Mental Health
·16 min read
The Calmer Mind, Engineered by Artificial Intelligence and Peptides
How AI and peptides are turning PTSD, stress, and mental wellness from a guessing game into a measurable, personalized plan, and what a skeptical, high-performing adult should actually believe.
By Tony Medrano, CEO & Founder, LongevityPlan.AI
Here is an uncomfortable statistic to open a wellness article with: most people reading this have already lived through a qualifying trauma. Population studies estimate that roughly 70% of adults worldwide experience at least one traumatic event in their lifetime, and somewhere between 6% and 9% will go on to develop post-traumatic stress disorder. In the United States, the lifetime figure sits near 6–7%; in Canada, which ranks highest among 24 surveyed nations, it is 9.2%. Those are the clinical cases. The far larger group is everyone walking around with the subclinical residue — the disrupted sleep, the flattened affect, the over-reactive threat system that quietly taxes decision-making, recovery, and healthspan long before anyone files a diagnosis.
This is not a veterans' issue, though veterans gave us much of the science. It is a high-performer's issue. The same neurobiology that produces combat PTSD also governs how a 52-year-old founder metabolizes a hostile board meeting, how a masters athlete recovers from a frightening crash, and how an aging parent processes a cancer scare. Chronic stress is not a character flaw; it is a measurable, modifiable physiological state. And for the first time, two very different scientific revolutions are converging on it: peptides, which let us speak to the brain in its own signaling language, and artificial intelligence, which lets us figure out who needs which message, when, and at what dose.
This brief is written for the skeptic — the reader who has heard "peptides" pitched alongside dubious anti-aging serums and "AI therapy" pitched as a chatbot that will solve everything. Good. Skepticism is the correct posture. Our job is to separate the genuinely evidenced from the genuinely overhyped, name the scientists doing the real work, and show how a data-driven longevity plan treats the mind with the same rigor the NBA brings to a hamstring.

Two revolutions are converging on the stressed brain: peptides that speak its own chemical language, and AI that decides who needs which message, when, and at what dose.
1. Why the Brain Speaks in Peptides
Peptides are short chains of amino acids — biology's text messages. Where a small-molecule drug is a blunt instrument that floods the whole system, many peptides are endogenous signaling molecules the body already uses to fine-tune specific circuits. That specificity is exactly what makes them interesting for mental wellness, and exactly why their effects are so frustratingly individual. A peptide is a key; whether it opens anything depends on the locks you happened to inherit.
Oxytocin: the cautionary tale that taught us precision
Oxytocin is the obvious place to start, because it is both the most famous "trust molecule" and the most instructive failure of one-size-fits-all thinking. At Amsterdam UMC and the ARQ National Psychotrauma Center, Miranda Olff, Mirjam van Zuiden, and Jessie Frijling ran one of the field's most rigorous early-intervention programs — the BONDS study — giving intranasal oxytocin to recently traumatized emergency-department patients to see whether it could head off PTSD before it consolidated.
The headline result was sobering: across the whole sample, oxytocin did not reliably prevent PTSD. But buried in the data was the lesson that defines modern psychiatry. In the subgroup of patients who arrived with high acute symptom severity, oxytocin produced a meaningful benefit. Olff's own framing is characteristically measured — oxytocin is known mainly for its pro-social effects, and the alleviating effects observed were small with clinical significance still to be established. Translation: the molecule works, but only for the right person at the right moment. Average a treatment across a mixed population and you erase the signal. That single insight — stratify, don't average — is the seed of everything AI is now bringing to the field.
Neuropeptide Y: the resilience the Special Forces already had
If oxytocin is about repair, neuropeptide Y (NPY) is about armor. In a now-classic series of studies at the National Center for PTSD, Charles Morgan, Ann Rasmusson, and Dennis Charney measured NPY in soldiers going through the U.S. Army's brutal survival school. Elite Special Forces soldiers not only mounted higher NPY surges under extreme stress, but they also returned to baseline faster than conventional troops — and their NPY levels tracked with staying mentally sharp under pressure. The mirror image showed up in combat veterans with PTSD, who carried abnormally low plasma and cerebrospinal fluid NPY.
NPY acts as a built-in brake on the stress response, counteracting corticotropin-releasing hormone and quieting the brain's noradrenergic alarm. As the resilience reviews by Charney's group put it, NPY is among the most promising endogenous candidates for building stress tolerance rather than merely treating its aftermath. Intranasal NPY has been tested in early human trials as a result. The performance framing writes itself: this is the molecule that separates the operators who stay cognitively online in a crisis from those who don't — and it is, in principle, measurable.
