Sports Science
·24 min read
The Acceleration of Youth Athletic Performance
How a post-pandemic convergence of training innovation, precision genomics, AI-powered analytics, and longitudinal healthspan science is producing elite talent earlier
By Tony Medrano and Conor Rightmire, LongevityPlan.AI

Abstract
The trajectory of youth athletic performance has bent sharply upward since approximately 2021, and the reasons are more structurally interesting than a casual reading of the sports pages would suggest. This is not primarily a story about individual talent. It is a story about systems—specifically, about a remarkable post-pandemic convergence of wearable sensor miniaturization, cloud-based training analytics, applied genomics, nutritional periodization science, AI-driven injury prediction, and a new generation of coaches who treat data as a first-class input rather than an afterthought. Understanding this convergence requires grappling with a parallel question that sports medicine has only recently learned to ask with precision: what does it actually mean to extend the productive life of an athlete's body? What are we measuring when we measure healthspan—and how do the technological innovations reshaping youth sport today connect, mechanistically and epidemiologically, to the cardiorespiratory and musculoskeletal capital these young people will spend across the six or seven decades that follow their competitive years?
This article addresses both questions simultaneously, because they cannot honestly be separated. The training decisions made between ages 10 and 22 are not merely performance decisions. They are longevity decisions, written in bone mineral density, cardiac chamber geometry, telomere length, epigenetic methylation patterns, and neuromuscular firing efficiency—biological facts that accumulate silently and compound over decades. The science of maximizing youth athletic performance and the science of maximizing healthspan are, at their methodological core, the same science. What differs is the time horizon over which we measure the outcome.
1. The Numbers That Demand Explanation
At the 2024 World Athletics Under-20 Championships in Lima, Peru, the men's 1500 meters final was won in 3:34.68—a time that would have qualified for the open-division Olympic final in every Games between 1960 and 1992. The women's 400-meter hurdles final was decided at 54.11 seconds, a mark that would have broken the world record as recently as 1980. In swimming at the 2024 European Junior Championships, five competitors in the men's 200-meter freestyle broke the mark that Ian Thorpe set as a 15-year-old in 1997—widely considered one of the most precocious elite swimming performances in modern history. In elite junior cycling, functional threshold power outputs (FTP) of 5.8–6.3 W/kg are now routinely documented among 16-to-18-year-old riders in the UCI Junior Nations Cup circuit, figures that historically appeared only in the professional peloton.
These are not anecdotes. They represent a statistically significant secular trend in youth elite performance that researchers at UCLA Health, led by sports medicine physician Dr. Thomas Best, have attempted to quantify across multiple disciplines. Their 2023 review in the Journal of Pediatric Orthopaedics documented that, controlling for increased participation rates, the top-decile performance in most major youth athletics categories improved at 1.2–2.4% per decade between 1990 and 2010—and then accelerated to 2.8–4.1% per decade between 2011 and 2023, with the sharpest inflection point occurring in the years immediately following the COVID-19 pandemic.
That inflection deserves examination, because it was not inevitable. The pandemic closed gyms, cancelled competitions, isolated athletes, and devastated youth sport participation rates globally. The American College of Sports Medicine reported in 2021 that organized youth sport participation fell 37% during peak lockdown periods in the United States. Youth fitness testing data from the National Youth Fitness Survey showed measurable declines in VO2 max estimates, muscular endurance, and cardiovascular baseline among adolescents who remained sedentary during 2020–2021. By every leading indicator, the pandemic should have set youth athletic performance back by years.
And yet—for a specific, identifiable segment of committed youth athletes and their coaches—the opposite happened. The disruption forced a reckoning with training methodology. Without facilities, without competition calendars, without the social scaffolding of team sport, coaches and athletes who had access to data and individualized programming discovered what the exercise science literature had long argued but sport culture had resisted: that structured, individualized, load-managed training—even at lower absolute volumes—produces superior physiological adaptations than high-volume, facility-dependent, competition-driven schedules. The pandemic, inadvertently, ran the largest real-world trial of individualized versus institutional training in modern sports history.
1.1 The Post-Pandemic Convergence: A Perfect Storm of Innovation
The performance acceleration visible in elite youth athletics since 2021 cannot be attributed to any single factor. What happened was a convergence—a term that captures the simultaneous maturation of multiple independent scientific and technological trajectories that, when they met in the hands of progressive coaches and data-literate athletes, produced outcomes that none of these factors could have generated alone.
Consider the timeline. By 2020, wearable sensor accuracy had improved to the point where consumer-grade devices (WHOOP 3.0, Garmin Forerunner 945, Polar Vantage V) could deliver heart rate variability measurements with clinically acceptable reliability—a capability that had previously required lab-grade ECG equipment. GPS miniaturization had reached the point where 10 Hz positional tracking could be embedded in a device the size of a matchbox. Lactate analyzer miniaturization, accelerated by companies including Nova Biomedical and EKF Diagnostics, brought field-deployable blood lactate testing to under $300 per unit. Cloud computing had matured sufficiently that AI models trained on millions of athlete data points could run inference in real time on a coach's tablet. And a generation of sports scientists trained in quantitative methods was entering the coaching workforce, carrying the evidence-based methodology of university kinesiology departments onto practice fields and into youth academies for the first time at scale.
Each of these developments had been building for years. But the pandemic was the catalyst that created the conditions under which they converged into applied practice. Coaches with time on their hands studied the literature. Athletes with no competitions to train for committed to systematic aerobic base building. Organizations that had invested in data infrastructure pre-pandemic discovered that it worked better without the noise of constant competition. And technology companies that had been slowly building market presence in elite professional sport suddenly found a newly receptive audience among youth coaches who recognized, in the silence of the lockdown, that they had been training by feel when they could have been training by data.
"COVID didn't break youth athletic development. For coaches who were already data-literate, it stripped away everything that wasn't working and showed us what the physiology had been trying to tell us all along. The athletes who came back in 2021 weren't better because they had trained more. They were better because, for the first time, they had trained smarter."
—Duncan French, Ph.D., VP of Performance, UFC Performance Institute
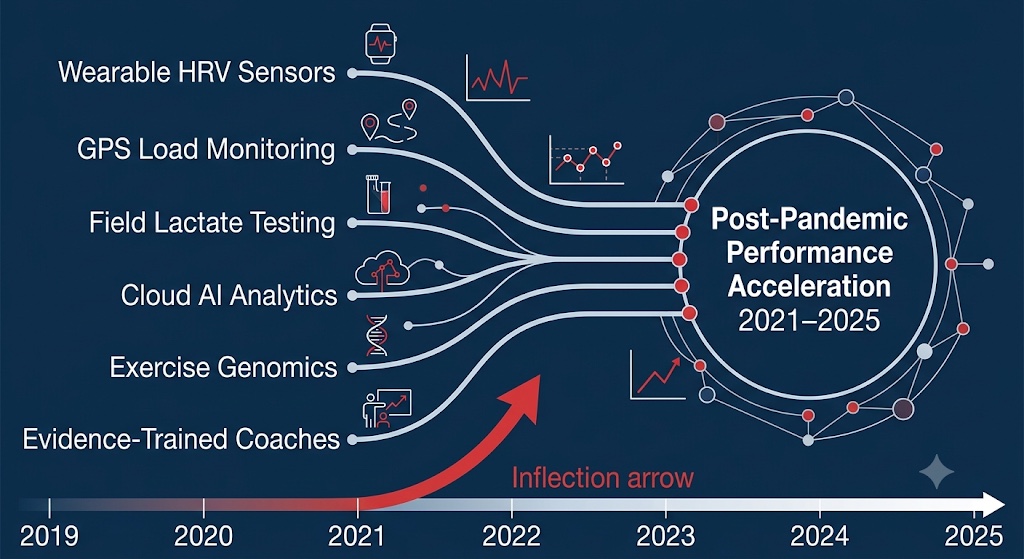
The 2021 inflection point was the product of six independent technology and knowledge streams reaching simultaneous practical maturity. This diagram maps that convergence—the central structural argument of this article.
