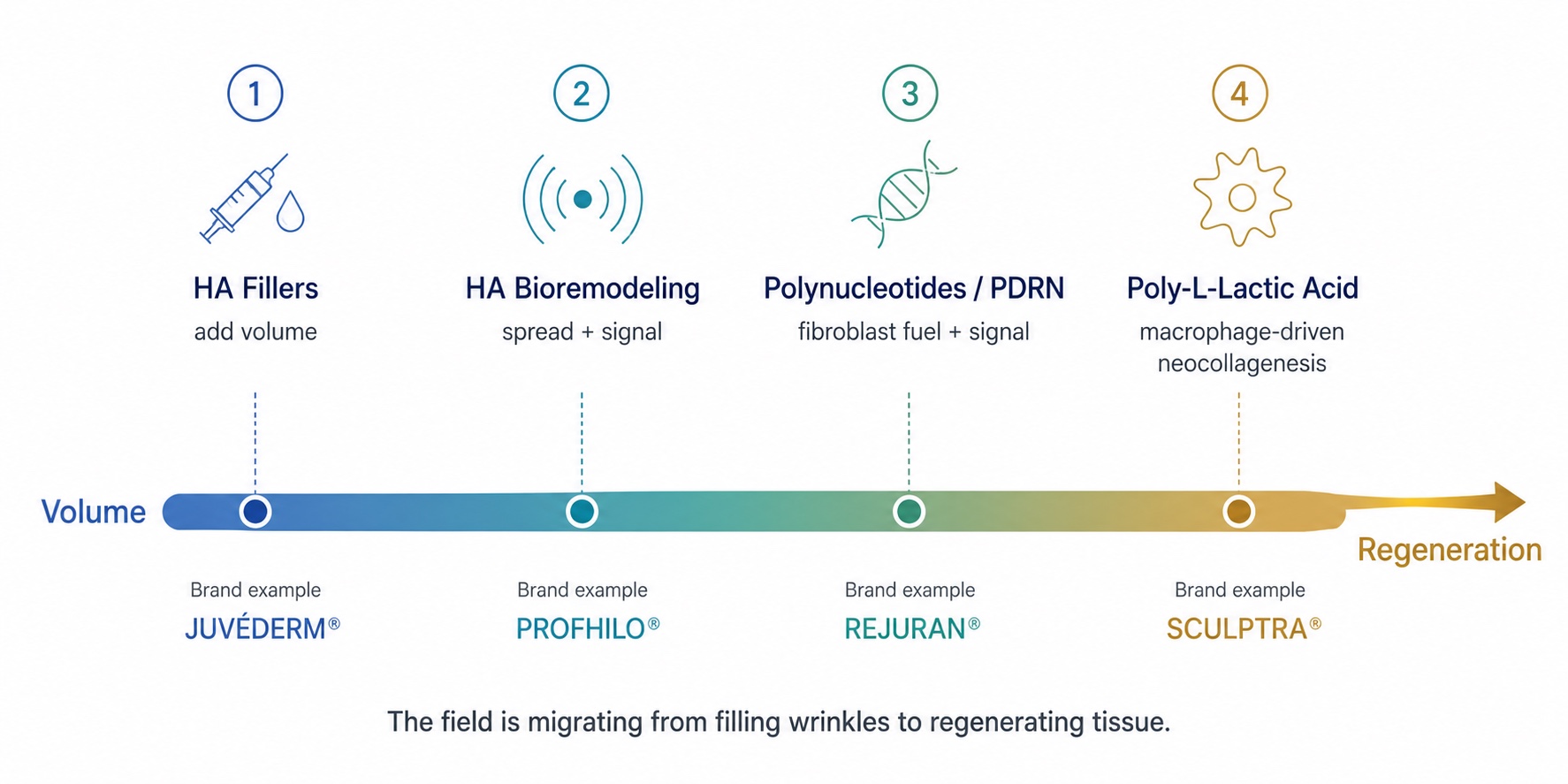
Figure 8. The Injectable Spectrum: From Volume Fillers to Collagen Regeneration
One way to read the market: a spectrum from "add volume" to "regenerate tissue." The strategic shift — and where the science is heading — is rightward, toward injectables that rebuild the skin's own collagen.
