Sports Science
·20 min read
The Hidden Nutritional Crisis Undermining Elite Athletic Performance
Iron and Vitamin D Deficiencies in Endurance Athletes: how they relate, and how they affect the performance and health of high-performing endurance athletes
By Conor Rightmire and Tony Medrano, LongevityPlan.AI

“What you don’t measure, you can’t manage, and what you can’t manage will eventually manage you.”- A restatement of the classic Drucker principle, applied daily in the training rooms of the NFL, NASA, and the U.S. Olympic and Paralympic Committee.
You’ve invested in your training. You’ve logged the miles, dialed in your sleep, tracked your HRV, and tightened your Zone 2. But something is still wrong. Your watts are flat. Your recovery is sluggish. You’re catching every cold in the office, and your race times have quietly, almost imperceptibly, been trending in the wrong direction. You’ve been blaming stress. Or overtraining. Or your age.
What if the real culprit is sitting in a blood test you haven’t taken yet?
Welcome to one of the most underdiagnosed performance-limiting problems in competitive sport, corporate wellness, and longevity medicine: the compounding, mutually reinforcing deficiencies of iron and vitamin D, and the immunological chaos that follows in their wake.
This is not a simple “take a supplement” story. It is a precision science story. And the science has become dramatically clearer, more actionable, and more personalized in the last few years, thanks to the convergence of molecular biology, continuous monitoring technology, AI-powered biomarker platforms, and the kind of individualized physiological profiling that was once reserved for Olympic-caliber athletes and is now available to high-performing executives, master triathletes, student-athletes, and anyone serious about extending their productive years.
Part I: Why Iron Is the Engine Oil of Endurance
Iron is not simply a dietary mineral; it is the molecular pivot on which aerobic life turns.
Every gram of hemoglobin requires iron to bind oxygen in red blood cells. Every myoglobin molecule in skeletal muscle that stores and transfers oxygen during a hard interval requires iron. The electron transport chain in your mitochondria, the biological process that converts glucose and fat into ATP energy, is iron-dependent at multiple steps. So is DNA synthesis, and the regulation of energy metabolism itself. [1]
Without a sufficient supply of iron, you cannot build red blood cells efficiently. Without red blood cells, your VO₂ max, which is the gold standard predictor of both athletic performance and longevity, falls. Your muscles fatigue faster, your recovery slows, your cognitive sharpness dulls, and your immune system, already taxed by training, begins to struggle with basic surveillance.
Iron storage in the body is approximately 4 grams in men and 2.5 grams in women, with only 1–2 mg lost per day under normal conditions. The body absorbs roughly 10% of the 10–15 mg of dietary iron consumed daily. [1] Those margins sound comfortable until you have a hard training session, then the entire equation changes.
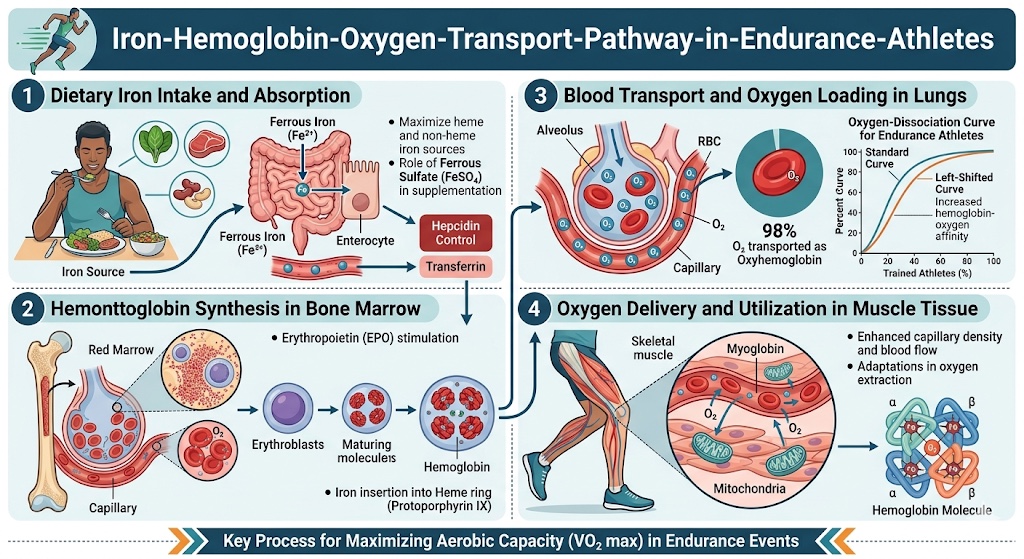
Iron is the essential cofactor in every step of the oxygen-delivery chain, which stems from hemoglobin synthesis in bone marrow, to oxygen binding in red blood cells, to mitochondrial electron transport in muscle. A deficit at any node degrades VO₂ max and athletic output before clinical anemia appears. Source: Solberg & Reikvam, Life (Basel), 2023 [PMC10608302].
The Athlete’s Iron Paradox
Endurance athletes live inside a metabolic paradox. The very act of sustained training, the thing they do to build VO₂ max and extend their healthspan, actively degrades their iron status through multiple simultaneous pathways:
- Hemolysis. Foot-strike hemolysis in runners causes the mechanical destruction of red blood cells with each impact on a hard surface. This is a real and measurable loss.
- Gastrointestinal bleeding. Hard endurance efforts reduce blood flow to the gut, which can cause microscopic GI bleeding. Not dramatic, but cumulatively significant over a training season.
- Sweat losses. Iron is excreted in sweat, and high-volume athletes sweat a great deal.
- Increased demand. Greater muscle mass, higher red blood cell turnover, and elevated mitochondrial biogenesis all increase the body’s iron requirements above those of sedentary individuals.
And then there is hepcidin, which is the master regulator of iron homeostasis, and in the context of endurance training, a silent destroyer.