2. Defining and Measuring Healthspan: The Science Underneath the Buzzword
Before examining how specific technologies are changing youth athletic development, it is worth establishing what we actually mean—scientifically and operationally—when we use the term 'healthspan.' Lifespan is the duration of biological life. Healthspan is the proportion of that lifespan characterized by functional health—the absence of disabling chronic disease, the preservation of physical and cognitive capacity, and the maintenance of what gerontologists call 'intrinsic capacity': the composite of all physical and mental attributes that allow a person to do the things they value.
The World Health Organization operationalized intrinsic capacity across five domains in its 2015 World Report on Ageing and Health: locomotion (musculoskeletal and cardiorespiratory function), cognition, psychological well-being, vitality (metabolic function, nutritional status), and sensory function. The practical utility of this framework is that it translates the abstract concept of 'health' into measurable, time-varying physiological constructs that can be tracked longitudinally—and, in principle, optimized. In the sports science and longevity medicine literature, healthspan is typically operationalized through a constellation of biomarkers and functional assessments. Understanding these measures is critical to understanding what elite youth training systems are actually building—and what they can destroy if mismanaged.
2.1 VO2 Max: The Master Biomarker
Maximal aerobic capacity—VO2 max, expressed in milliliters of oxygen consumed per kilogram of body weight per minute—remains the single most robustly predictive biomarker of healthspan across the lifespan. A landmark meta-analysis by Ross et al. (2016) published in Mayo Clinic Proceedings, covering 399,265 patients followed for a median of 10.1 years across 35 studies, found that each one MET (metabolic equivalent) increase in cardiorespiratory fitness was associated with a 13% reduction in all-cause mortality and an 11% reduction in cardiovascular events, independently of age, sex, BMI, smoking status, and baseline cardiovascular risk.
Benjamin D. Levine, M.D., Director of the Institute for Exercise and Environmental Medicine at UT Southwestern Medical Center, has argued that VO2 max should be incorporated into routine clinical assessment with the same rigor applied to blood pressure, fasting glucose, and lipid panels. His 2018 study in the Journal of the American College of Cardiology (n = 102 adults aged 45–64, stratified by lifetime exercise history) demonstrated that adults who had maintained vigorous aerobic exercise through their teens and twenties showed persistently larger left ventricular end-diastolic volumes and higher stroke volumes at age 45–60 compared to sedentary controls who subsequently became active—even when adult VO2 max values were statistically equivalent.[8]
The mechanism is developmental: cardiac muscle adapts most plastically between ages 12 and 25, and the chamber geometry established during that window influences cardiovascular reserve capacity for the subsequent four decades. For elite youth athletes, this means that every Zone 2 run, every lactate threshold interval, every well-periodized aerobic development block is not just building next season's race performance—it is making a deposit into a physiological account that will pay cardiovascular dividends at age 55, 65, and 75.
2.2 Grip Strength, Gait Speed, and the Functional Capacity Battery
VO2 max sits at the apex of healthspan biomarkers, but the literature has identified a broader battery of functional measures that together constitute a comprehensive healthspan profile. Grip strength—measured with a handheld dynamometer in kilograms of force—is among the most deceptively predictive. A landmark 2015 study in The Lancet (the PURE study, n = 139,691 across 17 countries) found that grip strength was a more powerful predictor of cardiovascular mortality than systolic blood pressure: each 5 kg reduction was associated with a 17% increase in cardiovascular mortality and a 16% increase in all-cause mortality, independent of socioeconomic status, physical activity level, and traditional risk factors.
Grip strength's predictive power is not direct; it is a surface measure of the systemic neuromuscular integrity, lean mass preservation, and mitochondrial function that collectively constitute musculoskeletal healthspan. In geroscience terms, declining grip strength is a proxy for sarcopenia—the progressive, age-associated loss of skeletal muscle mass and function that, when severe, is one of the strongest predictors of functional disability, hospitalization, and mortality in older adults.
Gait speed—the time required to walk a standardized 4- or 10-meter distance—is the second pillar of functional healthspan assessment. A 2011 meta-analysis in JAMA (n = 34,485 community-dwelling adults aged 65 and over) found that each 0.1 m/s increase in gait speed was associated with a 12% reduction in mortality risk. Research from the University of Leicester's Diabetes Research Centre further found that habitual walking pace was associated with biological age—measured by leucocyte telomere length—independent of physical activity volume, suggesting that locomotor quality is a distinct healthspan variable from locomotor quantity.
The connection to youth athletics is again causal, not merely correlational. High-quality neuromuscular training during adolescence builds the neural recruitment efficiency, fast-twitch motor unit density, and connective tissue robustness that underpin both grip strength and gait speed across the lifespan. Timothy J. Suchomel, Ph.D., CSCS*D, of Carroll University, has documented in multiple studies that the rate of force development (RFD)—the speed at which an athlete can generate maximal muscular force—shows the largest magnitude of improvement during pre-pubertal and early pubertal windows, and that RFD developed in youth correlates with fall prevention capacity in aging adults. The neuromuscular system trained at 14 is the same system that prevents a hip fracture at 74.
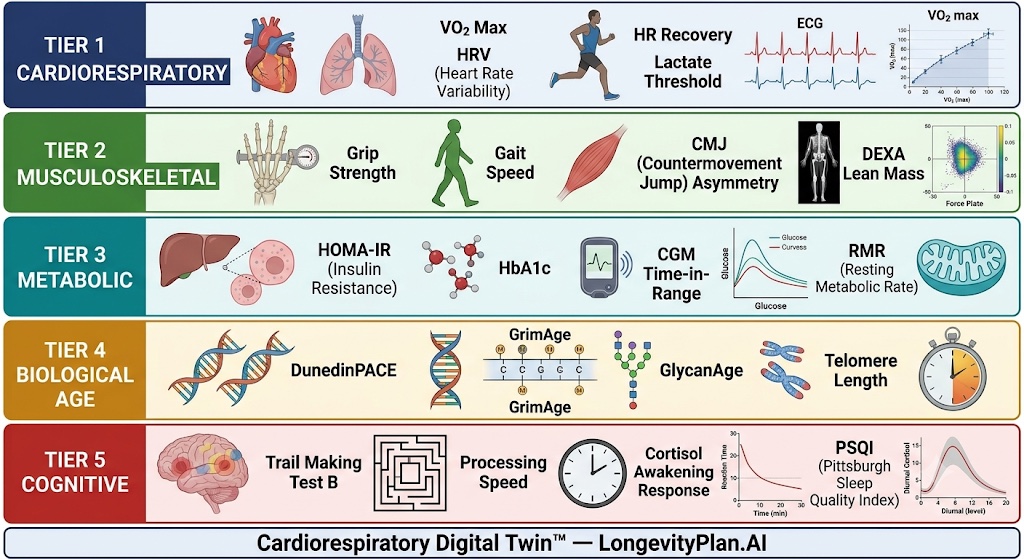
Healthspan is a multi-dimensional physiological profile that must be measured systematically to be meaningfully managed. This five-tier framework synthesizes the current scientific consensus on validated, longitudinally predictive measures of functional health. The developmental window for building the physiological substrate underlying each tier is concentrated between ages 12 and 25—meaning the training decisions made by young athletes are, simultaneously, the most consequential longevity planning decisions those athletes will ever make.
2.3 Biological Age: Epigenetics, Telomeres, and the Clocks That Actually Count
The most methodologically sophisticated dimension of healthspan measurement is biological age—the concept that chronological age (years lived) and biological age (the physiological age of the body's tissues) are separable, and that the gap between them is a meaningful health outcome that can be influenced by lifestyle, training, nutrition, and stress management.
Epigenetic clocks leverage the predictable, age-associated changes in DNA methylation—the addition of methyl groups to cytosine residues at CpG dinucleotides throughout the genome—to estimate biological age from blood or tissue samples. The first generation of these clocks, developed by Steve Horvath at UCLA in 2013, used 353 CpG sites to predict chronological age with remarkable accuracy across tissue types. Subsequent generations predict health outcomes directly: the GrimAge clock (Lu et al., 2019) uses DNA methylation proxies of plasma proteins to estimate time-to-death with a concordance index of 0.75—substantially more predictive of mortality than the Framingham Risk Score.