The neurotoxin-and-filler giants compete primarily on breadth and trust. AbbVie's Allergan Aesthetics anchors the category through the Botox and Juvéderm franchises and is extending into regenerative skin quality. Galderma has staked the strongest position in collagen biostimulation through Sculptra's 25-year evidence base and FDA wrinkle indication. Germany's Merz Aesthetics competes with its own biostimulator (calcium-hydroxylapatite) and energy devices. The newer toxin entrants — Evolus and Revance Therapeutics (now under Crown Laboratories) — are pushing on duration and patient experience, while Korea's Hugel and Daewoong have globalized lower-cost toxins. The strategic throughline: the majors are migrating from "fill the wrinkle" toward "regenerate the tissue."
The bioremodeling and regenerative specialists compete on mechanism and purity. IBSA Derma owns the HA-bioremodeling niche with its NAHYCO platform. Mastelli and PharmaResearch contest the polynucleotide space on source purity and clinical pedigree. Sinclair Pharma (now part of Huadong Medicine) and Teoxane add differentiated biostimulator and HA portfolios.
The genuine innovators are worth watching because they attack the supply problem at its root:
- CollPlant Biotechnologies produces recombinant human type I collagen grown in genetically engineered tobacco plants — animal-free, batch-consistent collagen as a raw material for regenerative products and bioprinting, sidestepping the variability of animal- or cadaver-derived collagen.
- Caregen is a peptide-focused biotech that designs and patents bioactive growth-factor-mimetic peptides used across dermatology and hair, exemplifying the "designed peptide" thesis rather than the "borrowed molecule" one.
- Promoitalia (Nucleofill) and Italy's broader polynucleotide cluster are differentiating by anatomical precision — formulations tuned for the under-eye and other delicate zones.
- Yuvan Research, a California longevity biotech, is tackling the oldest GHK-Cu problem — getting the peptide to actually penetrate skin — with a stabilized topical delivery gel, a reminder that delivery, not just the molecule, decides clinical fate.
5. From Molecule to Plan: The Digital Twin for Predictive Peptide Performance™
Knowing the menu is not the same as ordering well. This is where LongevityPlan.AI's broader thesis applies: in preventive medicine, data beats guesswork, and the most powerful interventions are those matched to the individual. The same architecture that powers a Cardiorespiratory Digital Twin™ for an endurance athlete can be applied to the dermal-collagen system.
The model is built in layers. The sensor layer captures what changes day-to-day — high-frequency dermal ultrasound for collagen density, cutometer elasticity readings, standardized cross-polarized imaging, plus systemic inputs (sleep, inflammatory markers, UV dose). The genomic blueprint supplies the fixed substrate beneath it. The intelligence layer fuses these multi-modal health data streams and runs predictive modeling to forecast, for a specific person, which biostimulator class is likely to deliver the largest density gain per dollar and per month, and how fast their MMP-1 genotype will erode the result. Over successive cycles, the system delivers AI-powered coaching improvements, tightening its estimate of your optimal maintenance interval the way a training model learns an athlete's recovery curve.