Part II: Hepcidin: The Hormone Your Sports Doctor Probably Hasn’t Mentioned
Hepcidin is a 25-amino-acid peptide hormone produced primarily by the liver. Its job is elegant in design: it regulates the export of iron from intestinal cells, macrophages, and liver stores by binding to and degrading ferroportin, the body’s only known cellular iron exporter. When hepcidin is high, iron stays locked up inside cells and cannot enter the circulation. [2]
Under normal circumstances, this is a fine homeostatic mechanism. In the context of repeated endurance training, it becomes a genuine liability.
Here is why: strenuous exercise triggers the release of interleukin-6 (IL-6), a pro-inflammatory cytokine that signals the liver to produce more hepcidin. Hepcidin levels typically peak 3–6 hours after exercise, precisely when most athletes eat their largest iron-containing meal of the day. [2]
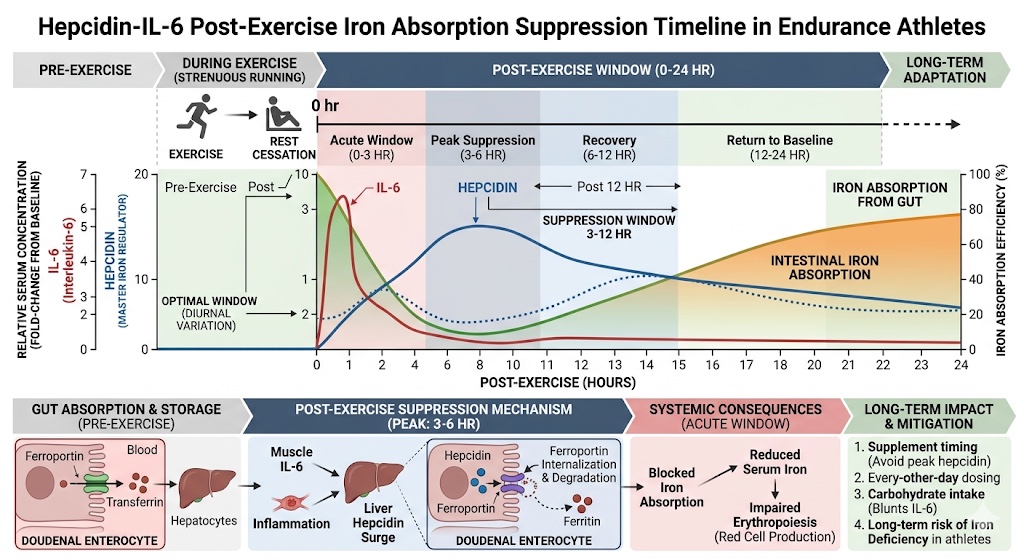
Post-exercise hepcidin kinetics: plasma hepcidin increases 51% within hours of a prolonged run (Barney et al., Journal of Nutrition, 2022), driven by IL-6, and reduces fractional iron absorption by 36% compared to rest. The peak hepcidin window (3–6 hours post-exercise) coincides with athletes’ primary meal times, which is a critical scheduling conflict.
A landmark 2022 study published in The Journal of Nutrition, examining 28 trained collegiate cross-country runners, found that:[3]
- Plasma hepcidin increased by 51% after a prolonged run (45.8 vs. 30.3 ng/mL at rest)
- Fractional iron absorption was reduced by 36% compared with rest (11.8% vs. 18.5%)
- Plasma IL-6 was significantly elevated post-exercise, consistent with the hepcidin elevation.
This means that an endurance athlete who finishes a long run and then eats a steak and spinach for dinner, doing everything “right” by conventional nutrition wisdom, may be absorbing barely two-thirds of the iron they think they’re getting.
Professor Peter Peeling of the University of Western Australia, one of the foremost researchers on iron metabolism in athletes, has noted that understanding the timeline of hepcidin elevation should fundamentally change how practitioners advise athletes on the timing of iron consumption by suggesting early morning intake, on an empty stomach, at least one hour before training, as the optimal window when hepcidin is at its lowest.[3]
An elevated hepcidin response has also been observed during intensified training periods in well-trained female long-distance runners, even when daily dietary iron intake appeared adequate, suggesting that training volume alone can drive iron deficiency through this hormonal pathway.[4]
Part III: The Scope of the Problem: Who Is Actually Deficient?
A detailed 2023 review published in Life (Basel) by Andrea Solberg and Håkon Reikvam of the University of Bergen confirmed that iron deficiency is prevalent among endurance athletes, not as a clinical outlier, but as a common finding, and its impact on VO₂ max and physical performance is well-documented. The review found that iron supplementation produced its most meaningful performance improvements in those with the lowest baseline iron status.[1]
Dr. Stacy Sims, PhD, one of the world’s leading researchers on female physiology and exercise nutrition, and author of ROAR, has quantified the disparity clearly: while iron deficiency affects roughly 5 to 11% of male athletes, that figure jumps to 15 to 35% of female athletes, driven by menstrual losses, training demands, and diagnostic thresholds that may be set too low.[5] A study in The Lancet Haematology has flagged this diagnostic gap, suggesting that the standard serum ferritin cut-off (typically 12–15 ng/mL) misses a large proportion of women experiencing iron deficiency without frank anemia (IDNA), a state where hemoglobin remains technically “normal” but iron stores are depleted enough to impair performance, mood, and recovery.
“Vitamin D is super important for downregulating hepcidin. We tell women to take vitamin D around training. That helps with that inflammatory response and reduces hepcidin. That’s another key link for people trying to increase their intake and absorption of iron.” - Dr. Stacy Sims, PhD, Female Physiology Expert
The Biomarker Hierarchy for Iron Assessment
Standard care measures hemoglobin. Performance science goes deeper:
- Serum ferritin, the primary storage biomarker, values below 30–50 ng/mL warrant attention in athletes
- Soluble transferrin receptor (sTfR), a more sensitive indicator of functional iron depletion at the tissue level, rises when cells are starving for iron
- sTfR-to-ferritin ratio (sTfR-F index), considered the gold standard for differentiating true iron deficiency from anemia of chronic inflammation
- Transferrin saturation, the percentage of transferrin that is iron-bound; low values confirm restricted iron supply
- Hepcidin, emerging as a clinically useful direct measure of iron regulatory status[4]
If your physician is only measuring hemoglobin during your annual physical, they are looking at the last domino to fall, not the ones already toppling.