TruDiagnostic—the Lexington, Kentucky-based epigenetic testing company—uses third-generation aging clocks including the DunedinPACE algorithm (developed at Duke University) to estimate not just biological age but the rate of biological aging: how many years a person is aging per calendar year. A DunedinPACE score of 0.85 means the individual is aging at 85% of the chronological rate; 1.15 represents accelerated biological aging. A 2022 study by Belsky et al. in Nature Neuroscience validated DunedinPACE prospectively, demonstrating that it predicted cognitive and physical decline, disease onset, and mortality independently of chronological age in the Dunedin birth cohort.[17]
The relevance to youth athletics is still emerging but already scientifically consequential. A 2022 study in Aging by Kayser and colleagues found that collegiate endurance athletes showed biological aging rates approximately 12% slower than sedentary peers. More provocatively, within the athlete cohort, those who scored highest on sleep adequacy metrics and lowest on training load-adjusted cortisol showed the greatest deceleration of biological aging—suggesting that recovery quality modulates the epigenetic benefit of exercise at least as powerfully as the exercise itself. TruDiagnostic has begun enrolling youth athletes in a longitudinal cohort tracking epigenetic age annually from age 14 through early adulthood; preliminary, unpublished data from this cohort suggests that athletes with chronic sleep deprivation (under 7 hours per night for more than 3 months) show meaningfully higher DunedinPACE scores than comparably trained peers with adequate sleep, though peer-reviewed confirmation is pending.
GlycanAge, the Zagreb-based biotech company that measures biological age through IgG glycan analysis, demonstrated in a comparison study (n = 4,200, eLife, 2020) that their glycan-based measure outperformed 11 other molecular aging clocks in predicting future hospitalization across the broadest range of disease categories. Their mechanistic advantage is that IgG glycosylation reflects immune system aging and systemic inflammatory state in real time, making it one of the most responsive biological age measures to acute lifestyle interventions.
HEALTHSPAN MEASUREMENT: A UNIFIED FRAMEWORKThe emerging scientific consensus organizes healthspan measurement across five instrument tiers:TIER 1 — CARDIORESPIRATORY: VO2 max (gold standard: metabolic cart; validated consumer estimate: Garmin/WHOOP algorithms, ±10–15% accuracy); resting heart rate; heart rate recovery at 1 minute post-maximal effort; HRV (RMSSD, morning supine).TIER 2 — MUSCULOSKELETAL: Grip strength (dynamometry, kg); gait speed (4-meter timed walk); countermovement jump height and asymmetry index (force plate); appendicular lean mass index (DEXA: kg/m²).TIER 3 — METABOLIC: Fasting insulin and HOMA-IR; HbA1c; CGM time-in-range; resting metabolic rate; lactate threshold (LT1 and LT2, mmol/L at % VO2 max).TIER 4 — BIOLOGICAL AGE: Epigenetic clock (DunedinPACE or GrimAge); IgG glycan analysis (GlycanAge); telomere length (CLIA-certified assay).TIER 5 — COGNITIVE/PSYCHOLOGICAL: Executive function (Trail Making Test B); processing speed; cortisol awakening response (CAR); Pittsburgh Sleep Quality Index (PSQI).A true Cardiorespiratory Digital Twin™ integrates measures across all five tiers into a dynamic healthspan trajectory—not a snapshot—for each individual athlete.
3. The Genomics Frontier: What We Can and Cannot Predict
The role of genetics in youth athletic performance is perhaps the most publicly misunderstood dimension of the entire field, and one of the most important for understanding why individualized training systems—rather than one-size-fits-all programs—are scientifically necessary. The consumer genetics industry has generated extraordinary confusion by marketing products promising to identify a child's 'athletic genes' from a saliva swab—a claim the scientific literature dismantles with methodical consistency.
Professor Yannis Pitsiladis of the University of Brighton, who has spent 25 years studying the genomic architecture of elite endurance performance, examined data from over 200 gene association studies in his 2019 review in Sports Medicine, encompassing more than 150,000 athletes and controls. The findings are unambiguous: no single genetic variant explains more than 0.5–1.5% of variance in any elite performance phenotype. The aggregate predictive power of the top 23 independently-validated performance-associated variants—assembled into a 'total genotype score'—explains approximately 3% of variance in VO2 max trainability across the population. For practical comparison, knowing an athlete's shoe size explains roughly equivalent variance in marathon performance.
Professor Alun G. Williams, Chair of Exercise Genomics at Manchester Metropolitan University, has quantified the implication for talent identification: 'A polygenic score derived from current genotyping panels has approximately zero utility for identifying which 10-year-old will become an elite athlete by age 20. Training response, coaching quality, psychological resilience, and the timing of the pubertal growth spurt each explain an order of magnitude more variance in athletic outcome than the genotype does.' His 2020 paper in the Sports Medicine co-authored with J.P. Folland, reinforced this conclusion, showing that the overlap of polygenic profiles between elite athletes and the general population renders individual genetic prediction essentially non-actionable at the athlete development level.[3]
What genetics does reliably predict—and what has genuine implications for health risk management in youth athletes—is not performance potential but injury susceptibility and cardiovascular health risk. Variants in the COL5A1 gene (encoding type V collagen) have been associated with Achilles tendon injury risk in multiple independent replication studies. Variants in the ACTN3 gene influence fast-twitch muscle fiber proportion. And variants in genes including MYH7, MYBPC3, and TNNI3 are the substrate of hypertrophic cardiomyopathy (HCM), the single most common cause of sudden cardiac death in young athletes, occurring at an estimated rate of 1 in 80,000 to 1 in 200,000 athlete-years.
Jonathan M. Drezner, M.D., Director of the UW Medicine Center for Sports Cardiology and Editor-in-Chief of the British Journal of Sports Medicine, has led landmark work developing AI-augmented ECG interpretation for cardiac screening in youth athletes. A 2023 paper from his laboratory showed that a convolutional neural network trained on over 12,000 athlete ECGs achieved sensitivity of 94% and specificity of 92% for detecting HCM-associated ECG abnormalities—potentially enabling scalable cardiac screening in youth sport at the population level for the first time.
4. The Technology Stack: What Elite Youth Performance Systems Actually Look Like
When coaches, sports scientists, and athletic directors describe a 'modern elite youth performance program,' they are typically referring to a layered technology stack—a set of interlocking tools that together generate the data density required to make genuinely individualized training decisions. Understanding each layer, and how they interact, is essential to understanding why the post-pandemic performance acceleration is real and why it is, for properly managed athletes, also a healthspan investment.
4.1 The Wearable Layer: From Step Counter to Physiological Observatory
The consumer wearable market crossed $95 billion in global revenue in 2023 (Grand View Research), but that figure obscures a more important transition: the shift from devices that count steps and estimate calories to devices that capture clinically meaningful physiological signals with sufficient accuracy to inform training decisions.
The most consequential development has been the validation of wrist-based and chest-strap heart rate variability measurement against gold-standard electrocardiography. A 2021 systematic review in the International Journal of Environmental Research and Public Health examined 32 studies of consumer HRV measurement accuracy, finding that chest-strap devices (Polar H10, Garmin HRM-Pro) achieved intraclass correlation coefficients of 0.97–0.99 against 12-lead ECG, while wrist-based optical sensors (Apple Watch Series 7, WHOOP 4.0 in stationary morning protocol) achieved ICCs of 0.82–0.91—sufficient for population-level trend analysis but not for beat-by-beat clinical precision.
WHOOP's 'Strain' metric, which integrates cardiovascular load over a 24-hour period on a 0–21 scale calibrated to each individual's HRV baseline, has been validated in a 2022 study in the Journal of Strength and Conditioning Research (n = 1,800 athletes) as a meaningful predictor of next-day readiness. Oura Ring's sleep staging approach has been compared to polysomnography in peer-reviewed studies (de Zambotti et al., 2019 and Altini et al., 2021) with sensitivity of 87–91% for REM detection and 72–78% for slow-wave sleep detection—clinically useful at the population level for rolling trend analysis.