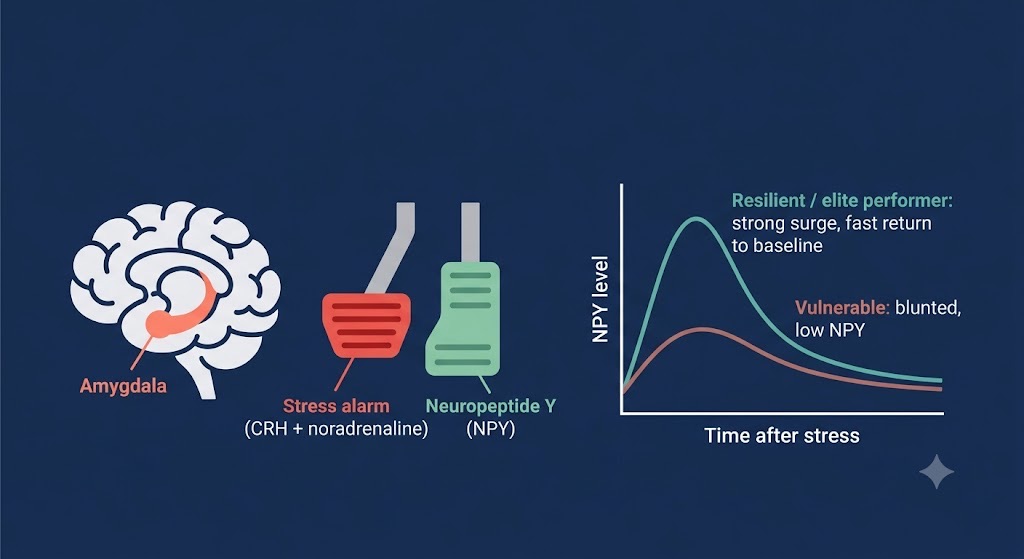
Neuropeptide Y acts as a natural brake on the stress alarm. The most resilient performers surge the hardest under pressure — and return to baseline fastest.
PACAP and PAC1: where sex, genes, and trauma collide
The most genetically elegant story belongs to Kerry Ressler, now at McLean Hospital and Harvard, working with Tanja Jovanovic (Wayne State) and colleagues. In a landmark 2011 Nature paper, they showed that blood levels of pituitary adenylate cyclase-activating polypeptide (PACAP) tracked with PTSD diagnosis and fear physiology — but, strikingly, only in women. They then traced the effect to a single genetic variant (rs2267735) sitting inside an estrogen-response element of the PAC1 receptor gene. Inherit one version, and your fear circuitry and PTSD risk shift measurably.
This matters for two reasons. First, it offers a biological explanation for why women carry roughly twice the PTSD risk of men. Second, and more sweeping, PTSD is roughly 30–40% heritable. Your trauma response is not pure psychology; it is partly written in code you were born with. Hold that thought — it is the hinge the rest of this article turns on.
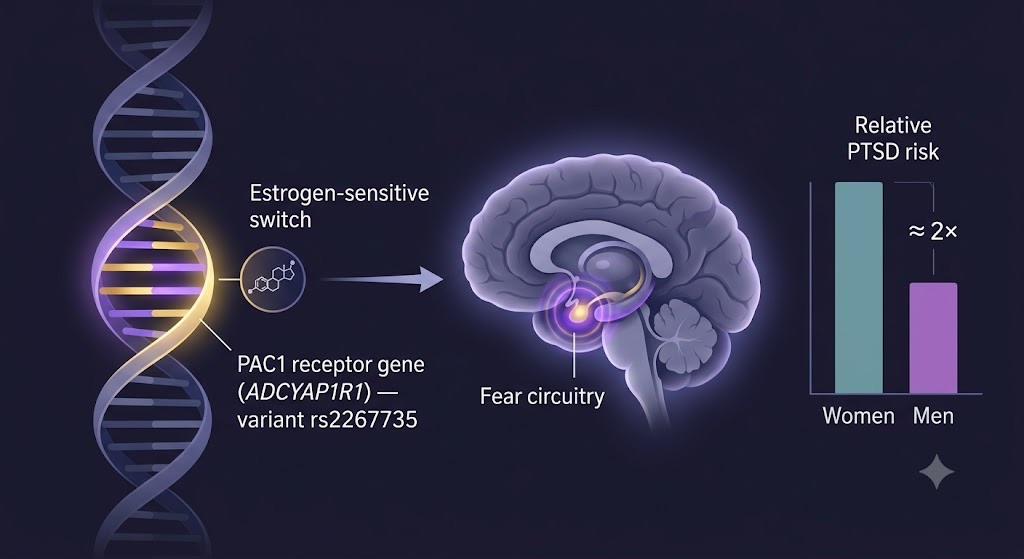
One inherited variant in the PAC1 receptor gene tracks with fear physiology and PTSD — a clue to why women carry roughly twice the risk, and to why genetics belongs at the foundation of any plan.
The designer peptide: targeting the stress switch itself
Then there is the work that points to the future. At the Center for Addiction and Mental Health (CAMH) in Toronto, Fang Liu's team identified a protein complex — the glucocorticoid receptor bound to FKBP51 — that stays abnormally elevated in people who develop PTSD, where in resilient individuals it returns to baseline after stress. Liu's group then built a peptide to physically disrupt that complex, and in preclinical work, it blocked the encoding and recall of fear memories. Liu's stated ambition is striking: this CAMH-led discovery could help millions by serving as both a blood-based biomarker and a nasal-spray peptide administered at the moment of trauma. This is precision psychiatry in its purest form — find the broken molecular switch, design a custom key, deliver it before the damage sets.