Part IV: Vitamin D: Not Just for Bones Anymore
Vitamin D receptor (VDR) sites have now been identified in virtually every cell type in the human body, including immune cells (macrophages, dendritic cells, T cells, and B cells), skeletal muscle fibers, cardiac muscle, and brain tissue. Vitamin D, when converted to its active form calcitriol, functions not merely as a vitamin but as a steroid hormone, directly regulating the expression of an estimated 1,000 to 2,000 genes involved in immune defense, protein synthesis, muscle function, cardiovascular performance, inflammatory response, and cell growth.[6]
The Immune Cost of Deficiency
Clara Crescioli, PhD, of the University of Rome “Foro Italico”, published a comprehensive 2022 narrative review in Frontiers in Immunology documenting how vitamin D acts as a critical regulator of both innate and adaptive immune responses, precisely the immune systems that athletes stress most severely through hard training.[7]
Prolonged, intense endurance exercise suppresses key components of immune function, including:
- Reduced output of secretory immunoglobulin A (SIgA) in saliva, which is the first line of defense against upper respiratory infections
- Reduced function of natural killer (NK) cells, neutrophils, T cells, and B cells
- Downregulation of MHC-II expression in macrophages, impairing pathogen presentation to T lymphocytes
A pivotal study of 225 endurance athletes over a 16-week winter training period found that those with vitamin D-deficient status (25(OH)D < 30 nmol/L) suffered a significantly higher incidence of upper respiratory tract infections than those with optimal levels (> 120 nmol/L). The optimal-status group showed significantly higher salivary SIgA secretion rates and higher cathelicidin concentrations (an antimicrobial peptide critical to innate defense).[8]
“Vitamin D3 is a steroid hormone involved in the expression of 1,000+ genes in your body. It plays a role in regulating serotonin, immune function, heart health, and weight management, and yet most athletes have no idea what their levels actually are.”
Dr. Rhonda Patrick, PhD, FoundMyFitness. Target blood level recommendation: 40–60 ng/mL of 25(OH)D.[9]
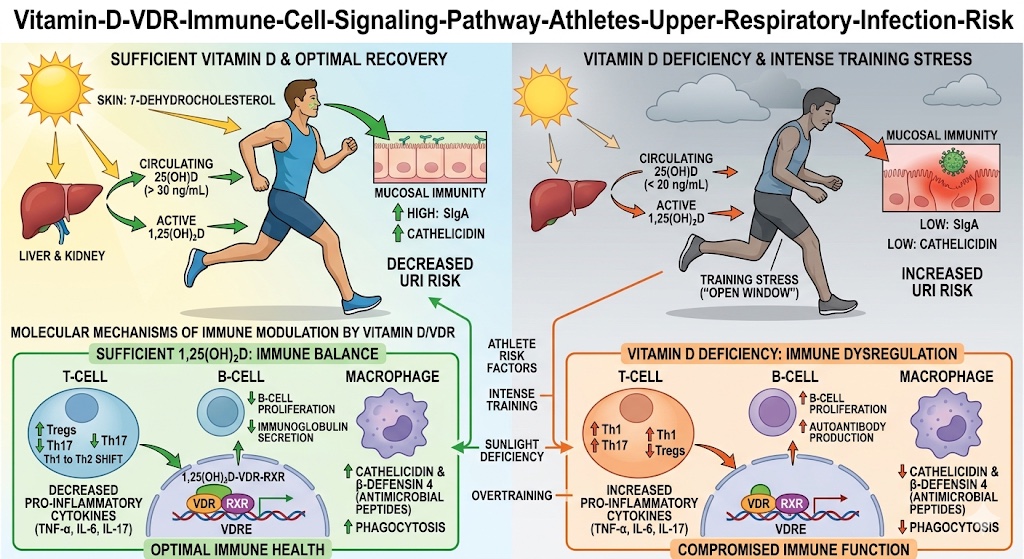
Vitamin D (calcitriol) binds to vitamin D receptors (VDR) on immune cells, including macrophages, T-cells, B-cells, and natural killer cells, activating antimicrobial peptide production (cathelicidins, defensins) and modulating cytokine cascades. In athletes with 25(OH)D < 30 nmol/L, this pathway is suppressed. Source: Crescioli, Frontiers in Immunology, 2022 [PMC9539769]; He et al., Exercise Immunology Review, 2016 [PMID 26634839].
Vitamin D, Muscle, and Physical Performance
Vitamin D directly modulates skeletal muscle biology through both genomic and non-genomic pathways. The genomic pathway involves calcitriol binding to nuclear VDRs in muscle cells, triggering protein synthesis and an increased number of type II (fast-twitch) muscle fibers, which are the fibers most responsible for power output, sprint speed, and force production.[10]
Vitamin D deficiency has been shown to cause:
- Fatty degeneration of type II muscle fibers
- Reduced muscle contraction velocity and strength
- Increased injury risk, including stress fractures
- Slower post-exercise recovery and muscle regeneration
A 2017 systematic review in the Journal of Strength and Conditioning Research found that vitamin D supplementation significantly improved muscle strength across multiple studies, most pronounced in those starting from a deficient baseline. Research has also revealed VDR sites on cardiac muscle tissue, raising compelling questions about vitamin D’s role in cardiovascular performance and long-term heart health.[11]
Part V: The Iron-Vitamin D Axis and Its Immune Consequences
Iron and vitamin D are not independent variables. They influence each other through multiple intersecting pathways, creating a bidirectional relationship that standard clinical panels, assessed in isolation, systematically miss with direct consequences for immune function, erythropoiesis, and recovery.