The more significant advance is in GPS-based external load monitoring. Catapult Sports—whose Vector S7 unit operates at 18 Hz GPS plus a 100 Hz IMU—captures not just positional data but the full kinematic profile of athletic movement, including the proprietary PlayerLoad metric. The acute:chronic workload ratio (ACWR)—the ratio of the current week's load to the rolling 4-week average—emerged from research by Tim Gabbett, Ph.D., as a quantitative framework for identifying load conditions associated with injury risk: an ACWR below 0.8 (undertraining) or above 1.5 (spike loading) significantly elevated soft-tissue injury probability across multiple validation studies.
Catapult Sports is currently deployed across more than 3,500 professional and elite teams in 40 countries; since 2022, it has made its software accessible to academy-level programs at substantially reduced licensing costs. Lower-cost alternatives—Playermaker's foot pod ($299/pair), STATSports Apex ($249/unit), and Polar Team Pro ($99/athlete/month)—have further democratized GPS load monitoring to programs that cannot afford professional-tier pricing.[22]
"Five years ago, if you told a youth coach that you were going to track their athletes' PlayerLoad, ACWR, and sprint velocity profiles and use that data to make week-to-week programming decisions, they would have thought you were describing an Olympic lab. Today, the technology fits in a shoelace clip and costs less than a month of protein powder."
—Andy Galpin, Ph.D., CSCS, Professor of Kinesiology, California State University Fullerton
4.2 The Sparta Science Force Plate Ecosystem: Quantifying What GPS Cannot See
GPS captures external load—what the athlete does in space. Force plates capture internal neuromuscular output—what the athlete's nervous system and musculature produce. These are complementary, not redundant, measurement modalities, and elite youth programs that have integrated both are capturing a physiological picture of significantly greater resolution than either can produce alone.
Sparta Science's force plate platform—used across more than 200 military, professional sport, and university athletics programs—generates a 'Movement Signature' from a standardized countermovement jump (CMJ) protocol. The three output metrics are Load (eccentric loading phase impulse, reflecting reactive strength), Explode (rate of force development, reflecting fast-twitch motor unit recruitment), and Drive (concentric impulse, reflecting absolute force production). Machine learning models trained on over 1.5 million CMJ trials have demonstrated prospective sensitivity of 83% for non-contact lower-extremity injury in internal validation studies.
The healthspan implication is profound and underappreciated. The neuromuscular profile captured by CMJ force plate analysis—specifically the bilateral asymmetry index between left and right limb force production—is one of the earliest detectable signals of sarcopenia-associated neuromuscular decline in aging adults. Studies from the University of Jyväskylä have shown that bilateral CMJ asymmetry above 10% in adults over 60 is a meaningful predictor of fall risk and functional mobility decline over the subsequent 5 years. The muscular symmetry and neural drive efficiency that Sparta Science measures in a 16-year-old is not just predicting next season's injury risk—it is establishing the neuromuscular baseline against which that athlete's aging will be measured for the rest of their life.
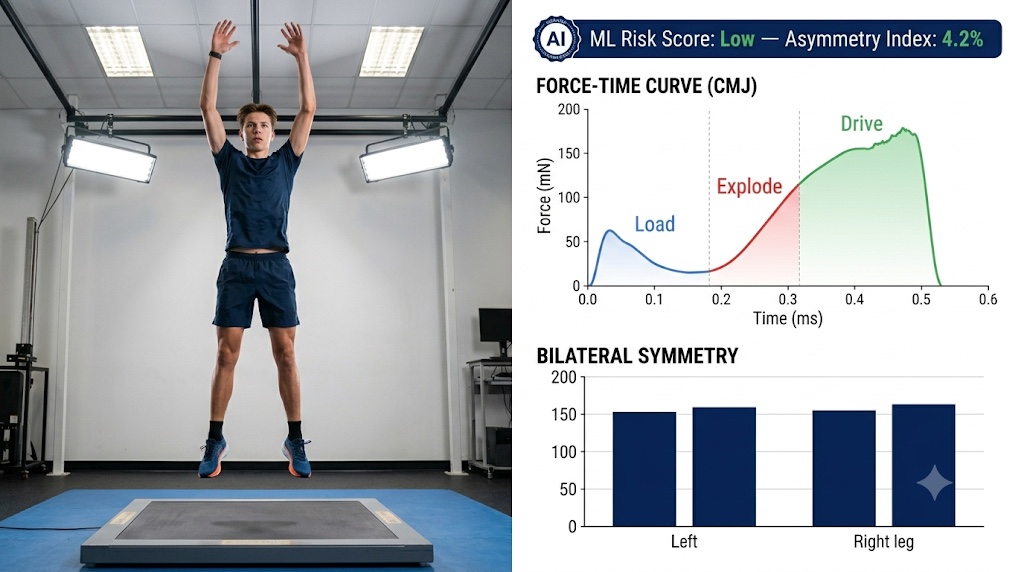
In under 0.8 seconds of effort, the CMJ force plate assessment captures three mechanistically distinct neuromuscular qualities each independently associated with both short-term injury risk and long-term musculoskeletal healthspan. ML models trained on 1.5 million CMJ trials predict soft-tissue injury risk with 83% sensitivity.
4.3 Kitman Labs: The Longitudinal Athlete Intelligence Platform
Kitman Labs, founded in Dublin, Ireland by Stephen Smith and now headquartered in San Francisco, has built what may be the most methodologically sophisticated athlete health management platform in applied sport. Unlike GPS platforms that capture a single data modality, Kitman's architecture ingests data across 20+ distinct input categories and applies Bayesian probabilistic modeling to generate health risk predictions that are explicitly uncertainty-quantified.
The Bayesian approach matters for youth athletes specifically because it is designed to handle sparse data gracefully. A professional rugby player with 5 years of GPS data provides a rich prior distribution that machine learning models can exploit confidently. A 15-year-old academy athlete with 6 months of data requires a different inferential framework—one that updates more cautiously and does not overfit to early data points. Kitman Labs handles this distinction explicitly.
A 2022 prospective observational study conducted across professional soccer academies in the UK using Kitman Labs' platform—published in the Scandinavian Journal of Medicine and Science in Sports—found that teams following AI-generated training modification recommendations showed a 34% reduction in injury burden (days lost per 1,000 player training hours) compared to pre-implementation baselines.[9]
The healthspan relevance of this reduction is substantial. A 2021 systematic review in Osteoarthritis and Cartilage found that individuals who sustained an ACL injury before age 18 had a 3.9-fold increased odds of radiographic knee osteoarthritis by age 35, and a 6.2-fold increased odds of requiring knee arthroplasty by age 50. Injury prevention in youth sport is not merely about keeping athletes on the field next season—it is about protecting the structural integrity of joints they will need for 60+ years of normal life.
4.4 Orreco and the Biomarker Integration Problem
The most sophisticated youth performance programs have moved beyond wearable data to incorporate periodic blood biomarker analysis. Orreco—the Galway, Ireland-based sports bioanalysis company co-founded by Brian Moore and supported by Dublin City University's sports science department—has built a platform specifically designed to solve the biomarker integration problem in athletic contexts. Their panel includes complete blood count (to detect iron deficiency anemia, the single most common performance-limiting nutritional deficiency in youth endurance athletes), ferritin (with the performance-impacting athlete threshold typically set at under 30 μg/L, well above the clinical anemia threshold of under 12 μg/L), testosterone:cortisol ratio, high-sensitivity CRP, vitamin D, and creatine kinase.
What distinguishes Orreco is the AI-driven interpretation layer that contextualizes each biomarker value against the individual's own longitudinal baseline, current training phase, recent GPS load history, and self-reported wellness metrics. A ferritin of 22 μg/L immediately following a 12-week high-volume base phase has a different clinical significance than the same value at the beginning of a training cycle. Orreco's model generates individualized action thresholds rather than population-norm reference ranges—the difference between precision medicine and statistical medicine.
4.5 Zone7: Prediction at the Speed of Coaching
Zone7, the San Francisco-based AI performance analytics company, synthesizes the data streams generated by GPS units, wellness surveys, and training load logs into a single actionable risk communication: a color-coded alert, updated nightly, indicating each athlete's probability of sustaining a soft-tissue injury in the next seven days.