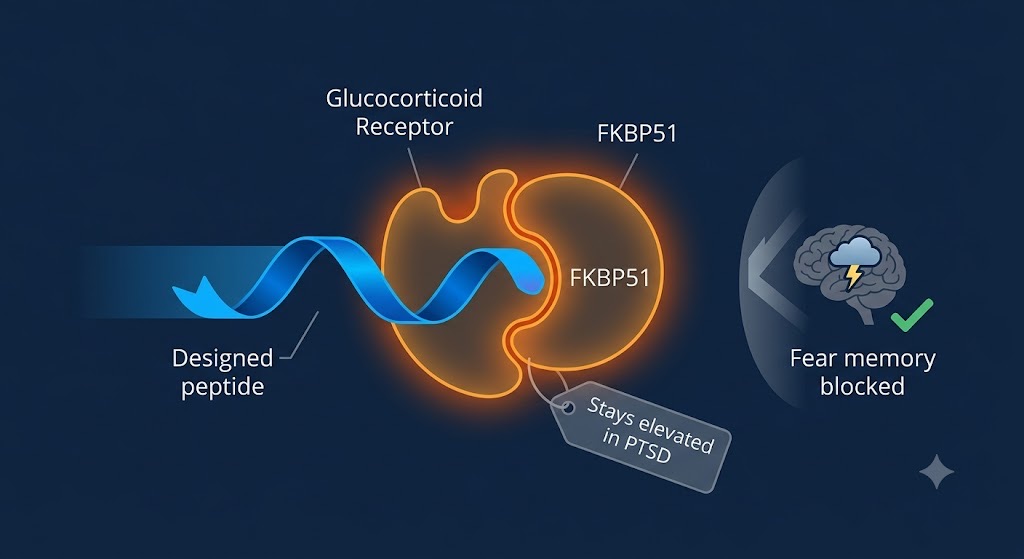
A custom-built peptide acts like a precision key — prying apart the overactive stress-hormone complex that helps lock traumatic memories in place.
Selank and Semax: where the skeptic should stay skeptical
Now the honest part. The peptides most aggressively marketed for anxiety and focus — Selank and Semax — deserve a clear-eyed paragraph. Both were developed at Russia's Institute of Molecular Genetics. Semax is a fragment-analog of ACTH(4-10) that influences BDNF and dopamine signaling; Selank is a tuftsin analog that modulates GABAergic and enkephalin pathways and has completed Phase III trials in Russia for generalized anxiety disorder. In Russia, they are registered medicines with decades of use and a favorable side-effect profile.
But — and this is non-negotiable for a data-driven reader — neither is FDA-approved in the United States. Western clinical evidence is thin, and the U.S. FDA has specifically flagged compounded versions for limited human safety data, immunogenicity risk, and impurity concerns. "Used for decades in Russia" is a real data point; it is not the same as a registered, replicated, Western-standard trial. A responsible plan treats these as investigational rather than established. The skeptic who keeps these in the "interesting, unproven" column is reasoning correctly.
The GLP-1 surprise: a metabolic peptide that quiets craving
Finally, one peptide family closes the loop between body and mind. GLP-1 receptor agonists — semaglutide and its relatives, the molecules behind the weight-loss boom — are peptide hormones, and they act not only on appetite but on the brain's reward and craving circuitry, modulating inhibitory signaling in the amygdala: the same fear-and-reward hub at the center of the trauma story. The clinical signal is mounting. A 2025 JAMA Psychiatry randomized trial led by Christian Hendershot found that once-weekly semaglutide reduced alcohol craving and consumption, and a registry of 227,866 people showed lower alcohol-related harm during periods of GLP-1 use.
The point is not that Ozempic cures trauma. It is that the wall between metabolic and mental health is largely imaginary, and peptides are the molecules that operate on both sides of it at once, which is precisely why they belong in a longevity plan rather than a single specialty. Novo Nordisk and Eli Lilly built empires on what GLP-1 does to the waistline; the neuroscience may prove the more profound legacy.
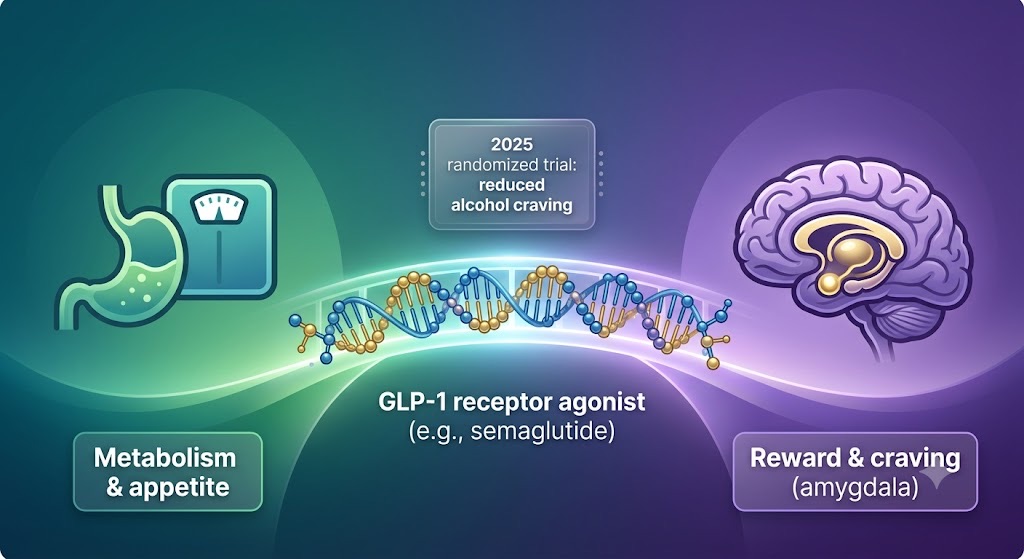
GLP-1 peptides blur the line between body and mind — acting on metabolism and on the brain's reward-and-craving hub at once, and showing why peptides belong in a whole-person longevity plan.
