Longevity
·14 min read
The Fire and the Firefighters: How to Actually Lower Inflammation
Not all inflammation is the same, and most of what you've been sold to fight it is noise. A skeptic's evidence-graded guide to the real causes and types of inflammation, and how diet, supplements, peptides, and measurement-first longevity planning actually move the needle.
By Tony Medrano, LongevityPlan.AI
In 2017, a cardiologist named Paul Ridker ended a twenty-five-year argument with a single trial. He took more than ten thousand heart-attack survivors whose cholesterol was already controlled by statins, gave half of them a drug that did nothing to their LDL and everything to one inflammatory signal — interleukin-1β — and watched their rate of second heart attacks, strokes, and cardiovascular deaths fall by roughly fifteen percent.[7] The drug, canakinumab, had no business helping the heart by the old logic. It helped anyway. Ridker's framing of why is the most important sentence in modern preventive cardiology, and it is short enough to memorize.
"Half of heart attacks occur in people who do not have high cholesterol."
— Paul M. Ridker, MD, Brigham and Women's Hospital, on the CANTOS trial[7]
That is the premise of this article, and of this newsletter. Inflammation is not a wellness buzzword to be smothered with turmeric lattes. It is a measurable, mechanistic driver of the diseases that actually end careers and lives — heart disease, diabetes, dementia, many cancers, and the slow erosion we politely call "aging." The science is now precise enough that you can quantify your own inflammatory load, identify the type of inflammation you have, and intervene using tools ranging from a grocery list to a monoclonal antibody. The catch is that the precision is wasted on people who don't measure. This is a buyer's guide for those who would rather measure.
Our audience skews skeptical — the forty-something executive who has been burned by supplement hype, the master's athlete nursing an old injury, the parent rebuilding after a hard decade, the seventy-year-old who wants the next decade to be worth living. Good. Skepticism is the correct posture. The argument here is not that you should believe more; it is that you should measure more, and let the data decide what belongs in your plan.