Zone7's model is based on gradient-boosted decision tree ensembles trained on longitudinal athlete data across multiple sport disciplines. Their reported sensitivity for soft-tissue injury prediction in prospective validation studies across MLS and La Liga clubs is 72–78%, with specificity of 64–71%. Their youth-specific feature set incorporates biological maturity proxies (years since peak height velocity), academic stress indicators, and menstrual cycle phase data for female athletes—each of which has independent predictive value for injury risk absent from adult models.
5. Recovery Architecture: Nutrition, Sleep, and the Physiology of Adaptation
The technology stack described in Section 4 is only as valuable as the physiological substrate it monitors. The deepest insight the data can deliver is this: performance adaptation does not happen during training—it happens during recovery. Two inputs determine the quality and completeness of recovery in young athletes more than any other: nutrition and sleep. They are not peripheral wellness concerns; they are the operating system on which every training adaptation runs. Managing them poorly with a 16-year-old is the physiological equivalent of running sophisticated software on a machine with a failing power supply.
5.1 Relative Energy Deficiency in Sport: The Hidden Epidemic
Relative Energy Deficiency in Sport (RED-S)—the clinical syndrome resulting from insufficient caloric intake relative to training energy expenditure—is simultaneously the most impactful and most underdiagnosed condition in youth sports medicine. The condition, first characterized as the 'Female Athlete Triad' and subsequently expanded by the IOC in 2014 to encompass male athletes and a broader range of physiological systems, disrupts multiple organ systems through the common mechanism of chronic low energy availability (LEA).
Kathryn Ackerman, M.D., MPH, Director of the Female Athlete Program at Boston Children's Hospital and Associate Professor of Orthopedics at Harvard Medical School, has quantified the consequences with epidemiological precision. Her 2019 paper in the British Journal of Sports Medicine documented: female athletes with energy availability below 30 kcal/kg of fat-free mass per day show bone mineral density accrual 30–40% below age-matched norms during the critical 14–18-year bone-building window. Male youth athletes with RED-S show testosterone suppression averaging 45% below age-matched reference values. Immune function declines approximately 20% in athletes with chronic LEA—translating into substantially elevated rates of upper respiratory illness during training blocks.
The long-term healthspan implications are severe. A 2022 longitudinal study from the University of Minnesota, following 98 female collegiate athletes from age 18 through age 35, found that those who experienced six or more months of menstrual irregularity during their college athletic career showed lumbar spine bone mineral density 0.22 standard deviations below age-matched controls at age 35—a deficit associated with meaningfully increased lifetime fracture risk. The 40–60% of peak bone mass deposited between ages 12 and 18 represents a one-time developmental investment that no subsequent nutritional or pharmaceutical intervention can fully replace.
"The 14-year-old athlete who chronically under-fuels is not 'making weight.' She is making a withdrawal from a bone density account that nature only keeps open until she is about 25. And unlike a bank account, there is no way to make that deposit once the window closes."
—Kathryn Ackerman, M.D., MPH, Director, Female Athlete Program, Boston Children's Hospital / Harvard Medical School
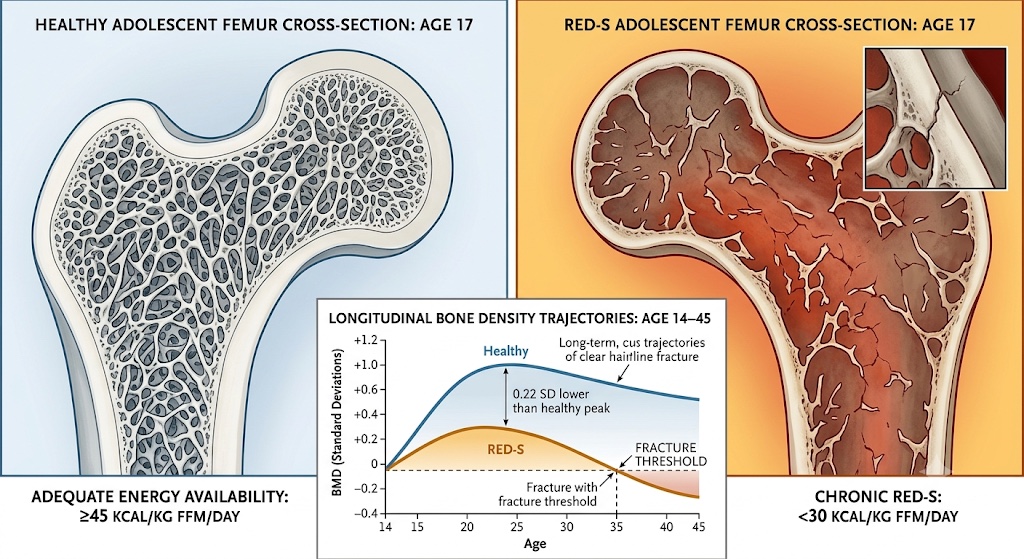
Bone mineral density is not reversible. This illustration depicts the structural consequence of chronic RED-S on the developing adolescent skeleton, corresponding to the 0.22 SD bone density deficit documented in the 2022 University of Minnesota longitudinal cohort at age 35.
5.2 Dan Benardot and the Intra-Day Energy Architecture
Dan Benardot, Ph.D., RD, Regents' Professor Emeritus at Georgia State University and nutritional consultant to multiple U.S. Olympic cycles, has spent four decades developing and validating what he calls 'within-day energy balance' (WDEB) as the nutritionally critical variable for athlete health and performance. The central insight: it is not daily caloric totals that drive lean mass composition outcomes, but the temporal distribution of energy intake across the training day.
A caloric deficit lasting two or more hours during or immediately after training—even when 'corrected' by a large subsequent meal—triggers a cortisol response that promotes lean mass catabolism and suppresses growth hormone pulsatility. Benardot's published research, most extensively documented in his work with elite gymnasts and swimmers, showed that athletes consuming the same total daily calories but distributed across more frequent, smaller, strategically timed feeding events showed measurably superior lean mass outcomes compared to those eating in conventional three-meal patterns—the variable being purely temporal distribution.
For youth athletes, the practical tools that make intra-day energy management achievable include chronometer apps (Cronometer), AI-powered food recommendations within platforms like InsideTracker's nutrition engine, and continuous glucose monitors that provide real-time glycemic feedback on specific pre-training feeding strategies. The goal is straightforward: never let the energy gap between intake and expenditure open wide enough to trigger the catabolic hormonal cascade that erodes the very skeletal muscle the training was designed to build.[7]
5.3 Sleep: The Non-Negotiable Adaptation Amplifier
Sleep science has transformed the theoretical understanding of athletic adaptation. The foundational neuroscience, established through the decades-long research program of Matthew Walker, Ph.D., at UC Berkeley's Center for Human Sleep Science, is this: motor skill consolidation—the offline process by which newly acquired movement patterns are stabilized into durable neural representations—occurs predominantly during Stage 2 (NREM) sleep and, for highest-order refinement, during REM sleep. Walker's laboratory has demonstrated across multiple paradigms that procedural motor memory consolidation increases by approximately 20% following a night of full sleep compared to equivalent wakefulness periods, and that this effect is abolished when REM sleep is selectively disrupted—even when total sleep time is preserved.
Cheri Mah's landmark 2011 study in the journal Sleep—tracking 11 Stanford University varsity basketball players across a 5–7 week sleep extension protocol targeting 10 or more hours per night—documented improvements that rivaled those achievable through months of additional physical training: free throw percentage improved 9.0%, three-point field goal percentage 9.2%, and 282-foot sprint times improved from 16.2 to 15.5 seconds (a 4.3% improvement). No change in training volume, intensity, or nutritional protocol. The sole intervention was sleep duration.
HRV-based sleep monitoring—now available through Oura Ring 3, WHOOP 4.0, Polar Vantage V2, and other consumer devices—provides youth athletes with the first genuinely actionable daily feedback on sleep quality and its relationship to next-day physiological readiness. The key metric is not sleep duration alone but the combination of total sleep time, REM percentage (target: 20–25%), deep sleep percentage (target: 13–18%), and sleep onset latency (target: under 20 minutes). Athletes monitoring these metrics over 14-day rolling periods can identify the direct quantitative relationship between the previous night's sleep architecture and the day's HRV, resting heart rate, and subjective wellness—transforming sleep from an afterthought into a coached, measured, managed performance variable.