2. Genetics: Why Your Friend's Miracle Peptide Does Nothing for You
Here is that hinge. Trace the through-line of every peptide above and one principle emerges: the same molecule produces different results in different bodies, and the difference is frequently genetic. The PAC1 variant that reshapes women's fear circuitry, the FKBP5 stress-hormone machinery Fang Liu targets, the inherited NPY tone that keeps some operators calm under fire — these are not edge cases. They are the rule.
This is where pharmacogenomics earns its place at the foundation of any serious plan. Genetics shapes peptide and drug response on at least three levels: the target (does your receptor variant respond?), the metabolism (your liver's CYP450 enzymes determine how fast you clear a compound — fast metabolizers underdose themselves, slow metabolizers accumulate side effects on a "normal" dose), and the risk landscape (which circuits are already vulnerable). Companies such as The Genomics Company are building exactly this kind of genetic assessment into personalized protocols — the argument being that you should know your relevant variants before you spend a year and a small fortune trialing peptides by feel.
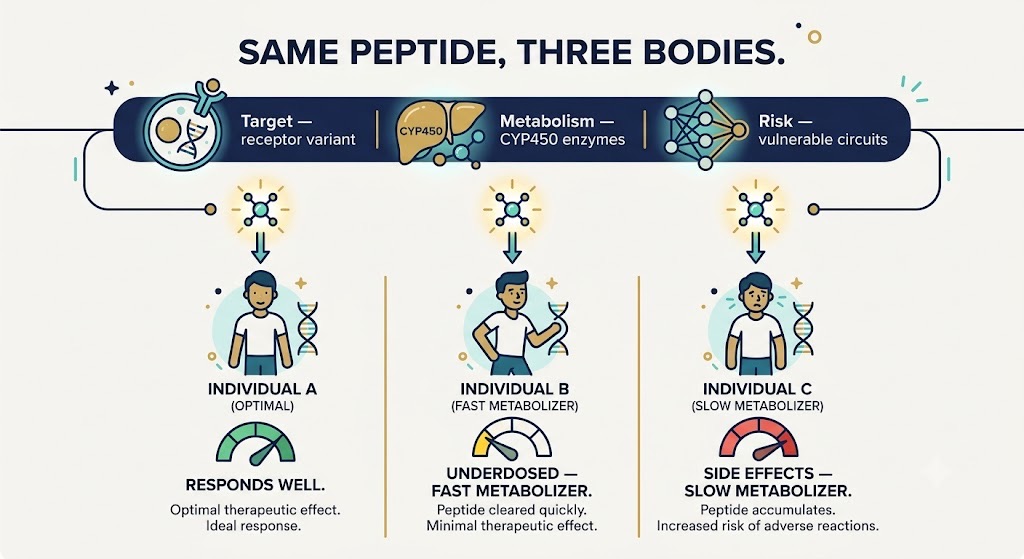
Same peptide, different bodies. Genetics shapes the target, the metabolism, and the risk, which is exactly why a protocol built on the population average so often fails the individual.
The skeptic's checkpoint. If a clinic offers you a peptide for stress or mood and has not asked about your genetics, medications, baseline biomarkers, or CYP450 metabolism, they are guessing. Sophisticated guessing, perhaps — but guessing. The science of the last fifteen years says response is heterogeneous and partly heritable. Any protocol that ignores that is selling you the average, and you are not the average.
3. The AI Layer: Three Jobs Machines Now Do Better Than We Did
If peptides are the message, AI is what makes the message land. It is doing three distinct jobs in mental health right now, and conflating them is the source of most of the hype and disappointment. AI is learning to measure the mind, design new molecules, and deliver support at scale. Only the first two are mature. The third is promising and genuinely contested.
Job one: measuring the mind
Psychiatry's oldest problem is that it has no blood test. Diagnosis rests on interviews and self-report, which are subjective, biased, and easy to mask — a veteran ashamed of his symptoms, an executive who has rehearsed sounding fine. The most elegant fix may be hiding in plain sound. At NYU Langone, Charles Marmar partnered with SRI International — the lab that built Siri — to ask whether the voice itself carries a fingerprint of trauma.