01 / The Two Fires
Acute inflammation saves your life. Chronic inflammation quietly ends it.
Why is the same biology that heals a sprained ankle the leading suspect behind age-related disease?
Inflammation is, at its root, a repair crew. When you cut yourself or catch a virus, the immune system mounts a fast, intense, local, self-limiting response: blood vessels dilate, neutrophils swarm, cytokines shout, the threat is cleared, and — this is the part everyone forgets — the whole operation is supposed to shut itself off.[1] Acute inflammation is not the enemy. An athlete who couldn't inflame couldn't heal. A body that couldn't inflame couldn't survive a splinter.
The trouble begins when the fire never goes out. Systemic chronic inflammation — a low-grade, smoldering, body-wide activation that produces no fever, no swelling, no symptom you can feel — is a different animal entirely. It does not protect tissue; it degrades it. And because it is silent, it accumulates for decades before it announces itself as a diagnosis. The Italian immunologist Claudio Franceschi gave this phenomenon its name around the turn of the millennium: inflammaging, the chronic low-grade inflammation that rises with age and tracks with nearly every disease of aging.[4]
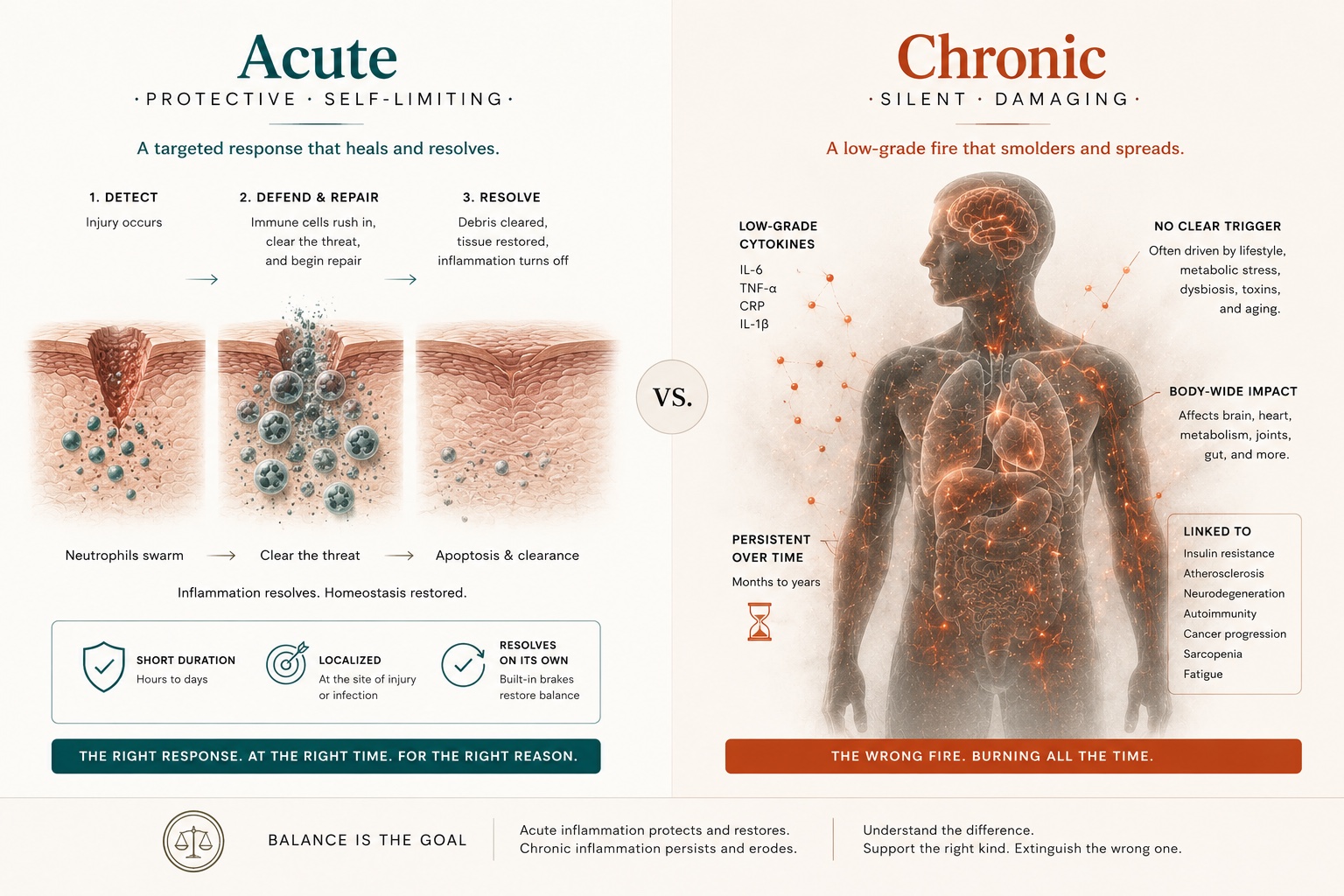
Figure 1. Acute vs. Chronic Systemic Inflammation: How Self-Limiting Repair Becomes Inflammaging
Acute inflammation is a fast, local, self-terminating repair response; chronic systemic inflammation is a silent, body-wide smolder that drives age-related disease — the phenomenon Claudio Franceschi named "inflammaging."
David Furman, who directs the Artificial Intelligence platform at the Buck Institute for Research on Aging and the 1,000 Immunomes Project at Stanford, has spent his career arguing that this is not a side effect of aging but a central cause of it. In 2013, researchers catalogued nine "hallmarks" of aging — genomic instability, telomere attrition, mitochondrial dysfunction, and the rest. Furman's contention is that chronic inflammation sits upstream of almost all of them.[3]
"I think of inflammation as the 10th hallmark."