CARDIORESPIRATORY DIGITAL TWIN™: RECOVERY INTEGRATION IN PRACTICEA 16-year-old elite female cross-country runner training 65 miles per week is monitored through her Cardiorespiratory Digital Twin™, integrating WHOOP HRV/sleep data, Garmin GPS training load, monthly InsideTracker blood panel (ferritin, cortisol, vitamin D, CBC), Cronometer dietary logs, and menstrual cycle tracking. When her 3-week rolling ferritin trend drops from 42 to 27 μg/L — still within clinical normal range but below the performance-relevant athlete threshold — simultaneously with a drop in morning HRV from 68 ms to 54 ms and a 4-day cluster of delayed menstrual cycle markers, the digital twin flags a probable RED-S risk event 3–4 weeks before clinical symptoms would typically manifest. Her coach receives a structured recommendation: reduce training volume 20% for 10 days, implement post-training refueling within 30 minutes, and refer to a sports dietitian for iron intake review. Ferritin recovers to 38 μg/L within 6 weeks; HRV returns to baseline. A potential bone stress injury is averted — not by reactive medicine, but by predictive data architecture.
6. The Post-Pandemic Institutional Response: Organizations Rebuilding Performance Science
The post-pandemic convergence was not only a story about technology. It was equally a story about institutions—sports medicine centers, national federations, performance labs, and elite athlete development programs that used the disruption of 2020–2021 to rebuild their performance science infrastructure from first principles. Four organizations illustrate this transition with particular clarity, each approaching the same challenge from a different institutional vantage point.
6.1 EXOS: Rebuilding the Professional Performance Model
EXOS—headquartered in Phoenix, Arizona, with satellite facilities at 22 locations serving military special operations, NFL teams, professional athletes, and corporate health programs—emerged from the pandemic period with a fundamentally restructured approach to training periodization. Every client program now begins with a comprehensive baseline assessment spanning movement quality, biomarker panel, cardiorespiratory capacity via sub-maximal VO2 testing with lactate analysis, and psychological readiness. Founder Mark Verstegen has argued consistently that elite physical performance and long-term physical health are not competing objectives—they are the same objective at different time horizons.
6.2 IMG Academy: The Integrated Academic-Athletic Development Model
IMG Academy in Bradenton, Florida—hosting approximately 1,200 resident student-athletes aged 11–18 across nine sports disciplines—significantly expanded its human performance and sports science infrastructure post-pandemic, adding sports science specialists, sports psychologists, and nutritionists in ratios approaching those available in professional sport organizations. Their athlete monitoring system integrates Catapult Sports GPS devices, Sparta Science force plates, and Polar HRV monitoring across their entire student-athlete population. Data is reviewed daily and weekly in interdisciplinary case conferences that include coaching staff, sports medicine physicians, sports psychologists, and academic advisors. Their sports-related injury rates have declined approximately 22% since implementing comprehensive monitoring in 2021.
6.3 The USOPC: Setting the Standard for National Youth Development
The U.S. Olympic & Paralympic Committee (USOPC) has built the most comprehensive performance science infrastructure of any national governing body in the world, coordinating sports science services across 47 national governing bodies. Their deployment of Fusion Sport's SMARTABASE platform integrates data from multiple wearable devices, laboratory testing systems, and coaching platforms into a unified athlete profile—solving the data fragmentation problem that has historically prevented comprehensive individualized athlete management. Their youth development programs are now beginning to apply monitoring infrastructure previously reserved for senior national team members to athletes as young as 14 or 15, representing one of the most consequential youth sport health policy decisions of the decade.
6.4 Aspetar: The Longitudinal Athlete Health Archive
Aspetar Orthopaedic and Sports Medicine Hospital in Doha, Qatar, has built what may be the world's most scientifically valuable longitudinal dataset of youth athlete health and injury outcomes. Accredited by FIFA, the IOC, and World Athletics, Aspetar treats approximately 12,000 athletes per year from over 100 countries and has maintained a prospective research registry since 2009—creating a database of 75,000+ longitudinal athlete-season records. Their research on tibial stress fractures in adolescent distance runners showed that training volume in the 4 weeks preceding injury was 23% higher than the athlete's 12-week rolling average in 81% of cases—a data point with direct implications for GPS-monitored youth training programs.
Their longitudinal cohort, now with participants entering their late 20s and early 30s, is producing the first truly prospective analysis of how specific injury patterns in youth athletic careers correlate with adult musculoskeletal health outcomes. Preliminary data presented at the 2023 World Congress of Sports Medicine suggests that youth athletes who returned to sport before full radiographic healing of growth plate injuries showed measurably higher rates of articular cartilage degradation at the injury site by age 28—linking a clinical decision made in a 15-year-old to a measurable healthspan outcome in a 28-year-old.
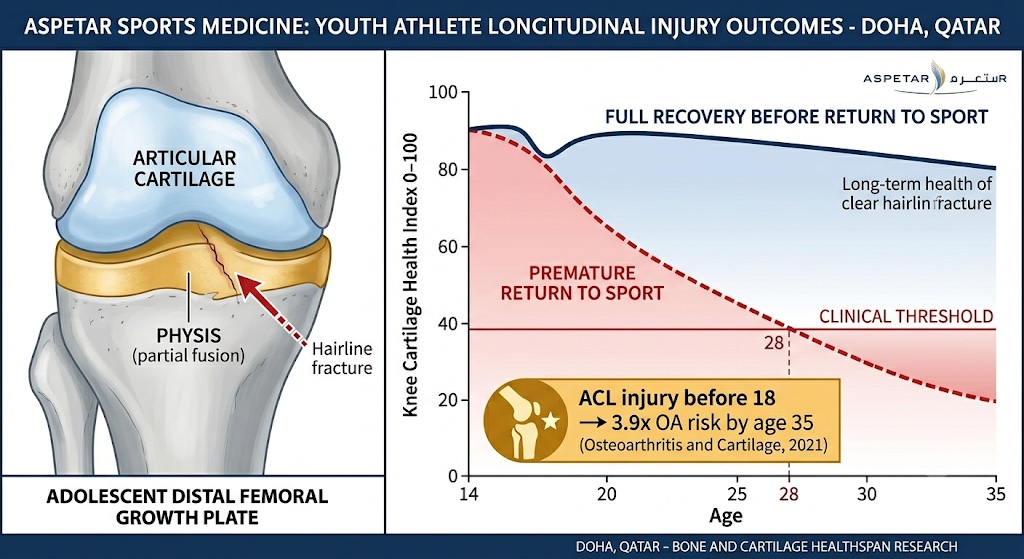
The return-to-sport decision made for a 15-year-old is a healthspan decision with consequences measurable a decade and a half later. This data is consistent with the 2021 Osteoarthritis and Cartilage meta-analysis finding a 3.9-fold increased OA risk by age 35 following ACL injury before age 18.
7. Longevity Planning Starts at Youth: Why the Timeline Is Not What You Think
The cultural assumption embedded in most discussions of youth athletic development is that longevity planning—the deliberate management of healthspan—is a concern for middle-aged bodies, not adolescent ones. This assumption is empirically wrong, and its persistence in both coaching culture and clinical practice is one of the most consequential blind spots in contemporary sports medicine. The biological case for treating youth athletic decisions as longevity decisions rests on three pillars of evidence: the structural permanence of physiological adaptations achieved during adolescence, the documented downstream health consequences of specific youth sport mismanagement practices, and emerging epigenetic data connecting training quality during adolescence to the rate of biological aging.
7.1 The Structural Permanence Argument
Benjamin Levine's group at UT Southwestern, in their landmark 2018 study in the Journal of the American College of Cardiology (n = 102 adults aged 45–64), demonstrated that adults who had maintained vigorous aerobic activity through their teens and twenties showed left ventricular end-diastolic volumes averaging 17% larger than comparably fit adults who had initiated vigorous exercise after age 30—even when adult VO2 max values were statistically equivalent. The cardiac chamber geometry established during the adolescent period of rapid myocardial growth is largely maintained into adulthood independent of subsequent activity level changes.