It does. Their algorithm partitioned the human voice into more than 40,000 features, then used a random-forest model to narrow them to 18 that distinguished veterans with PTSD from those without, reaching roughly 89% accuracy. The most revealing detail was that the team's intuition was wrong. As Marmar put it, they expected agitated speech, but the features are flatter, more atonal speech — the machine was capturing the emotional numbness clinicians know but cannot quantify. This is the sensing frontier of modern mental health: a passive, cheap, non-intrusive signal a model can read continuously. Startups, including Ellipsis Health, have since turned vocal biomarkers into screening tools deployable inside ordinary telehealth calls, validated across age groups, including older adults. The work was funded in part by Cohen Veterans Bioscience, one of the field's most serious private backers.
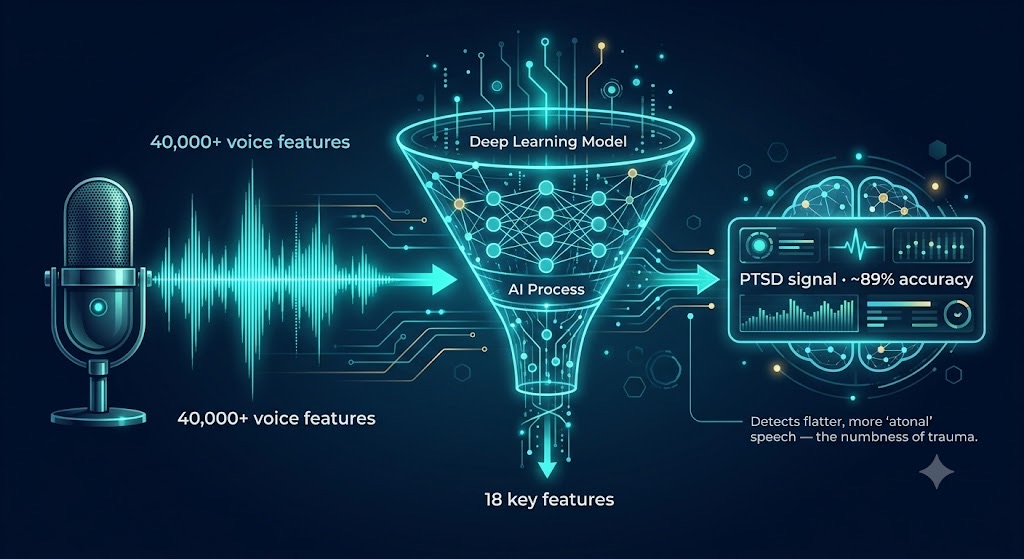
AI can hear trauma in the voice — distilling tens of thousands of vocal features down to a handful that reveal the emotional flatness clinicians have long described but never measured.
Job two: designing molecules that never existed
The deepest application of AI here is also the least visible to consumers. In 2024, David Baker of the Institute for Protein Design at the University of Washington shared the Nobel Prize in Chemistry for computational protein design — the first time a machine could conjure entirely new proteins from a molecular wish list. His lab's diffusion models, RFdiffusion and its descendants, do for proteins what image generators do for pictures: specify the target, generate the molecule.
For our purposes, the breakthrough is RFpeptides, published in Nature Chemical Biology, which designs ring-shaped "macrocyclic" peptides that bind disease-associated proteins using only the target's structure — no brute-force library screening. Cyclic peptides resist degradation and bind tightly, exactly the properties you want in a brain-targeting therapeutic. Gaurav Bhardwaj, who led the work with Baker, framed the stakes plainly: the goal is peptide-based medicines for a variety of diseases for which there are no good options today. The university has licensed the technology to a spinout, Vilya. Imagine the Fang Liu strategy — disrupt a specific stress-protein complex — but with the precise binder designed by an AI in days rather than discovered by luck over years. That is the pipeline taking shape.
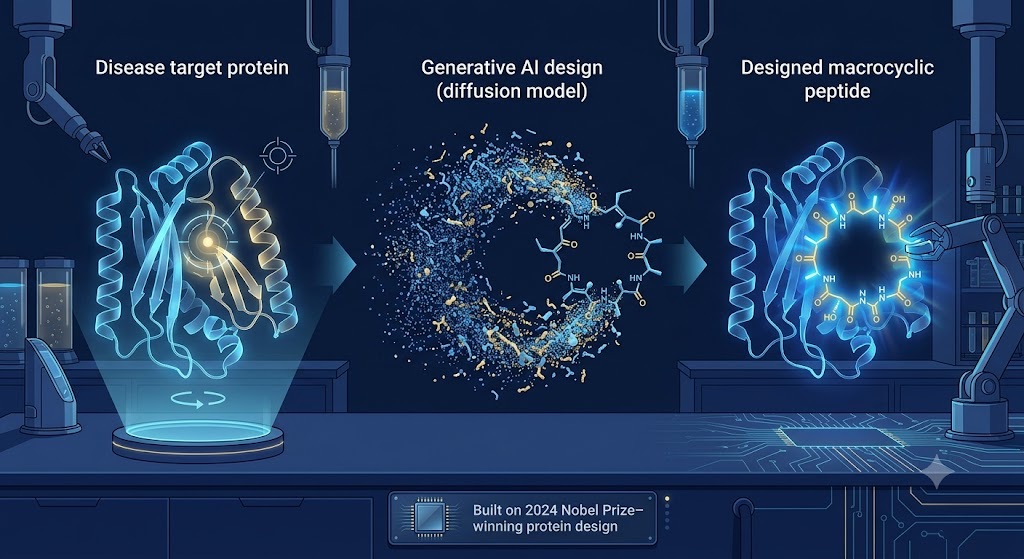
Generative AI now designs ring-shaped peptides to order — collapsing years of trial-and-error library screening into days of computational design.