— David Furman, PhD, Buck Institute for Research on Aging & Stanford University[3]
His point is mechanistic, not poetic: if you are chronically inflamed, he argues, you will also tend to have genomic instability, mitochondrial dysfunction, protein-folding problems, telomere shortening, and epigenetic drift — the supposedly independent hallmarks, all downstream of one smoldering signal.[3] That reframing matters for the skeptic, because it converts "inflammation" from a vague villain into a single, trackable, modifiable lever.
02 / A Taxonomy of Smoke
Where the fire actually starts
Chronic inflammation is not one condition. It has at least five distinct origins, and they call for different responses.
The reason most "anti-inflammatory" advice fails is that it treats inflammation as a single dial. It isn't. Effective longevity planning begins by identifying which source is driving your numbers, because the intervention that quiets metabolic inflammation does little for the autoimmune kind, and vice versa. Here is the working taxonomy.
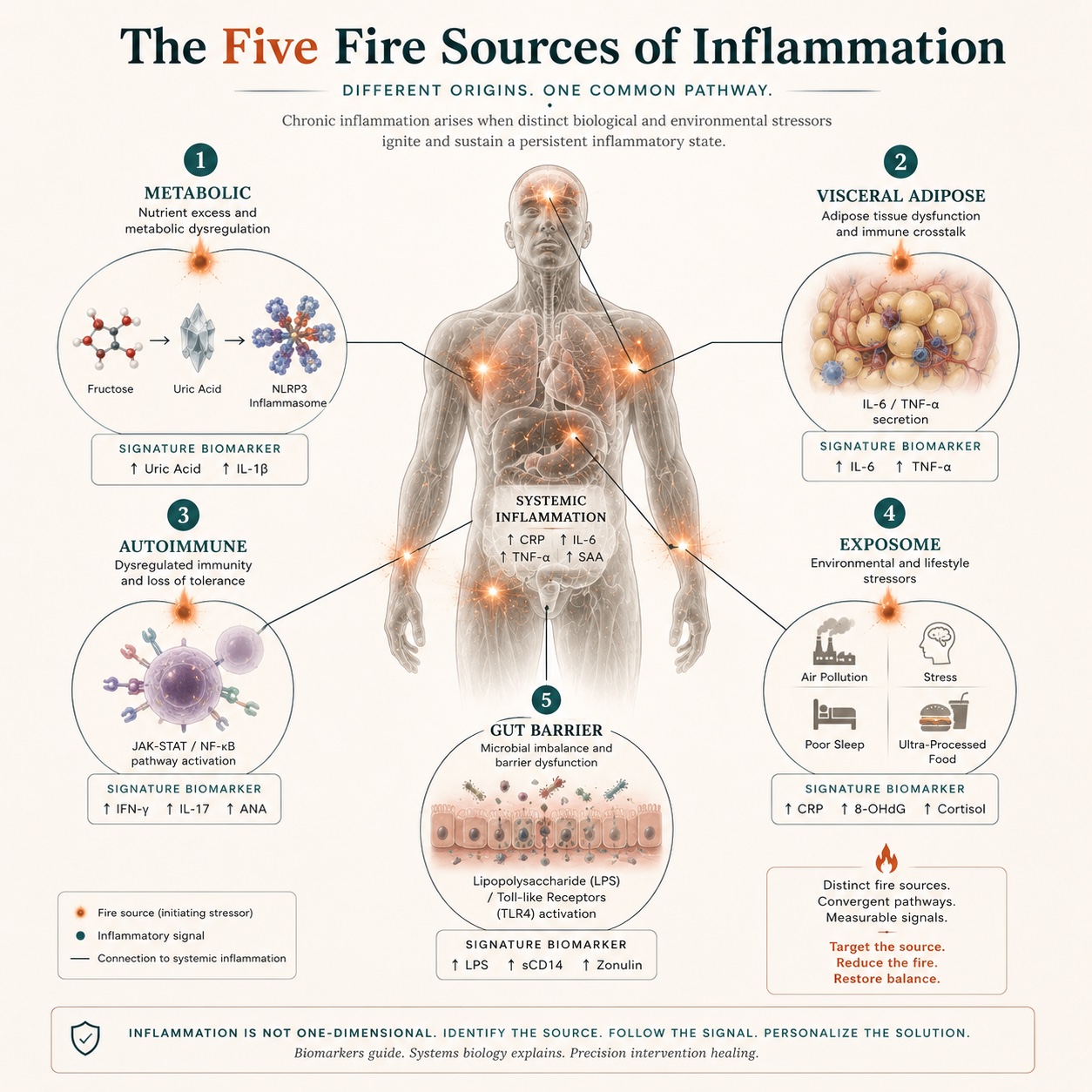
Figure 2. The Five Sources of Chronic Inflammation: Metabolic, Adipose, Autoimmune, Exposome, and Gut-Barrier
Chronic inflammation has at least five distinct origins, each with a signature biomarker and a different intervention. Identifying which "fire" is burning is the first step in any evidence-based anti-inflammatory plan.