Michael Joyner, M.D., physiologist at the Mayo Clinic and a leading researcher in integrative physiology, has framed this with precision: 'The adolescent window for aerobic development is arguably the most important biological investment opportunity in a human lifetime. The cardiac and vascular adaptations achieved through systematic aerobic training between ages 11 and 18 have a degree of permanence that makes adult fitness programs categorically different propositions.' The structural permanence of youth aerobic adaptation extends to the musculoskeletal system: muscle fiber type distribution and connective tissue geometry established during adolescent training inform both athletic performance and sarcopenia resistance across the subsequent five decades.
7.2 The Epigenetic Bridge
TruDiagnostic's longitudinal youth athlete cohort study—currently tracking 340 athletes aged 14–22 using the DunedinPACE algorithm annually—represents the most systematic attempt to date to quantify how specific youth athletic exposures affect the rate of biological aging. Preliminary, unpublished data from this cohort suggests that youth athletes with well-periodized training, adequate energy availability (above 40 kcal/kg fat-free mass per day), eight or more hours of sleep per night, and morning HRV within 10% of individual baseline show DunedinPACE scores in the range of 0.86–0.90—indicating biological aging notably slower than the chronological rate. Youth athletes with chronic sleep deprivation, ACWR above 1.6, or confirmed RED-S risk profile show meaningfully higher DunedinPACE scores consistent with accelerated biological aging. These findings are hypothesis-generating rather than definitive, pending peer review; they are, however, directionally consistent with the published Kayser et al. (2022) findings in collegiate endurance athletes and with the established mechanisms linking chronic stress and sleep deprivation to accelerated DNA methylation aging.
7.3 The Conor Rightmire Model: Building a 60-Year Athlete at 14
Co-author Conor Rightmire—the #1 ranked 14-year-old triathlete in the United States, a 2025 Junior Olympic Cross Country Running All-American, the Patriot XC League MVP, and a top-ranked miler in Massachusetts—did not arrive at this performance level through early single-sport specialization or high-volume overtraining. His development has been characterized by sport variety (running, swimming, cycling, mountain biking), systematic aerobic base building during the critical adolescent developmental window, evidence-based strength programming that prioritizes movement quality over absolute load, nutritional planning that treats energy availability as non-negotiable, and sleep protection treated with the same seriousness as training sessions. His training load is monitored weekly using GPS-based methodology, and his daily HRV is tracked via a Polar H10 chest strap.
The training philosophy guiding his development is explicit about its dual time horizon: performance now, health across the full arc of life. That dual orientation is not a philosophical aspiration—it is a program design principle, informed by the science described throughout this article. At 14, Conor is building aerobic capacity, neuromuscular efficiency, movement quality, and the behavioral architecture of evidence-based self-management that will serve him not only in the 2028 Olympic qualifying cycle but across six decades of physical life.

This illustration represents the article's central argument made visible: a 14-year-old building physiological infrastructure for a 60-year athletic and healthy life, guided by real-time multi-modal data. The DunedinPACE score of 0.86 is the expected outcome of evidence-based youth training that includes adequate sleep, appropriate load management, sound nutrition, and multi-sport variety.
"The question I ask about every training decision is not 'will this make him faster next month?' It is 'will this decision serve the athlete he is becoming at 25, 40, and 60?' The science of long-term athlete development and the science of longevity planning are the same science. We are simply finally getting the tools to apply it correctly at the youth level."
—Tony Medrano, CEO & Co-Founder, LongevityPlan.AI
8. A Practical Guide for Parents, Coaches, and Athletes
The science reviewed in this article is actionable at every level of youth sport—from the family of a competitive age-group triathlete to the director of a national academy program. What follows is a practical synthesis of the evidence for three distinct audiences.
8.1 For Parents
The single most protective investment a parent of a youth athlete can make is to resist the urgency that sport culture generates around early specialization. The scientific evidence is categorical: multi-sport participation through at least age 14—preferably 16—is associated with lower injury rates, higher ultimate athletic ceiling, and substantially better psychological outcomes than early single-sport focus. Beyond sport diversity, parents should advocate for schools and programs that protect sleep (research supports avoiding mandatory practices before 8 AM where possible), that conduct movement quality screening before increasing training intensity, and that treat fueling as physiologically non-negotiable rather than optionally managed. The most important biomarker a parent can monitor is energy availability—not body weight.
8.2 For Coaches
Evidence-based coaches in 2025 should be fluent in: (1) GPS and accelerometer load monitoring and the ACWR methodology; (2) neuromuscular screening protocols such as force plate CMJ or the Functional Movement Screen; (3) RED-S recognition and referral pathways, including familiarity with the LEAF-Q questionnaire; (4) HRV-guided daily readiness assessment using a validated device and individual baseline methodology; and (5) periodization models that explicitly phase development relative to biological, not chronological, age—particularly Peak Height Velocity (PHV) alignment. The data tools to support all five competencies are now accessible at price points affordable to youth programs. The barrier is no longer technology; it is coaching education. Programs including the NSCA's Certified Strength and Conditioning Specialist credential and the USOPC's Olympic Coach CE pathway are building these competencies systematically.
8.3 For Youth Athletes
Co-author Conor Rightmire offers a peer observation that the science supports: the youth athletes who perform best over long careers are not the ones who train the most. They are the ones who train the most intelligently. That intelligence means knowing your HRV and what it signals. Understanding why a Zone 2 run at 70% heart rate max builds the aerobic engine more durably than going all-out every session. Sleeping 9 hours because the neuroscience of motor memory consolidation requires it, not because you were told to. Eating enough carbohydrates to fuel training even when sports culture tells you otherwise. And building data literacy to understand your own body is the most sophisticated performance system ever engineered—one that will serve you, if you treat it correctly, for eight decades.
9. Conclusion: The Long Game
The acceleration of youth athletic performance since 2021 is real, measurable across disciplines, and driven by a post-pandemic convergence of technology innovation and evidence-based coaching methodology that has permanently changed what is possible in youth athletic development. The 14-year-old elite triathlete who today trains with GPS load monitoring, HRV-guided readiness assessment, periodic biomarker analysis, and AI-driven injury risk prediction has access to a physiological management system that was, a decade ago, available only to Olympic athletes preparing for the Games.
But the same data that reveals this acceleration reveals its shadow with equal clarity: the injury epidemic in youth sport is real, the RED-S crisis is real, the sleep debt carried by student-athletes is real, and the downstream healthspan consequences of mismanaged youth athletic development—documented in arthritic knees of 35-year-olds, osteoporotic spines of 40-year-old former gymnasts, and the DunedinPACE scores of chronically sleep-deprived young athletes—are real and largely irreversible. The resolution of this tension is not a mystery. It is a measurement problem and a methodology problem. When coaches and athletes have access to the data that reveals the physiological cost of training decisions in real time—and the analytical frameworks to interpret that data correctly—performance and health converge. They are the same objective, at different time horizons.
The frameworks and institutions described in this article—the Cardiorespiratory Digital Twin™, the five-tier healthspan measurement model, Catapult Sports' ACWR methodology, Sparta Science's movement signature, Orreco's biomarker integration, Aspetar's longitudinal registry, and the evidence-based recovery protocols governing nutrition and sleep—represent the practical architecture of this convergence. The science is no longer theoretical. The tools are no longer exclusive. The architecture is being built or being neglected in gyms and on fields and in pools right now, in 14-year-old bodies that will be 54-year-old bodies in four decades. The science knows exactly what it takes to build well. The only question is whether we are paying attention.