Job three: delivering support — and its honest limits
The most visible — and most overhyped — frontier is AI that talks back. The provocative data point arrived in March 2025, when a Dartmouth team led by Nicholas Jacobson published in NEJM AI the first randomized controlled trial of a generative-AI therapy chatbot, "Therabot." Across 210 adults with depression, anxiety, or eating-disorder risk, the four-week intervention produced symptom reductions of roughly 51% for depression, 31% for anxiety, and 19% for eating-disorder concerns — comparable to outpatient therapy, with unusually high engagement.
Before anyone declares therapists obsolete, listen to the field's own skeptics. John Torous, who directs digital psychiatry at Beth Israel Deaconess Medical Center, warned publicly that social-media enthusiasm was outrunning the evidence — one promising trial is not a revolution. That tension is healthy, and it is exactly the posture the new institutional players are taking. At Stanford, the CREATE Center — co-directed by Shannon Wiltsey Stirman and Johannes Eichstaedt and funded by an $11.5 million NIH grant — is explicitly building large language models to assist clinicians, not replace them, for a PTSD population where access, not just efficacy, is the bottleneck. Eichstaedt's framing is the one to remember: large language models are not ready to act as stand-alone therapists, but can meaningfully support the humans who are.
Used well, this is AI as the tireless Coach / Practitioner working alongside the human one — available at 2 a.m. when the panic actually hits. The evidence base is real but young. Woebot Health (founded by Alison Darcy, whose 2017 trial first showed an automated CBT agent could reduce depression and anxiety) and Wysa (which earned an FDA Breakthrough Device Designation for managing chronic pain and its associated mood symptoms, and is being evaluated inside the UK's NHS) represent the more rigorously studied, narrowly-scoped end of the market. UK triage tool Limbic is doing similar work upstream, deciding who needs human care fastest. Headspace Health sits on the consumer end. The pattern that separates the credible from the promotional is simple: published trials, clear scope, and a crisis-escalation pathway to a human.
4. The Digital Twin: Turning the Layers Into a Plan
Sensors that read your state. Genetics that predict your response. Designed molecules that hit precise targets. Each is powerful alone; their value compounds when fused. That fusion is the idea behind a Digital Twin for Predictive Peptide Performance™ — a continuously updated computational model of one specific person, built to answer the question peptide medicine has never been able to answer well: which compound, at which dose, for which goal, in this body?
The architecture mirrors what the layers already provide. A sensor layer ingests multi-modal health data — wearable HRV and sleep architecture, vocal biomarkers from a daily check-in, periodic blood panels, symptom scales. An intelligence layer overlays the genetic foundation (PAC1, FKBP5, CYP450 metabolizer status, the variants that govern target and clearance) and learns the individual's baseline. Then predictive modeling does the work no clinician can do by intuition: simulating how this twin is likely to respond to a given protocol before the first injection, then correcting itself against real-world outcomes — the same logic of digital twins now used in clinical trial modeling and aerospace, applied to your nervous system.
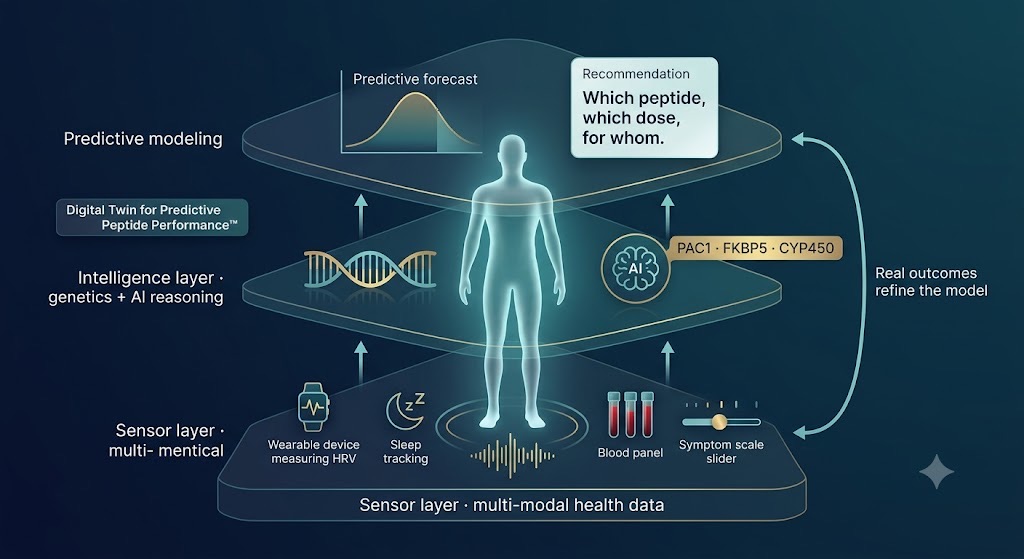
A digital twin fuses your sensors, your genes, and predictive modeling into one continuously updated model of you — replacing a year of guesswork with a structured, measurable plan.