1. Metabolic inflammation — the sugar that lights the match
The most common and most modifiable source in the modern world is metabolic. Richard Johnson, a professor of medicine at the University of Colorado Anschutz Medical Campus, has built a decades-long case that fructose — the sugar in sucrose and high-fructose corn syrup — is not merely "empty calories" but an active metabolic signal.[11] Unlike glucose, fructose metabolism generates uric acid inside the cell, and elevated intracellular uric acid drives oxidative stress in the mitochondria and activates the NLRP3 inflammasome — the molecular machine that manufactures inflammatory cytokines. [12] Johnson describes this as flipping a metabolic "fat switch" that our ancestors used to survive famine and that our sodas now leave jammed in the "on" position.[11] The practical signal: chronically elevated uric acid and fasting insulin are early signs of metabolic inflammation long before glucose looks abnormal.
2. Visceral-adipose inflammation — fat as an endocrine organ
Visceral fat is not inert storage; it is metabolically active tissue that secretes inflammatory cytokines (notably IL-6 and TNF-α) and recruits inflammatory macrophages. This is why waist circumference and visceral-fat percentage predict cardiometabolic risk better than weight alone, and why even modest fat loss can meaningfully lower circulating inflammatory markers.
3. Immune and autoimmune inflammation
Here, the repair crew turns on the building. In rheumatoid arthritis, lupus, psoriasis, inflammatory bowel disease, and dozens of related conditions, the immune system attacks the body's own tissues, triggering cytokine cascades via pathways such as JAK-STAT and NF-κB.[1] This category is where the most precise pharmacology already exists — and, as we'll see, where the next generation of therapeutic peptides is aimed.
4. The exposome — your environment, integrated over time
Furman's lab frames many chronic-inflammation drivers as the exposome: the cumulative load of environmental and social insults — air pollution, ultra-processed food, chronic psychological stress, disrupted sleep, sedentary time — that the immune system reads as a continuous, low-grade threat. [2] No single exposure is decisive; the integral over years is.
5. Gut-barrier inflammation
A compromised intestinal barrier ("leaky gut") allows bacterial components, such as lipopolysaccharide, to translocate into the circulation, where they trigger immune activation through Toll-like receptors. Fiber, fermented foods, and microbiome diversity are not wellness decoration here; they are barrier maintenance with measurable downstream effects on systemic markers.
The skeptic's takeaway
"Lower your inflammation" is not an instruction; it's a category error. The useful question is which fire — metabolic, adipose, autoimmune, environmental, or gut — and the only way to answer it is to measure the signals each one leaves behind. That measurement problem is what the rest of this guide is about.
03 / The Resolution Revolution
The opposite of inflammation isn't suppression. It's resolution.