The Two-Way Street
A landmark study published in Nutrients examining 219 female elite athletes across seven sports disciplines found:[12]
- The percentage of iron-deficient athletes was significantly higher (32%) in the vitamin D-deficient group than in the vitamin D-sufficient group (11%)
- The odds ratio for vitamin D deficiency increased with progressing iron deficiency, from 1.75 in mild iron deficiency to 4.6 in severe iron deficiency.
- The percentage of vitamin D-deficient athletes was higher (75%) among those with iron deficiency than in those with normal iron status (48%)
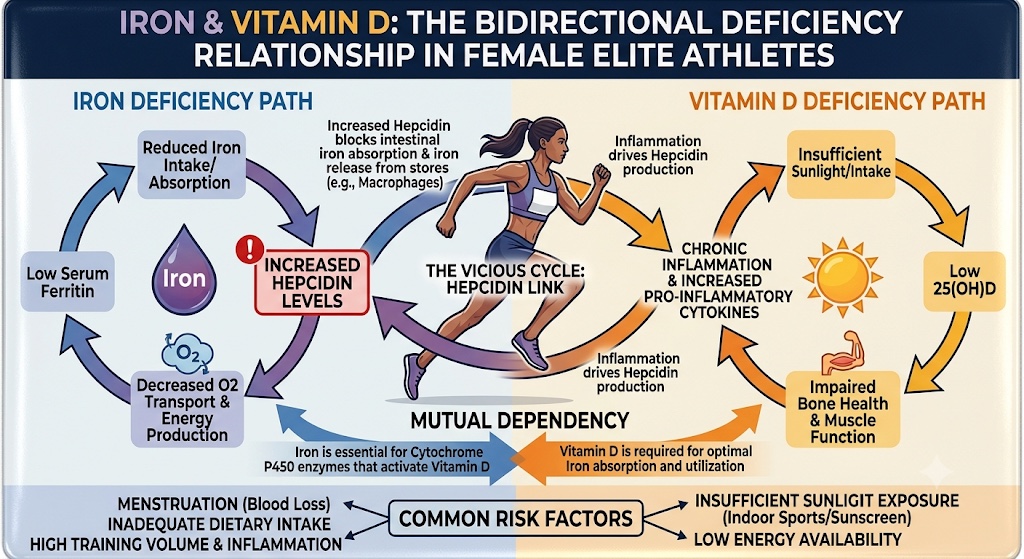
The bidirectional iron–vitamin D relationship in 219 elite female athletes: iron deficiency was 3x more prevalent in vitamin D-deficient athletes (32% vs. 11%), and the odds ratio for vitamin D deficiency rose to 4.6 in severely iron-deficient athletes. Source: Malczewska-Lenczowska et al., Nutrients, 2018 [PMC5852743].
The mechanisms driving this mutual dependency include:
- Iron is required for vitamin D synthesis. The hydroxylation of vitamin D is mediated by iron-dependent cytochrome P450 enzymes. Without adequate iron, your body cannot efficiently convert D precursors into their active hormonal form.
- Vitamin D modulates hepcidin. Vitamin D plays a role in downregulating hepcidin, thereby improving the body’s ability to absorb dietary iron. One reason Dr. Sims advises female athletes to take vitamin D timed around training.[5]
- Both modulate erythropoiesis. Vitamin D receptors have been found on erythroid progenitor cells, suggesting that vitamin D directly influences red blood cell production.[1]
- Both regulate inflammation. Both deficiencies amplify inflammatory cytokine cascades (especially IL-6 and TNF-α) and are suppressed by chronic inflammation, which creates a feedback loop in which nutritional depletion drives inflammatory load, which drives further depletion.
How it affects the Immune system:
Both iron and vitamin D function as regulatory inputs to the immune system, not merely nutritional raw materials. Understanding their immune roles completes the clinical picture and explains why deficiencies in both compounds together create compounding vulnerability.
Iron and immune function: Iron is essential for the proliferation of lymphocytes and the oxidative burst of neutrophils, which are the key components of pathogen defense. However, iron is also used by pathogens for growth, which is why the body restricts iron availability during infection. This creates a genuine clinical tension in athletes: iron supplementation during acute illness may be counterproductive, as it feeds pathogens. Chronic iron deficiency, however, creates immunosuppression that makes infections more likely in the first place. Timing and precision matter enormously.
Vitamin D and immune calibration: Vitamin D helps the immune system calibrate its response by promoting antimicrobial peptide production and T-regulatory cell function while dampening excessive inflammatory responses. A 2024 systematic review in the journal Sports confirmed that vitamin D supplementation was associated with reductions in pro-inflammatory markers (IL-6, TNF-α) in exercising athletes, with the strongest effects in those who were deficient at baseline.[13]
A 2026 narrative review in Nutrients by researchers at Radom University in Poland who analyzed a decade of evidence across vitamins A, C, D, E, and B-complex, reinforced that vitamin D deficiency is the most prevalent micronutrient problem in athletes, particularly in indoor sports and winter months, and crucially noted that excessive antioxidant supplementation can paradoxically impair adaptive responses like mitochondrial biogenesis, which is a nuance that underscores the need for precision, not blanket supplementation.[14]
The clinical upshot: if you find iron deficiency, look for vitamin D deficiency. If you find a vitamin D deficiency, check iron more carefully than a single hemoglobin value. These two deficiencies travel together.