Concretely: a digital twin that knows you carry low endogenous NPY tone, metabolize compounds slowly, and show flattening vocal markers during high-stress weeks is a twin that can flag a downturn early, recommend the evidence-based intervention most likely to fit your biology, and titrate dose against your clearance rate rather than a population average. It cannot promise miracles — the honest models won't — but it can replace a year of expensive trial and error with a structured, measurable hypothesis. That is the difference between biohacking and medicine.
5. A Buyer's Guide: Reading the Longevity Market Without Getting Sold
None of this lives in a vacuum. A whole industry has emerged to sell the data, the interpretation, and the protocols — and the offerings differ more than the marketing suggests. For the skeptical buyer, the useful frame is a spectrum from data to guidance to action.
At the data-breadth end, Function Health (founded 2021, now backed by a $298 million Series B) tests 100-plus biomarkers twice a year and hands you a rich dashboard — extraordinary raw coverage, lighter on what to do next. Superpower competes on accessibility, and an AI-driven results layer at a lower annual price. At the guidance-and-action end, clinician-led services such as Lifeforce emphasize a physician interpreting fewer markers and prescribing directly, at a premium. Newer entrants — The Protocol and Extension Health, among them — push further toward continuous, protocol-driven optimization. The instructive recent detail is that competition has gotten sharp enough to produce litigation over what even counts as a "biomarker," a sign of a market maturing past its honeymoon.

A number is not a plan, and a plan is not a result. Platforms differ most in how far they carry you from raw data toward real, personalized action.
The point of a longevity plan is not which logo wins. It is that a number is not a plan, and a plan is not a result. Most platforms excel at one stage of the data-to-action chain. Mental wellness is precisely where the chain most often breaks, because the relevant biology — genetics, neuropeptide tone, vocal and behavioral signal — sits outside a standard lipid panel. The value of integrating peptide science and an AI digital twin into a longevity plan is that it closes that gap: it connects what your biology says to what you should actually do about your mind, and then measures whether it worked.
Five questions to ask any provider before you spend a dollar on peptides for stress or mood: (1) What genetic and metabolic data informs this protocol? (2) What is the regulatory status of each compound — FDA-approved, compounded, or investigational? (3) What objective markers will we track to know it's working? (4) What is the published evidence, in humans, for this specific use? (5) Where is the human clinician, and what is the escalation path if I get worse? A provider who welcomes these questions is a partner. One who deflects them is a vendor.
6. The Honest Bottom Line
Strip away the marketing, and a coherent, defensible picture remains. The neurobiology of stress and trauma largely operates through peptides — oxytocin, NPY, PACAP, the FKBP51 stress-switch, and the GLP-1 system that links mind to metabolism. Response to those peptides is heterogeneous and partly genetic, which is why the field is abandoning averages for stratification. AI has already proven itself in measuring the mind through voice and behavior, and in designing novel peptides that would have taken decades to discover. AI-delivered therapy is real and improving, but not yet a stand-alone substitute for a human, and anyone telling you otherwise is ahead of the evidence.
The mature move is neither credulity nor dismissal. It is to treat your mind the way an elite program treats a joint or a cardiovascular system: measure it, understand your individual biology, intervene with evidence-based tools, and verify the result with data. A Peptide Longevity Plan™ built on a genetic foundation and an honest read of the science is not a magic syringe. It is something better — a way to stop guessing. For the 70% of us carrying some trauma and the 100% of us aging, that is the whole game: not just more years, but more years with the lights on upstairs.
A note, because this topic is serious: PTSD, trauma, and chronic stress are medical conditions, and nothing here is medical advice or a substitute for a licensed professional. If you or someone you know is struggling, please reach out to a qualified clinician — and if you are in crisis, contact your local emergency services or a crisis line such as 988 in the U.S. The science of measurement is exciting precisely because it gets more people to the help that already works.
Sign up for FREE daily Longevity Club Workshops, or join the Affiliate Program (pays 20%).
About the Author
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data and leverages proprietary Digital Twin for Predictive Peptide Performance™ technology, wearable data, and biomarker data to deliver personalized optimization and longevity recommendations. A 3x technology/AI company CEO with 2 successful exits, Tony has completed 3 Full Ironman Triathlons (140.6 mi) since 2019. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University, and has worked with the US Olympic Team, the NBA, NFL, MLB, NASA, Google, Microsoft, and Netflix, among others. He also served as a US Navy Officer commanding an emergency response team aboard a destroyer.
Disclaimer: This article is for educational purposes and is not medical advice, diagnosis, or treatment. Health decisions should be made with a qualified clinician who can interpret your individual results.
Endnotes
- Marmar CR, et al. Speech-based markers for PTSD; NYU Langone reporting notes that more than 70% of adults worldwide experience a traumatic event and up to ~12% in some countries develop PTSD. NYU Langone News.
- Ressler KJ, et al. "Post-traumatic stress disorder is associated with PACAP and the PAC1 receptor." Nature 470:492–497 (2011); PTSD prevalence ~5–10%, ~30–40% heritability, ~2× higher risk in women.