Charles Serhan's discovery that ending inflammation is an active program — not a passive fade-out — rewrote the pharmacology.
For most of the twentieth century, medicine assumed inflammation ended the way a campfire dies: by running out of fuel. Charles Serhan, the Simon Gelman Professor of Anesthesia at Harvard Medical School and director of the Center for Experimental Therapeutics and Reperfusion Injury at Brigham and Women's Hospital, proved that assumption wrong. Resolution, he showed, is not a passive fade — it is an active, tightly orchestrated biochemical program, driven by a class of molecules he named specialized pro-resolving mediators (SPMs).[5]
These mediators — the resolvins, protectins, and maresins — are built by the body from omega-3 fatty acids (EPA and DHA), along with the arachidonic-acid-derived lipoxins.[5] They don't merely block inflammatory signals the way ibuprofen does; they actively tell neutrophils to stop arriving, instruct macrophages to clear cellular debris, and return the tissue to homeostasis.[6] Serhan's distinction is profound for anyone thinking about longevity: a drug that suppresses inflammation can leave the wreckage un-cleared, while the body's own resolution program finishes the job and walks away.
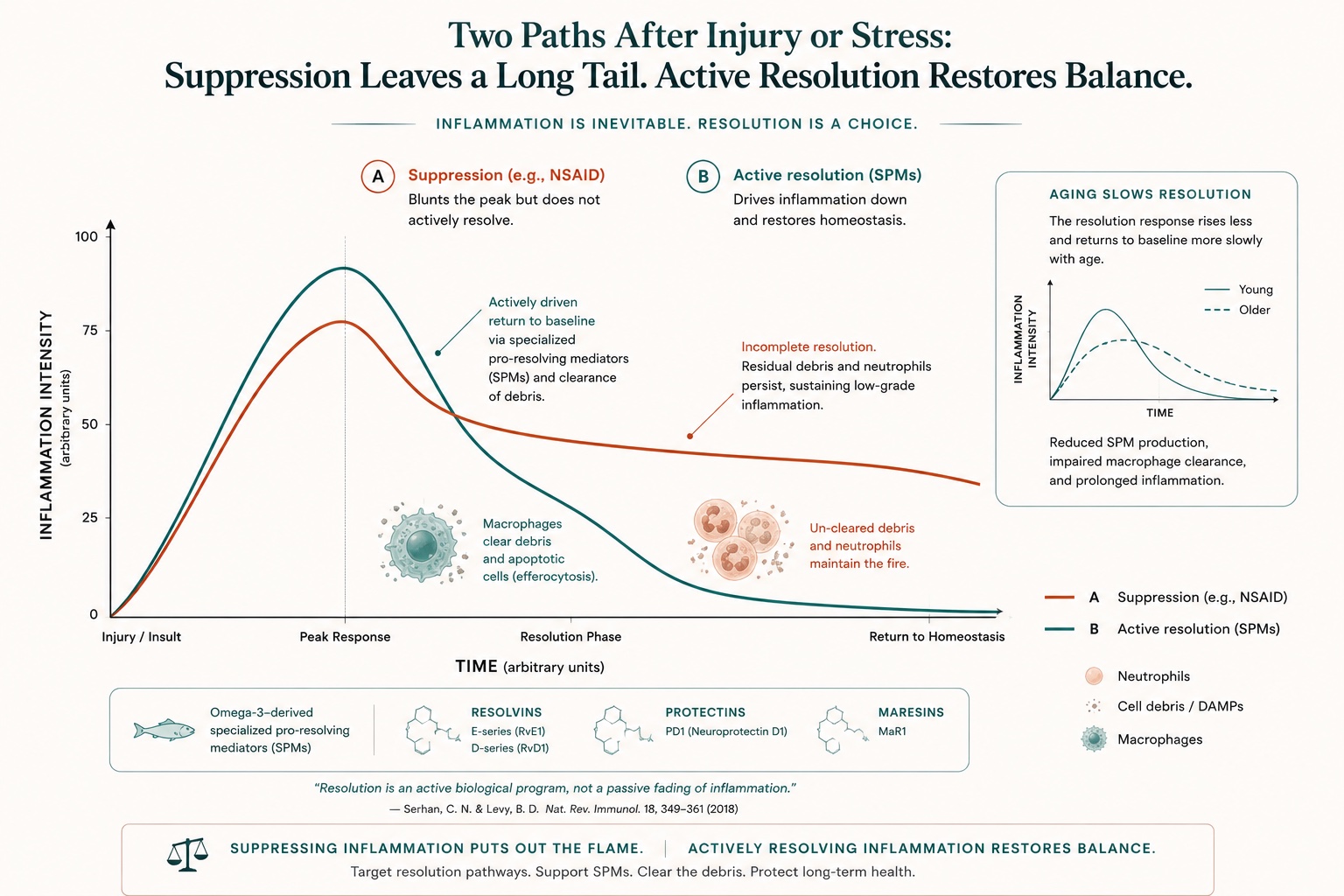
Figure 3. Resolution vs. Suppression of Inflammation: How Omega-3-Derived Specialized Pro-Resolving Mediators Clear Tissue
Charles Serhan showed that ending inflammation is an active program driven by omega-3-derived specialized pro-resolving mediators — not a passive fade. The capacity to resolve declines with age, which may contribute to age-related tissue loss.