Part VI: Who Is Most at Risk and Why It’s Probably Not Who You Think
The actual at-risk populations are broader and more surprising than the popular image of the elite marathon runner:
- Female endurance athletes of all levels. The combination of menstrual losses, typically lower caloric intake, and high training volume creates persistent iron deficits. Research consistently shows a 15–35% prevalence in this group.[5]
- Male distance runners and triathletes. Foot-strike hemolysis, GI bleeding during long events, and high sweat losses place male endurance athletes at meaningful risk. Studies suggest a 5–11% prevalence, but functional deficiency (without frank anemia) is more common.[1]
- Plant-based and vegetarian athletes. Non-heme iron (from plant sources) is absorbed at roughly 1–8% compared to 15–35% for heme iron from animal sources. Plant-based athletes must consume significantly more dietary iron to achieve equivalent absorption.
- Indoor athletes and winter-season athletes. Vitamin D synthesis requires UVB sun exposure, which drops precipitously in northern latitudes during winter. NBA players, indoor swimmers, gymnasts, and wrestlers have particularly high rates of vitamin D deficiency.
- Master athletes and executives over 40. Skin synthesis of vitamin D declines significantly with age. Absorption of dietary iron may also decline with age-related changes in gastric acid secretion.
- Elite student-athletes. Young women in demanding sports like cross-country, soccer, and rowing face triple jeopardy: These include growth demands, menstrual losses, and training loads, which all happen during the years when bone density and iron stores need to be maximized for long-term health.
Part VII: From Deficiency to Optimization: What Actually Works
Testing First, Always
There is no substitute for objective measurement. A targeted panel for iron and vitamin D status in athletes should include:
For iron: Serum ferritin, hemoglobin, hematocrit, transferrin saturation, total iron binding capacity (TIBC), and soluble transferrin receptor (sTfR). Consider hepcidin where available.
For vitamin D: Serum 25-hydroxyvitamin D (25(OH)D). Many practitioners now consider 40–60 ng/mL optimal for athletes, rather than the clinical sufficiency cutoff of 20–30 ng/mL.
For immune status: High-sensitivity CRP (hsCRP), white blood cell differential, and saliva SIgA can help characterize the immunological picture.
Table 1. Performance-Optimized Biomarker Reference Ranges for Endurance Athletes
| Biomarker | Clinical “Normal” | Performance-Optimized Target |
|---|---|---|
| Serum Ferritin | > 12 ng/mL (women), > 15 ng/mL (men) | > 50 ng/mL (both sexes) |
| Hemoglobin | > 12 g/dL (women), > 13.5 g/dL (men) | High-normal for sex/altitude |
| Transferrin Saturation | 15–50% | 25–40% |
| 25(OH)D (Vitamin D) | > 20 ng/mL | 40–60 ng/mL |
| hsCRP (Inflammation) | < 3.0 mg/L | < 1.0 mg/L |
| sTfR | 8.7–28.1 nmol/L | Low-normal (tissue iron replete) |
Note: All testing and supplementation should be supervised by a qualified sports medicine physician, internist, or registered dietitian specializing in athlete health. Do not supplement with iron without a documented deficiency.
Iron Supplementation: Timing Is Everything
The research is clear: iron supplementation is most effective when taken on an empty stomach, at least 60 minutes before food or at least 2 hours after a meal, and not in the post-exercise hepcidin window (3–6 hours post-training). See Part II for the underlying mechanism.[3]
Forms matter. Ferrous sulfate is the most commonly prescribed form, but ferrous bisglycinate chelate shows comparable absorption with substantially fewer GI side effects. Intravenous iron therapy is increasingly used in elite settings when oral iron proves insufficient. Vitamin C co-ingestion enhances non-heme iron absorption by up to 2–3x by converting iron to the ferrous (Fe²⁺) form that intestinal transporters (DMT1) can absorb. Coffee, tea, calcium, and phytates should be separated from iron intake by 1–2 hours.
Vitamin D Supplementation: D3, Not D2
The relevant form for supplementation is cholecalciferol (D3), not ergocalciferol (D2). D3 is substantially more bioavailable and biologically active than D2. Dosing should be individualized based on baseline 25(OH)D levels. Many sports medicine physicians use 4,000–6,000 IU/day in documented deficiency, with monitoring every 3 months. Dr. Rhonda Patrick has described maintaining her own levels at 4,000–5,000 IU/day, targeting blood levels of 50 ng/mL.[9]
Vitamin K2 (specifically MK-7) is the critical co-nutrient for vitamin D supplementation at higher doses, as it directs calcium to bones rather than soft tissues and arteries. Magnesium is also required for vitamin D activation; magnesium deficiency (extremely common in athletes) can blunt the full biological impact of vitamin D supplementation.
Nutrition: The Foundation That Supplements Cannot Replace
For iron: Prioritize heme iron (red meat, dark poultry, seafood, especially oysters and clams) as the most bioavailable source. Athletes in heavy training blocks may need 18–32 mg of dietary iron per day, substantially above the standard RDA.
For vitamin D: Fatty fish (salmon, sardines, mackerel), egg yolks, and fortified dairy are the primary dietary sources, but dietary supply is rarely sufficient to reach optimal blood levels without supplementation, particularly for those with limited sun exposure.
Part VIII: The Cardiorespiratory Digital Twin™: AI-Powered Iron and Vitamin D Monitoring at Scale
The challenge with iron and vitamin D management is not conceptual. It is personalized and dynamic. Your iron absorption efficiency is shaped by your hepcidin genotype. Your vitamin D conversion rate is influenced by polymorphisms in the CYP2R1 and CYP27B1 genes. Your training load, diet composition, latitude, season, inflammatory status, and gut microbiome all interact to determine your real-time micronutrient status in ways that defy simple algorithms.
This is precisely why AI-powered longitudinal biomarker tracking has become one of the most important tools in elite performance medicine. At the center of this revolution is the Cardiorespiratory Digital Twin™, developed by LongevityPlan.AI to continuously model, track, and optimize an individual athlete’s iron, vitamin D, and immune status in real time.