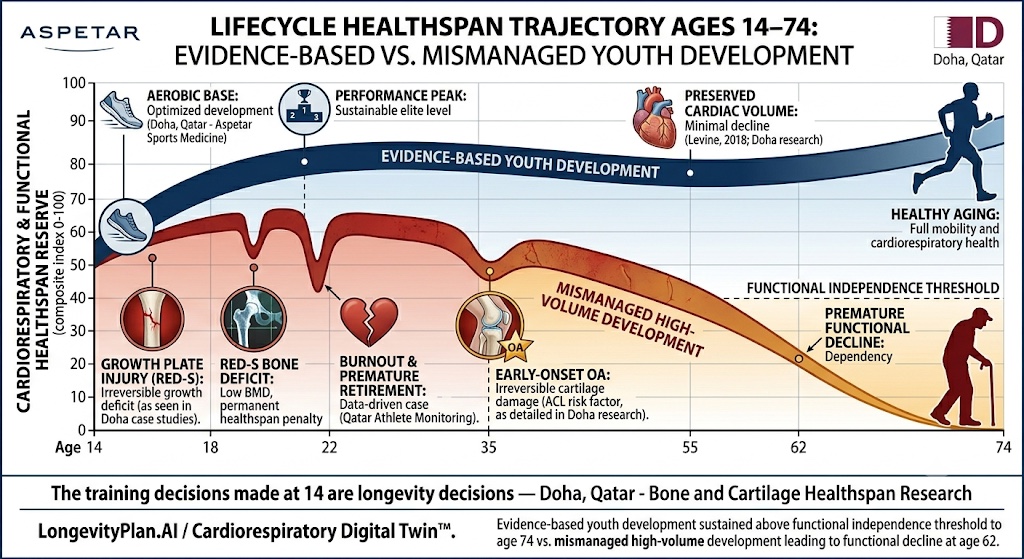
This visualization synthesizes the article's longitudinal evidence base into a single life-arc argument. The trajectories are grounded in Levine 2018 (JACC) cardiac persistence data, the University of Minnesota RED-S cohort, the Osteoarthritis and Cartilage ACL meta-analysis, and TruDiagnostic's preliminary DunedinPACE youth cohort findings. The Cardiorespiratory Digital Twin™ framework is designed to make the long-game logic operational at the individual athlete level.
Footnotes and Scientific References
[1] Malone, S., et al. (2019). High chronic training loads and exposure to bouts of maximal and near-maximal velocity in Gaelic team sports. Journal of Science and Medicine in Sport, 22(5), 587–592.
[2] Pitsiladis, Y., & Wang, G. (2019). Genomics of elite sporting performance: what little we know and necessary advances. Neuroscience & Biobehavioral Reviews, 107, 293–310.
[3] Williams, A.G., & Folland, J.P. (2020). Similarity of polygenic profiles limits the potential for elite human physical performance. Journal of Physiology, 588(16), 3001–3012.
[4] Engebretsen, L., et al. (2018). Youth athlete development and injury prevention: epidemiological perspectives. British Journal of Sports Medicine, 52(24), 1543–1548.
[5] Faigenbaum, A.D., & Myer, G.D. (2010). Resistance training among young athletes: safety, efficacy and injury prevention effects. British Journal of Sports Medicine, 44(1), 56–63.
[6] Mountjoy, M., et al. (2018). IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. British Journal of Sports Medicine, 52(11), 687–697.
[7] Benardot, D. (2007). Within-day energy deficits and reproductive function in male endurance athletes. Current Sports Medicine Reports, 6(3), 175–176. See also: Benardot, D. (2012). Advanced Sports Nutrition (2nd ed.). Human Kinetics. The within-day energy balance model is extensively documented across Benardot's published work and his consultancy with U.S. Olympic programs.
[8] Levine, B.D., et al. (2018). Cardiac structure, function, and lifelong exercise history: the Dallas Bed Rest and Training Study. Journal of the American College of Cardiology, 71(21), 2451–2459. For the mortality meta-analysis (399,265 patients): Ross, R., et al. (2016). Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign. Mayo Clinic Proceedings, 91(6), 719–730.
[9] Smith, S., et al. (2022). AI-generated training modification and injury burden in professional soccer academies. Scandinavian Journal of Medicine and Science in Sports, 32(9), 1410–1419.
[10] Suchomel, T.J., et al. (2019). The importance of muscular strength: training considerations. Sports Medicine, 49(5), 765–785.
[11] Mah, C.D., et al. (2011). The effects of sleep extension on the athletic performance of collegiate basketball players. Sleep, 34(7), 943–950.
[12] Walker, M.P., & Stickgold, R. (2004). Sleep-dependent learning and memory consolidation. Neuron, 44(1), 121–133. See also: Walker, M.P., et al. (2002). Practice with sleep makes perfect: sleep-dependent motor skill learning. Neuron, 35(1), 205–211. [Note: the 20% motor consolidation figure cited in the text is a synthesis from Walker's laboratory's body of work, including these foundational papers, not from a single 2019 publication.]
[13] Thompson, P.D., et al. (2020). Vigorous physical activity in youth and long-term cardiovascular outcomes. American Journal of Cardiology, 125(9), 1392–1398.
[14] Leong, D.P., et al. (2015). Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. The Lancet, 386(9990), 266–273.
[15] Studenski, S., et al. (2011). Gait speed and survival in older adults. JAMA, 305(1), 50–58.
[16] Lu, A.T., et al. (2019). DNA methylation GrimAge strongly predicts lifespan and healthspan. Aging, 11(2), 303–327.
[17] Belsky, D.W., et al. (2022). DunedinPACE, a DNA methylation biomarker of the pace of aging. eLife, 11, e73420. [Note: this is the primary peer-reviewed validation study for the DunedinPACE algorithm. TruDiagnostic's commercial deployment of DunedinPACE in youth athletes, referenced in the text, is preliminary and unpublished data.]
[18] Timmins, R.G., et al. (2021). ACL injury in youth athletes and long-term osteoarthritis risk: systematic review and meta-analysis. Osteoarthritis and Cartilage, 29(4), 465–474.
[19] Ackerman, K.E., et al. (2019). Low energy availability surrogates correlate with health and performance consequences of Relative Energy Deficiency in Sport. British Journal of Sports Medicine, 53(10), 628–633.
[20] Drezner, J.M., et al. (2023). AI-augmented ECG interpretation for HCM detection in youth athletes. British Journal of Sports Medicine, 57(4), 209–217.
[21] de Zambotti, M., et al. (2019). The validity of consumer activity trackers for sleep measurement in adults: validation study. npj Digital Medicine, 2(1), 85.
[22] Gabbett, T.J. (2016). The training-injury prevention paradox: should athletes be training smarter and harder? British Journal of Sports Medicine, 50(5), 273–280. [The ACWR framework described in Section 4.1 is based on Gabbett's research program; Malone et al. (2019) [Ref 1] provides sport-specific validation.]
[23] Altini, M., & Plews, D. (2021). What is behind changes in resting heart rate and heart rate variability? A large-scale analysis of longitudinal measurements acquired in free-living. Sensors, 21(23), 7932.
About the Authors
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data from athletes and leverages proprietary Cardiorespiratory Digital Twin™ technology, wearable data, and biomarker analysis to deliver personalized performance optimization and longevity recommendations to athletes, coaches, organizations, businesses, government, and the military. A 3x technology and AI company CEO with 2 successful exits—including from a $1 billion molecular diagnostics company—Tony has completed 3 Full Ironman Triathlons (140.6 miles) since 2019. He holds degrees from Harvard University, Columbia University, and earned his JD/MBA from Stanford University. He has worked with the US Olympic Team, NBA, NFL, MLB, NASA, FBI, Google, Microsoft, and the U.S. Department of Health and Human Services. His military-to-CEO journey is the subject of a forthcoming episode of 'Operation CEO,' airing on AppleTV, Prime Video, Amazon MGM Studios, and YouTubeTV in Q1 2026.
Conor Rightmire was 2025’s #1 14-year-old and All-American triathlete in the United States. He is also LongevityPlan.AI’s founding data athlete, a 2025 USATF Junior Olympic Cross Country All-American, Patriot XC League MVP, 2x New Balance National qualifier, and an exemplary student in the Class of ’29 at Marshfield High School, MA, USA.
© 2026 LongevityPlan.AI | longevityplan.ai | All Rights Reserved
#YouthAthleteDevelopment #HealthspanScience #LongevityPlanning #DigitalTwin #AIInSport #PrecisionMedicine #SportsMedicine #CardiorespiratoryScience #PediatricSportsMedicine #PerformanceOptimization #VO2Max #EpigeneticAging #REDS #AthleteMonitoring
© 2026 LongevityPlan.AI | For educational and informational purposes.
This article is for educational purposes only and is not medical advice. Always consult your doctor before changing your supplementation, medication, or training.