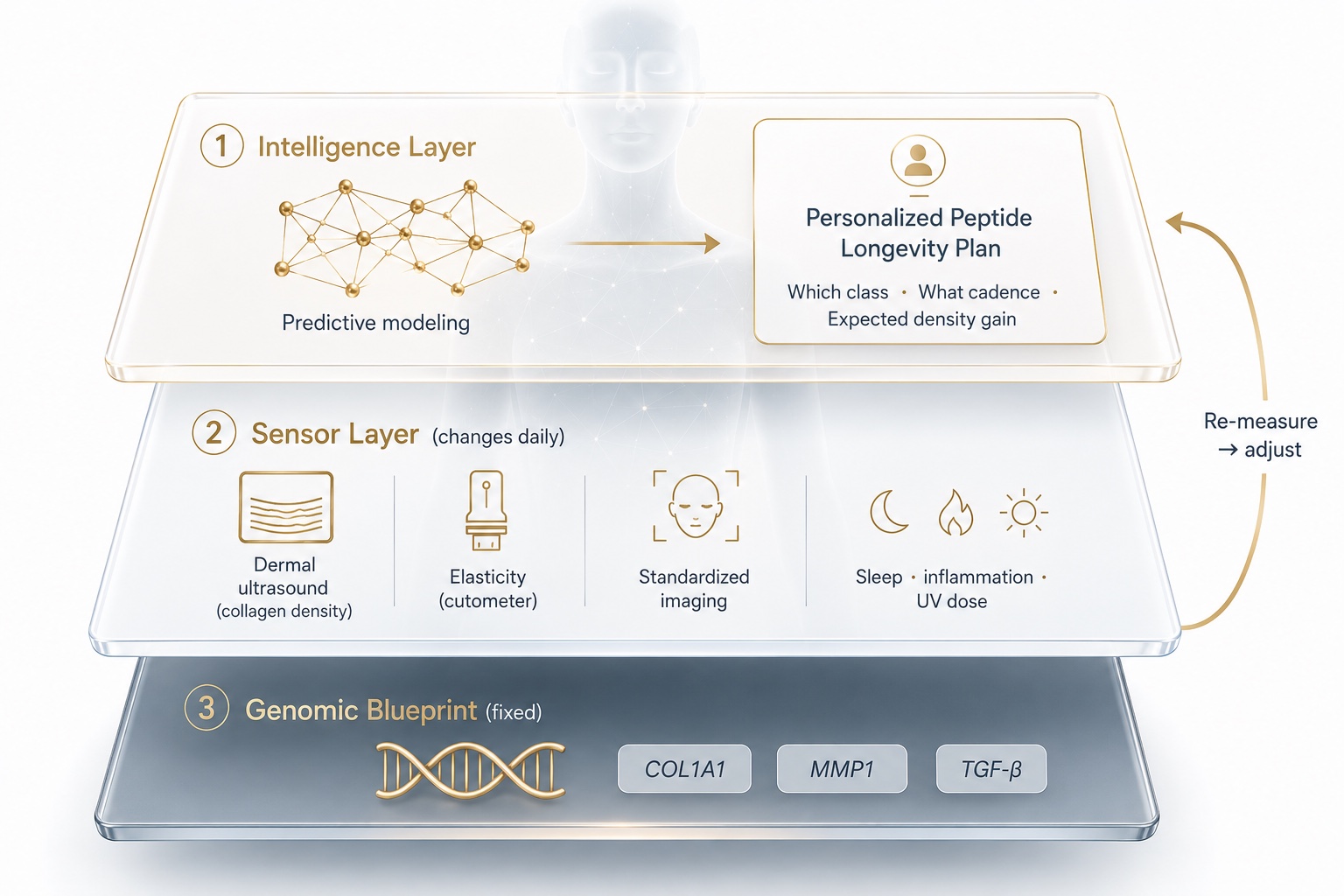
Figure 9. The Digital Twin for Predictive Peptide Performance: Sensor, Intelligence, and Plan Layers
The Digital Twin for Predictive Peptide Performance™ stacks a fixed genomic blueprint beneath daily sensor data, then uses predictive modeling to forecast which injectable, at what cadence, will work best for one specific person — and updates as it re-measures.
The genome tells you the demolition rate. The sensors tell you the current structure. The twin tells you which intervention, at what cadence, will keep the two in your favor — before you spend a cent on the wrong one.
In practice, this reframes the relationship between the Coach / Practitioner and the Athlete / Patient. Peptide Therapy stops being a product you buy and becomes a measured input in a feedback loop: baseline, intervene, re-measure, adjust. A personalized Peptide Longevity Plan™ sequences the four mechanism classes based on your genotype and goals, rather than chasing whatever is trending. This is the same evidence-first posture that NASA applies to astronaut deconditioning, that Stanford Athletics and U.S. Olympic programs apply to load management, and that clinicians like Eric Topol and Peter Attia have argued should define "Medicine 3.0": proactive, personalized, prevention-weighted. For organizations, the logic scales — a Corporate Wellness Program or a membership Longevity Club can extend the same predictive infrastructure to a workforce or community, turning episodic vanity spending into a managed healthspan asset.