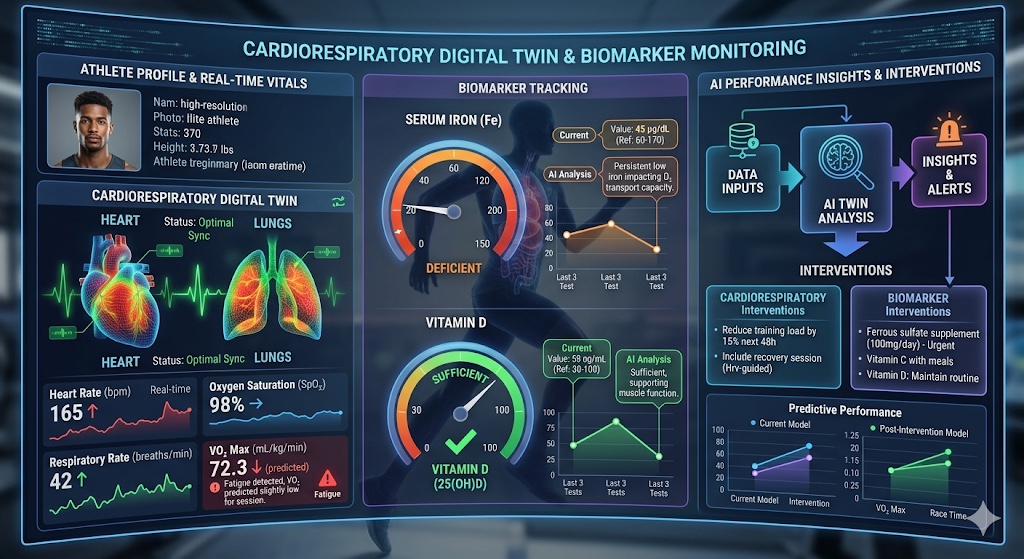
The LongevityPlan.AI Cardiorespiratory Digital Twin™ integrates continuous wearable data (HRV, sleep, load), periodic biomarker panels (ferritin, 25(OH)D, hsCRP, sTfR), and training-load metrics into a single AI model. Outputs include personalized iron absorption windows, vitamin D dosing protocols, immune readiness scores, and longitudinal nutrient trajectory forecasts.
How the Digital Twin Measures Iron and Vitamin D:
The Cardiorespiratory Digital Twin™ does not merely display raw biomarker numbers. It builds a living, continuously updated physiological model of your body by fusing four distinct data streams:
- Continuous wearable signals. Heart rate variability (HRV), resting heart rate, sleep architecture, and training load from devices like WHOOP, ŌURA Ring, and Garmin provide surrogate markers of iron and vitamin D status that update daily. A declining HRV trend combined with rising resting heart rate and plateauing training adaptation, for example, can serve as an early composite signal of emerging iron deficiency, which is weeks before clinical anemia appears on a blood panel.
- Periodic biomarker panels. The Digital Twin ingests structured laboratory data from providers, including InsideTracker and Function Health, by capturing ferritin, hemoglobin, sTfR, transferrin saturation, TIBC, 25(OH)D, hsCRP, and vitamin B12. Each lab draw is timestamped against training load and nutrition data, allowing the model to contextualize results: a ferritin of 28 ng/mL two days after a race is a very different clinical picture than the same result after two weeks of rest.
- Training and lifestyle context. Training log data, which includes volume, intensity, sport modality, altitude, and environmental heat, is fed into the model to calculate the expected hepcidin response on any given day. The Digital Twin uses this to forecast when iron absorption will be most suppressed and when it will be most available, generating a personalized iron absorption window calendar for each athlete.
- Genetic and epigenetic inputs. Integration with epigenetic age platforms such as True Diagnostics DunedinPACE algorithm and nutrigenomic data (CYP2R1/CYP27B1 vitamin D metabolism polymorphisms, TMPRSS6 iron absorption variants) allows the Digital Twin to personalize dosing recommendations beyond population averages.
What the Digital Twin Recommends:
Based on the integrated model, the Cardiorespiratory Digital Twin™ generates seven categories of personalized, real-time recommendations related to iron and vitamin D:
- Optimal iron supplementation timing - specific windows based on predicted hepcidin nadir (e.g., “tomorrow morning, 6:00–7:00 AM, before training, empty stomach”)
- Iron-enhancing dietary co-pairings - vitamin C with iron-rich meals; separation of calcium, coffee, and phytates
- Personalized vitamin D3 dosing - weekly targets calibrated to current 25(OH)D levels, body mass, sun exposure history, and seasonal latitude
- Vitamin D + K2 + magnesium co-supplementation protocols - because vitamin D cannot be optimized in isolation
- Immune readiness scores - a daily composite index (0–100) integrating iron status, vitamin D status, sleep quality, and training load to flag days when infection risk is highest
- Retest scheduling - AI-driven prompts to retest specific biomarkers at the optimal interval
- Longitudinal trajectory forecasting - predictive modeling showing how current iron and vitamin D trends will evolve over the next 90 days under different supplementation and training scenarios
Tools That Feed the Twin: Real-World Platforms:
InsideTracker, whose Scientific Advisory Board is chaired by Dr. David Sinclair of Harvard Medical School, operates one of the largest longitudinal biomarker databases in consumer health. A 2024 retrospective analysis of more than 20,000 users over approximately five years found statistically significant improvements (p < 0.05) in 43 different biomarkers, including vitamin D, iron, hsCRP, HbA1c, and LDL cholesterol, among users who followed AI-generated personalized action plans.[15] Users who actively engaged with individualized recommendations showed meaningfully better outcomes than those who received data without guidance.
On the continuous monitoring side, Abbott’s FreeStyle Libre and Dexcom’s Stelo, which were both cleared over-the-counter in the US in 2024, add a critical metabolic dimension to the Digital Twin’s iron optimization model. Research has established that low carbohydrate availability amplifies the post-exercise hepcidin spike, meaning a depleted glycogen state after training directly worsens iron absorption.[16] CGM integration allows the Digital Twin to correlate glycemic patterns with hepcidin-predicted iron absorption windows, generating nutrition timing recommendations that simultaneously optimize carbohydrate availability and iron uptake.