The aging angle is the part that should make every reader over forty sit up. In animal models, the ability to produce these resolution mediators declines with age — meaning older bodies don't just inflame more easily, they resolve more slowly.[6] Some of the loss of muscle and tissue quality we attribute to "getting old" may be, in part, a failure to resolve. This reframes omega-3 supplementation: its value may lie less in blunting inflammation and more in supplying the raw material for the body's resolution machinery.
Anti-inflammation says, "stop the fire." Resolution says, "and now clean up, repair the wall, and send the trucks home." Aging is, in part, the slow loss of the second instruction.
04 / If You Can't Measure It, You're Guessing
The biomarkers and the inflammatory clock
From a five-dollar hs-CRP test to a deep-learning "immune age" — how inflammation became quantifiable.
The cheapest, most validated entry point is high-sensitivity C-reactive protein (hs-CRP), a liver-made protein that rises in response to inflammatory cytokines. It is the marker that drove CANTOS enrollment, the marker that consumer panels lead with, and a number you can act on. Broadly, hs-CRP under 1 mg/L signals low cardiovascular risk; above 3 mg/L signals active vascular inflammation — often years before any symptom.[16] Add interleukin-6 (IL-6), fibrinogen, ferritin, and uric acid, and you begin to triangulate which of the five fires is burning.