6. The Skeptic's Decision Framework
Strip away the branding, and a rational buyer's guide reduces to a few questions, answered with data rather than hope:
- What is my actual problem? Thin, crepey, low-density skin and fine lines point toward regeneration (PDRN/PN, HA bioremodeling, PLLA). Lost facial volume is a different fix (structural fillers). Confusing the two wastes money.
- What does my genome predict? A high-demolition MMP1 profile argues for the most durable collagen builder (PLLA) plus tighter maintenance; a strong synthetic genotype may respond beautifully to gentler bioremodeling.
- What is the evidence tier? Favor mechanisms with human histology and randomized data (PLLA, HA bioremodeling, topical GHK-Cu, PDRN series) over molecules with only cell-culture stories.
- Who is holding the needle? For every biostimulator and filler, injector skill and vascular safety training dominate outcomes — which is why the American Society for Dermatologic Surgery and dermatology societies publish filler safety guidance.
- How will I measure it? If you cannot quantify a before-and-after (ultrasound density, elasticity, standardized photos), you cannot know whether you are buying biology or buying a story.
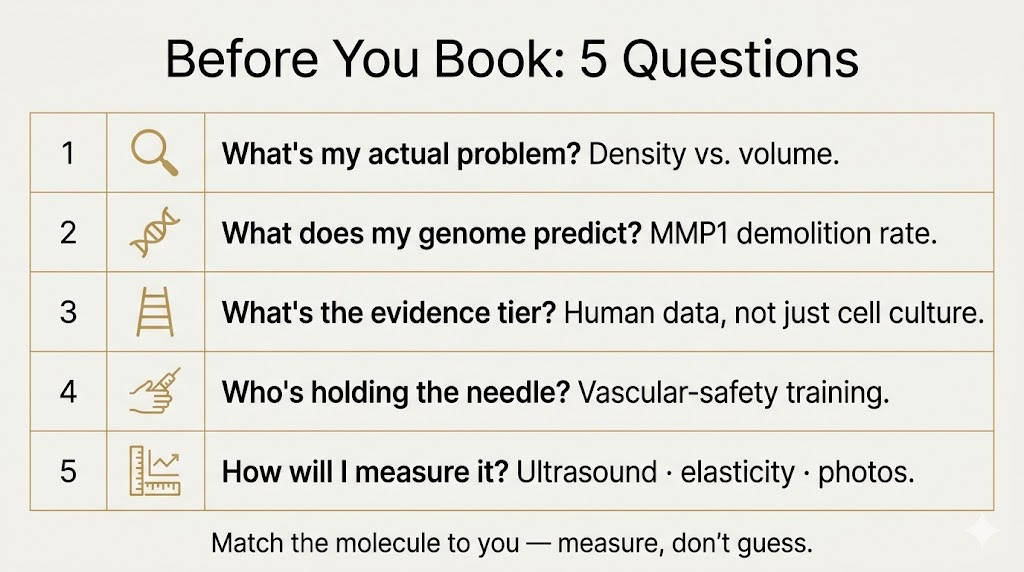
Figure 10. Five Data-Driven Questions Before Any Collagen Injectable
A saveable checklist for skeptical buyers. The molecule matters less than the match — and the only way to know whether you're buying biology or a story is to measure yourself before and after.
The through-line is unglamorous and entirely the point: the molecule matters less than the match. The best injectable for the population average may be a poor choice for you, and the only way to know is to measure you.
7. The Bottom Line
The collagen story is one of the rare places where anti-aging marketing and actual cell biology point in the same direction — collagen loss is real, mechanistic, and at least partly reversible, and several injectables have credible human data to back them. The discipline is in the matching. Your fibroblasts, your MMP1 promoter, your TGF-β signaling, and your metabolism are not the average, and a genome-anchored, sensor-fed model is simply the honest way to respect that.
There is a quieter point underneath all of this. The same fibroblast biology that shows up as a wrinkle at 45 shows up as a fragile tendon at 60 and a stiff arterial wall later still. Treating skin as the visible edge of a system — and planning for it early, with data — is not vanity. It is the most legible on-ramp to thinking about your whole healthspan while you still have the most degrees of freedom to change it. The best time to build a model of your own biology was twenty years ago. The second-best time is before your next appointment.