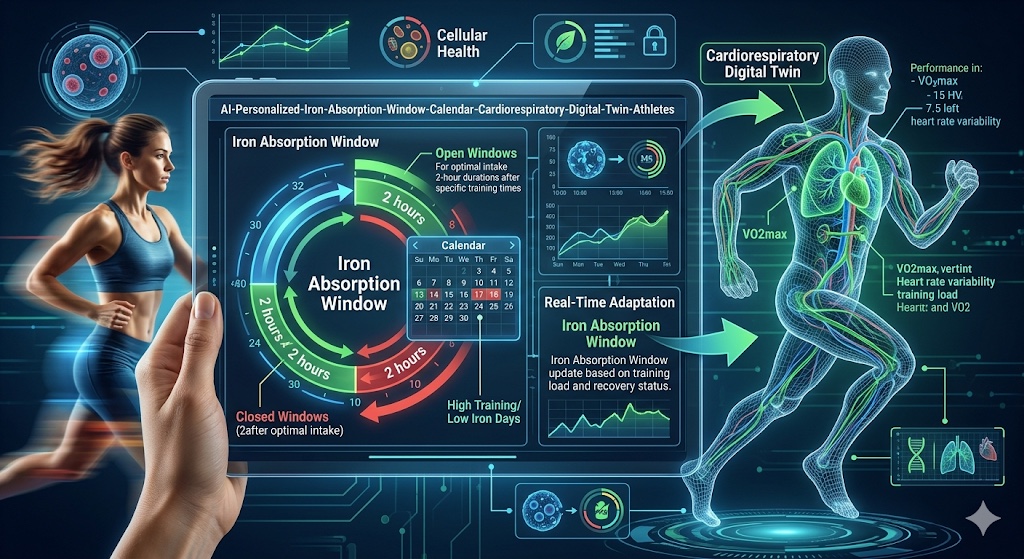
The Cardiorespiratory Digital Twin™ generates a personalized iron absorption window calendar by modeling predicted hepcidin levels based on training load, CGM glycemic data, sleep quality, and prior biomarker trends. Green windows indicate optimal iron absorption timing; red windows indicate high hepcidin suppression periods to avoid.
Part IX: Lessons from Elite Organizations: What the Best Are Already Doing
U.S. Olympic and Paralympic Committee (USOPC)
The USOPC Sports Dietitian program conducts routine iron and vitamin D screening across Olympic sports, with particular emphasis on endurance athletes, female athletes, and those in indoor training environments. Iron management protocols, including IV iron infusions for documented severe depletion, are part of standard performance support at major championships. Altitude training camps include mandatory iron optimization protocols, often with monitoring every 3–4 weeks.
NFL Teams
Multiple NFL franchises have integrated wearable biometric monitoring, blood biomarker testing, and AI-assisted load management into their performance systems. A player whose ferritin drops below threshold during training camp is now frequently identified proactively, because the data systems connect performance metrics to biological markers in ways that create early warning signals.
Cleveland Clinic and Johns Hopkins Medicine
Both the Cleveland Clinic and Johns Hopkins Medicine have integrated precision nutrition, including systematic iron and vitamin D assessment, into their sports medicine and executive health programs. The Cleveland Clinic Executive Health Program includes advanced biomarker screening panels as standard components of annual evaluations for corporate leaders who demand the same physiological optimization protocols as elite athletes.
Viome and the Gut Microbiome Frontier
Viome, founded by Naveen Jain, has brought metatranscriptomics-based gut microbiome analysis to consumer health. Their emerging research platform is beginning to illuminate the relationship between microbiome composition and iron absorption efficiency. Specific gut bacteria are involved in the fermentation and transformation of dietary iron, and dysbiosis may contribute to iron deficiency even in the presence of adequate dietary intake.
Elite sports organizations like NFL training camps and Olympic altitude training centers have adopted systematic iron and vitamin D screening as performance infrastructure. The Cardiorespiratory Digital Twin™ democratizes this level of precision for independent athletes, coaches, and executives.
Part X: A Practical Monitoring Protocol for Performance-Focused Individuals
Whether you are a 52-year-old Ironman competitor, a 38-year-old CEO who runs marathons, a high-school soccer player with Division I aspirations, or a military officer responsible for peak cognitive and physical performance under pressure, the framework is the same, with individualized parameters.
Quarterly Blood Panels (minimum, twice annual)
Should include: ferritin, hemoglobin, hematocrit, sTfR, transferrin saturation, TIBC, 25(OH)D, hsCRP, complete blood count with differential, and vitamin B12. Add hepcidin during heavy training blocks if clinically available. Platforms such as InsideTracker, Function Health, and Fountain Life offer comprehensive panels that go beyond standard clinical care.
Continuous Monitoring
CGM (Abbott Lingo or Dexcom Stelo for non-diabetic use cases) provides real-time data on carbohydrate status and post-exercise metabolic recovery, including the glycemic patterns that influence hepcidin and iron absorption.
Wearable Integration
HRV tracking via Garmin, Polar, WHOOP, or ŌURA Ring provides surrogate markers of recovery quality and autonomic nervous system function that correlate with micronutrient status over time.
AI-Powered Analysis
Integration of longitudinal data like biomarkers, wearable data, and training load is the layer that transforms raw numbers into actionable, personalized interventions. This is the core premise of LongevityPlan.AI’s Cardiorespiratory Digital Twin™: not population-average recommendations, but individual-specific protocols calibrated to your biology, your training demands, your hormonal status, and your longevity goals.
A quarterly precision biomarker protocol for performance-focused athletes and executives: ferritin, sTfR, transferrin saturation, TIBC, 25(OH)D, hsCRP, and CBC with differential from the evidence-based minimum. Integrated with the Cardiorespiratory Digital Twin™, this protocol creates an early warning system that catches iron and vitamin D depletion weeks before symptoms appear.