- Centre for Addiction and Mental Health (CAMH). "Study finds potential new treatment for preventing PTSD." Jan 13, 2020 — Canada highest of 24 nations; 9.2% lifetime PTSD (per British Journal of Psychiatry).
- Frijling JL, van Zuiden M, Koch SBJ, … Olff M. "Efficacy of oxytocin administration early after psychotrauma in preventing PTSD (BONDS): study protocol of an RCT." BMC Psychiatry 14:92 (2014).
- van Zuiden M, Frijling JL, Nawijn L, … Olff M. "Intranasal Oxytocin to Prevent PTSD Symptoms: A Randomized Controlled Trial in Emergency Department Patients." Biological Psychiatry 81(12):1030–1040 (2017) — benefit concentrated in high acute-symptom subgroup.
- Dumont GJH, Olff M, et al. "Oxytocin for the treatment of PTSD?" Amsterdam UMC research portal — effects small; clinical significance to be determined.
- Morgan CA, Wang S, Southwick SM, Rasmusson A, Hazlett G, Hauger RL, Charney DS. "Plasma neuropeptide-Y concentrations in humans exposed to military survival training." Biological Psychiatry 47:902–909 (2000).
- Rasmusson AM, Hauger RL, Morgan CA, Bremner JD, Charney DS, Southwick SM. "Low baseline and yohimbine-stimulated plasma NPY levels in combat-related PTSD." Biological Psychiatry 47:526–539 (2000).
- Kautz M, Charney DS, Murrough JW. "Neuropeptide Y, resilience, and PTSD therapeutics." Neuroscience Letters 649:164–169 (2017).
- Ressler KJ, Mercer KB, Bradley B, Jovanovic T, et al. Nature 470:492–497 (2011); ADCYAP1R1 SNP rs2267735 within an estrogen-response element predicts PTSD in women.
- Li H, Su P, … Liu F. CAMH / University of Toronto. Glucocorticoid receptor–FKBP51 complex elevated in PTSD; disrupting peptide blocks fear-memory encoding/recall in preclinical models. Journal of Clinical Investigation (2020); CAMH news release, Jan 13, 2020.
- Zozulia AA, et al. "Efficacy and possible mechanisms of action of selank in generalized anxiety disorder and neurasthenia." Zh Nevrol Psikhiatr (2008); FDA compounding concerns for Semax/Selank (limited human safety data, immunogenicity, impurities). Neither is FDA-approved in the U.S.
- Hendershot CS, Bremmer MP, Paladino MB, et al. "Once-Weekly Semaglutide in Adults With Alcohol Use Disorder." JAMA Psychiatry 82(4):395–405 (2025). ClinicalTrials.gov NCT05520775.
- Lähteenvuo M, Tiihonen J, et al. "Repurposing semaglutide and liraglutide for alcohol use disorder." JAMA Psychiatry 82(1):94–98 (2025); within-individual analysis of 227,866 individuals with AUD.
- Marmar CR, Brown AD, et al. Speech-based PTSD classification using random-forest ML; ~89% accuracy from 18 of 40,000+ voice features. Depression and Anxiety (2019); NYU Langone / SRI International; funded in part by Cohen Veterans Bioscience.
- Ellipsis Health vocal-biomarker validation, including feasibility in a senior population (AUC ~0.82 vs PHQ-8/GAD-7). PMC9037748.
- Institute for Protein Design, University of Washington. "David Baker wins Nobel Prize for protein design" (2024 Nobel Prize in Chemistry, shared with Hassabis and Jumper, DeepMind). ipd.uw.edu.
- Rettie S, Juergens D, Adebomi V, … Bhardwaj G, DiMaio F, Baker D. "RFpeptides" — de novo macrocyclic peptide binder design. Nature Chemical Biology (2025); licensed to Vilya.
- Heinz MV, Jacobson NC, et al. "Randomized Trial of a Generative AI Chatbot for Mental Health Treatment (Therabot)." NEJM AI (March 27, 2025); N=210; ClinicalTrials.gov NCT06013137.
- Torous J (Beth Israel Deaconess Medical Center), commentary on the Therabot trial. STAT News, AI Prognosis (April 2025).
- Stanford HAI. "New Center to Drive AI Innovation in PTSD Treatment" (CREATE Center; co-directors Wiltsey Stirman and Eichstaedt; $11.5M NIH grant; PTSD ~7% of U.S. population). Aug 28, 2025.
- Fitzpatrick KK, Darcy A, Vierhile M. "Delivering CBT to Young Adults With Symptoms of Depression and Anxiety Using a Fully Automated Conversational Agent (Woebot): An RCT." JMIR Mental Health 4(2):e19 (2017).
- Wysa clinical evidence: FDA Breakthrough Device Designation following a peer-reviewed JMIR trial in chronic pain with associated depression/anxiety; NICE "digital front door" evaluation within NHS Talking Therapies. wysa.com/clinical-evidence.
- Function Health $298M Series B (Nov 2025); biomarker-platform comparison and the Function v. Superpower advertising litigation (Jan 2026) on the definition of a "biomarker." ArentFox Schiff, Longevity Lens (2026).