Sign Up for the LongevityPlan Affiliate Program (Pays 20%)
About the Author
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data from athletes and leverages proprietary Digital Twin for Predictive Peptide Performance™ technology, wearable data, and biomarker data to deliver personalized performance optimization and longevity recommendations to athletes, coaches, organizations, businesses, government, and the military. In addition to being a 3x technology / AI company CEO with 2 successful exits, Tony has also finished 3 Full Ironman Triathlons (140.6 mi) since 2019. He has degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University.
Tony has been involved with AI and molecular diagnostic start-ups for 10 years, and also worked with the US Olympic Team, National Basketball Association (NBA), National Football League (NFL), Major League Baseball (MLB), Iditarod, FBI, NASA, U.S. Department of Health and Human Services (HHS), Google, Microsoft, Netflix, Bridgewater Associates, ConocoPhillips, British Petroleum, One Medical, and Jenny Craig, Inc. to provide technology, artificial intelligence and/or molecular diagnostics solutions to their employees.
One of Tony's prior companies provided Conversational AI to health, fitness, and wellness companies; another delivered access to digital libraries of British Petroleum for oil discovery; and his first was a mobile app platform funded by Softbank, which resulted in a case study published by Stanford University Press, and was taught in multiple MBA programs for a decade. Tony loves to teach and mentor; he earned public school teaching credentials in NY and MA and taught inner-city high school students to give back to the underprivileged community in Harlem. He also lectured on entrepreneurship and venture capital to second-year MBA students at Stanford Business School for five years. He co-authored one of the first issued patents for mobile applications. Tony also served as a US Navy Officer commanding an emergency response team on a USN Destroyer. Tony's military-to-CEO career has recently been chosen to air on an episode of "Operation CEO" a documentary by InsideSuccess.TV, which will air on AppleTV, Prime Video & Amazon MGM Studios, YouTubeTV, and other major platforms worldwide in 2026.
Endnotes
[1] Quan T, Fisher GJ, et al. Reviews on age-associated alterations of the dermal extracellular matrix microenvironment in human skin aging. University of Michigan Department of Dermatology research program.
[2] Faculty profile, Gary J. Fisher, PhD, Harry Helfman Professor of Molecular Dermatology and Director, Photoaging and Aging Research Program, University of Michigan Medical School.
[3] Fisher GJ, Quan T, et al. "Looking older: fibroblast collapse and therapeutic implications." Arch Dermatol. 2008;144(5):666–672.
[4] Fisher GJ, et al. Collagen fragmentation promotes oxidative stress and elevates MMP-1 in fibroblasts from aged human skin (Arch Dermatol, 2008) and in related fibroblast mechanics work.
[5] Ibid.; see also Quan T, Fisher GJ. "Extracellular matrix regulation of fibroblast function: redefining our perspective on skin aging."
[6] Expression of catalytically active MMP-1 in dermal fibroblasts induces collagen fragmentation resembling aged human skin; Col1a2;hMMP1 transgenic mouse model (J Invest Dermatol / PMC3738263; PMC11577279).
[7] Varani J, Fisher GJ, Kang S, Voorhees JJ, et al. Vitamin A (retinoic acid) stimulates collagen accumulation in naturally aged human skin in vivo; Fisher GJ, Kang S, et al. "Mechanisms of photoaging and chronological skin aging," Arch Dermatol. 2002.
[8] "Personalized skin health management... based on genetic polymorphisms" Frontiers in Genetics, 2025; COL1A1/COL1A2/COL3A1/ELN polymorphisms and skin elasticity.
[9] "MMP-1 and -3 promoter variants are indicative of a common susceptibility for skin and lung aging: results from a cohort of elderly women (SALIA)." J Invest Dermatol; PubMed 25599395.
[10] "Menopause, Ultraviolet Exposure, and Low Water Intake Potentially Interact with the Genetic Variants Related to Collagen Metabolism Involved in Skin Wrinkle Risk in Middle-Aged Women." PMC7922323.
[11] "From destruction to protection: rethinking MMP-1 in skin aging." Arch Dermatol Res, 2026; TGF-β/Smad induction of COL1A1 and repression of MMP-1.