Conclusion: The Performance Gap You Can Close
Iron deficiency and vitamin D insufficiency are not exotic conditions for sick people. They are among the most prevalent, most performance-limiting, and most correctable nutritional deficiencies in active, ambitious, health-conscious humans.
The science is unambiguous: both deficiencies independently reduce VO₂ max, impair immune resilience, slow recovery, reduce muscle strength, and compromise cognitive function. Together, through their bidirectional molecular interactions, they amplify each other’s harms by creating a compounding deficit that standard clinical panels often fail to catch before it costs weeks of performance, months of injury recovery, or years of healthspan.
The tools to address these gaps are through precision biomarker testing, AI-powered personalized protocols including the Cardiorespiratory Digital Twin™, continuous monitoring technology, and evidence-based supplementation strategies timed to the biology of training have never been more accessible or more powerful.
The only thing required is the decision to measure, to understand, and to act with the precision that your biology deserves. Because the gap between excellent and extraordinary is often not more training, it’s better data and the wisdom to act on it.
Your longevity plan starts today.
About the Authors:
Conor Rightmire was 2025’s #1 14-year-old and All-American triathlete in the United States. He is also LongevityPlan.AI’s founding data athlete, a 2025 USATF Junior Olympic Cross Country All-American, Patriot XC League MVP, 2x New Balance National qualifier, and an exemplary student in the Class of ’29 at Marshfield High School, MA, USA.
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data from athletes and leverages proprietary Cardiorespiratory Digital Twin™ technology, wearable data, and biomarker data to deliver personalized performance optimization and longevity recommendations to athletes, coaches, organizations, businesses, government, and the military. In addition to being a 3x technology / AI company CEO with 2 successful exits, Tony has also finished 3 Full Ironman Triathlons (140.6 mi) since 2019. He has degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University. Tony has been involved with AI and molecular diagnostic start-ups for 10 years, and also worked with the U.S. Olympic Team, National Basketball Association (NBA), National Football League (NFL), Major League Baseball (MLB), Iditarod, FBI, NASA, U.S. Department of Health and Human Services (HHS), Google, Microsoft, Netflix, Bridgewater Associates, ConocoPhillips, British Petroleum, One Medical, and Jenny Craig, Inc. to provide technology, artificial intelligence and/or molecular diagnostics solutions to their employees. Tony also served as a U.S. Navy Officer commanding an emergency response team on a USN Destroyer. LongevityPlan.AI is veteran-owned.
Footnotes and Primary Sources
[1] Solberg, A. & Reikvam, H. “Iron Status and Physical Performance in Athletes.” Life (Basel), 13(10):2007. October 2023. PMC10608302. DOI: 10.3390/life13102007
[2] Peeling, P. et al. “Iron Status and the Acute Post-Exercise Hepcidin Response in Athletes.” PLoS ONE, 2014. PMC3965532.
[3] Barney, D.E. et al. “A Prolonged Bout of Running Increases Hepcidin and Decreases Dietary Iron Absorption in Trained Female and Male Runners.” Journal of Nutrition, September 2022. DOI: 10.1093/jn/nxac158.
[4] Deguchi, M. et al. “Elevated Serum Hepcidin Levels during an Intensified Training Period in Well-Trained Female Long-Distance Runners.” Nutrients, 2017. PMC5372940.
[5] Sims, S. “Women and Iron Deficiency.” drstacysims.com; Tonal Research Communications, 2022–2023.
[6] Ogan, D. & Pritchett, K. “Vitamin D and the Athlete: Risks, Recommendations, and Benefits.” Nutrients, 5(6):1856–1868. 2013. PMC3725481.
[7] Crescioli, C. “Vitamin D, Exercise, and Immune Health in Athletes: A Narrative Review.” Frontiers in Immunology, 13:954994. September 2022. PMC9539769.
[8] He, C.S. et al. “Influence of Vitamin D Status on Respiratory Infection Incidence and Immune Function during 4 Months of Winter Training in Endurance Sport Athletes.” Exercise Immunology Review, 2016. PubMed PMID: 26634839.
[9] Patrick, R. “Vitamin D3’s Role in Immune Function.” FoundMyFitness.com. Personal communications and published educational content.
[10] Książek, A. et al. “Vitamin D, Skeletal Muscle Function and Athletic Performance in Athletes — A Narrative Review.” Nutrients, 11(8):1800. 2019. PMC6722905.
[11] Close, G.L. et al. “Assessment of Vitamin D Concentration in Non-Supplemented Professional Athletes and Healthy Adults during the Winter Months in the UK.” Journal of Sports Sciences, 31(4):344–353. 2013.
[12] Malczewska-Lenczowska, J. et al. “The Association between Iron and Vitamin D Status in Female Elite Athletes.” Nutrients, 2018. PMC5852743.
[13] Saedmocheshi, S. et al. “The Effect of Vitamin D Consumption on Pro-Inflammatory Cytokines in Athletes: A Systematic Review of RCTs.” Sports, 12(1):32. January 2024. PMC10821273.
[14] Wiacek, M. et al. “Vitamin Supplementation in Sports: A Decade of Evidence-Based Insights.” Nutrients, 18(2):213. January 2026. PMC12845069.
[15] InsideTracker / Segterra. “Landmark Study of 20,000 Users: AI Health Platform Linked to Significant, Sustained Health Biomarker Improvements.” Business Wire / Fitt Insider. 2024–2026.
[16] Badenhorst, C.E. et al. “Effects of Macro- and Micronutrients on Exercise-Induced Hepcidin Response in Highly Trained Endurance Athletes.” International Journal of Sport Nutrition and Exercise Metabolism, 2017. PubMed PMID: 28605609.
This article is for educational purposes only and is not medical advice. Always consult your doctor before changing your supplementation, medication, or training.