But a single marker is a snapshot, and inflammation is a network. This is where artificial intelligence earned its place in the field. The Buck–Stanford team took the blood immunome of 1,001 people aged 8 to 96 and used deep learning to distill the nonlinear, redundant tangle of cytokine signals into a single number: the inflammatory clock of aging, or iAge.[2] Published in Nature Aging, iAge tracks multimorbidity, frailty, immune decline, and cardiovascular aging — and, validated against the Framingham Heart Study, predicted mortality in roughly 2,500 people.[2]
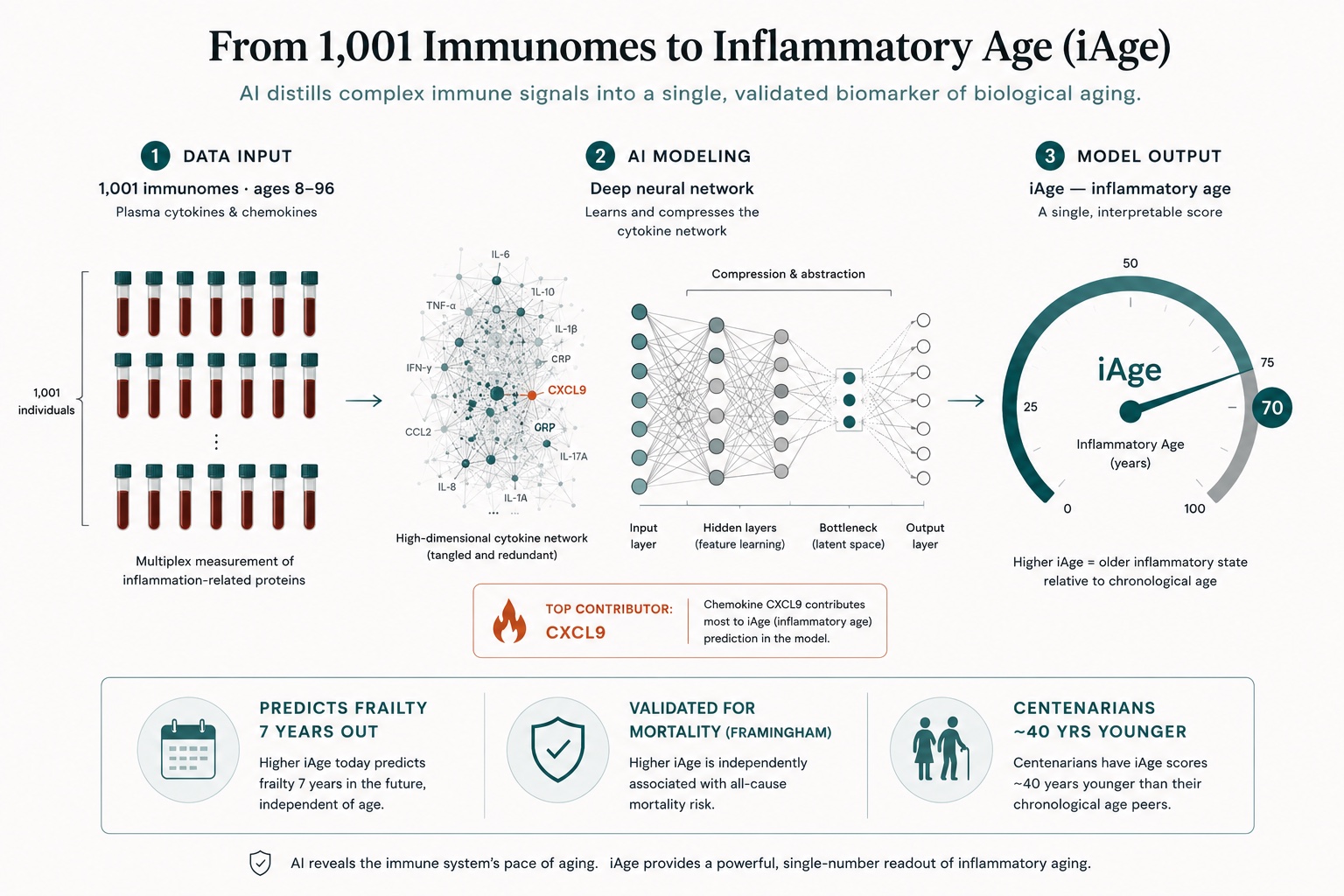
Figure 4. The Inflammatory Clock of Aging (iAge): Deep Learning From 1,001 Immunomes to an Immune-Age Biomarker
Researchers used deep learning on 1,001 blood immunomes to compress the cytokine network into a single "inflammatory age." iAge predicts frailty seven years in advance; its strongest contributor is the chemokine CXCL9.