[12] The Genomics Company (thegenomicscompany.com), saliva-based genomic interpretation and personalized "Brain & Body Blueprint" service. Company materials, 2025.
[13] Plasma GHK declines from ~200 ng/mL at age 20 to ~80 ng/mL by age 60. Pickart L, Margolina A., review literature; secondary summary at Pulse & Remedy clinical review.
[14] Maquart FX, et al. GHK-Cu at 1–10 nM stimulates the synthesis and breakdown of collagen and glycosaminoglycans and modulates MMPs/TIMPs. Summarized in "GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration" (PMC4508379).
[15] Pickart L, Margolina A. "Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of New Gene Data." Int J Mol Sci, 2018 (PMC6073405).
[16] "Peptides: Emerging Candidates for the Prevention and Treatment of Skin Senescence: A Review." MDPI, 2025 (PMC11762834); GHK-Cu serum reduced wrinkle depth vs. vehicle.
[17] Innerbody clinical review of GHK-Cu (2026); discussion of MMP-1 upregulation at certain concentrations and anecdotal "copper uglies."
[18] "Polydeoxyribonucleotide: A promising skin anti-aging agent" and clinical reviews of PDRN mechanism via A2A adenosine receptor and DNA salvage pathway.
[19] Skin Spa New York / Sunny Aesthetic clinical reviews summarizing PDRN dual mechanism (structural nucleotides + receptor signaling), 2026.
[20] Mastelli S.r.l. (Italy), Plinest line and PN-HPT purification technology; KINS Clinic and CLNQ clinical summaries, 2025–2026.
[21] PDRN injectable series (3–4 sessions) and dermal-density gains by 20 MHz ultrasound; collagen remodeling 3–6 months post-series.
[22] Market-share reporting: salmon-DNA polynucleotide boosters as the second-most-requested injectable after botulinum toxin in major markets; PharmaResearch (Rejuran), Promoitalia (Nucleofill).
[23] Profhilo (IBSA Farmaceutici Italia), NAHYCO Hybrid Technology; 32 mg H-HA (1,100–1,400 kDa) + 32 mg L-HA (80–100 kDa), 64 mg/2 mL; product and review literature.
[24] In vitro dermal-components remodeling: increased type I, III, IV, VII collagen and elastin vs. H-HA or L-HA alone; D'Agostino et al.; Stellavato et al.
[25] "A Systematic Review of the Efficacy and Safety of Profhilo" (9 studies, 278 participants; PMC13038071); "Safety Assessment... Worldwide Postmarketing Data" (>40,000 patients; PMC7327616).
[26] Avelar LE, Nabhani S, et al. "Unveiling the Mechanism: Injectable Poly-L-Lactic Acid's Evolving Role." J Cosmet Dermatol, 2025 (PMC11743305). (Disclosure: authors are Galderma investigators/employees.)
[27] "Poly-L-lactic Acid (Sculptra): A Regenerative Aesthetic Treatment." Cosmetics (MDPI), 2026; mechanism via M2 macrophages and fibroblast neocollagenesis.
[28] Goldberg D, et al. clinical study (14 subjects): type I collagen +65.5% at 3 months; ex vivo dose-dependent COL1A1 mRNA increase and MMP-1 decrease (Avelar review, PMC11743305).
[29] Werschler WP, histologic type I collagen findings (cited in PMC7564527); Bohnert K, Dorizas A, Lorenc P, Sadick NS. RCT of injectable PLLA for skin quality. Dermatol Surg. 2019;45(5):718–724.
[30] Sculptra Instructions for Use, Galderma Laboratories, 2023; FDA indications include nasolabial folds and fine lines/wrinkles in the cheek region.
[31] Sculptra IFU contraindications (keloid/hypertrophic scarring history) and vascular occlusion warning; general filler safety guidance from the American Society for Dermatologic Surgery.
This article is for education and is not medical advice. Injectable treatments carry risks, including vascular occlusion; consult a qualified, appropriately trained physician. Several cited clinical summaries are secondary sources; primary peer-reviewed citations are listed where available.
Earn while you share. Join the LongevityPlan Affiliate Program and earn 20% on every referral.