1,001 blood immunomes were used to train the iAge deep-learning model. [2]
7 years in advance is how early iAge predicted who would become frail. [2]
~40 years is how much younger centenarians' inflammatory age ran versus their calendar age. [3]
The single strongest contributor to iAge turned out to be a chemokine called CXCL9 — a protein normally used to summon immune cells to an infection, but which, in aging blood vessels, drives cellular senescence and adverse cardiac remodeling. Silencing it restored function in aging endothelial cells in both humans and mice.[2] The lesson is structural: predictive modeling turned a redundant cloud of immune proteins into an actionable target. Furman and Stanford's Mark Davis co-founded a company, Edifice Health, to commercialize the iAge concept — one of several signs that inflammatory measurement is moving from the lab bench to the consumer.[3]
Why this matters for planning
An inflammatory marker you measure once is trivia. The same marker measured every quarter, against a stable baseline, while you change one variable at a time, is a feedback loop — and feedback loops are how performance is built. The athlete who tracks hs-CRP through a training block, or the executive who watches uric acid fall as the sodas leave the desk drawer, is doing the same thing the iAge model does, at human scale.
05 / Lever One: Diet
The most powerful anti-inflammatory drug is in the kitchen — and it's mostly subtraction
What the evidence actually supports, stripped of the wellness-industrial complex.
Diet is where the most inflammation is gained and lost, and where the most nonsense is sold. The honest summary is unglamorous. First, subtract the accelerants: added fructose and refined carbohydrate (Johnson's metabolic match), and the chronic caloric excess that builds visceral fat. Second, fix the fat ratio: modern diets are heavy in omega-6 and light in omega-3, and since both compete for the same enzymatic machinery, the balance tilts the body's lipid signaling toward inflammation and away from resolution. Third, feed the barrier and the microbiome: fiber, polyphenols, and fermented foods maintain the gut wall, whose failure drives systemic immune activation.
None of this requires a branded protocol. Large nutrition-epidemiology cohorts have long associated Mediterranean-pattern eating — plants, legumes, fish, olive oil, minimal ultra-processed food — with lower circulating inflammatory markers and lower cardiometabolic risk. The mechanism is the same taxonomy in reverse: less metabolic inflammation, less adipose inflammation, a better-fed barrier, and more omega-3 substrate for Serhan's resolution mediators. The reason this beats any supplement is dose and duration: you eat three times a day, every day, for the rest of your life.
The skeptic's correction to the "anti-inflammatory food" genre is that no single food is a drug. Blueberries and broccoli are not pharmaceuticals; the pattern is the intervention, sustained over years, and measured against your own hs-CRP rather than against a magazine listicle.
06 / Lever Two: Supplements
Three that earn their place — and the fine print everyone skips
Graded by evidence, not by marketing budget.
Most of the supplement aisle is, charitably, untested. A short list has real randomized-trial support for inflammation — and even those come with a caveat that the industry would rather you ignore: the benefit concentrates in people who were deficient or low to begin with. Supplements correct shortfalls; they rarely upgrade the already-sufficient.
Marine omega-3 (EPA/DHA)
Strong evidence.
This is the best-supported anti-inflammatory supplement, and the data are of cardiovascular grade. In REDUCE-IT, led by Deepak Bhatt — then at Brigham and Women's, now the Dr. Valentin Fuster Professor of Cardiovascular Medicine at the Icahn School of Medicine at Mount Sinai — 8,179 statin-treated patients with elevated triglyceride levels received either 4 grams per day of purified EPA (icosapent ethyl) or placebo. The EPA group saw a 25% reduction in major cardiovascular events and a 20% reduction in cardiovascular death.[8] Mechanistically, EPA both lowers triglyceride-rich lipoproteins and supplies the substrate for resolvins. The supplement-aisle version is lower-dose, but the VITAL trial — with 25,871 participants — found that omega-3 modestly lowered hs-CRP and cut heart attacks by about 40%, specifically in people who rarely ate fish.[18] Translation: biggest payoff for the omega-3-deficient.
Vitamin D3
Moderate evidence.
The VITAL trial, co-led by Harvard's JoAnn Manson, followed more than 25,000 adults and found that vitamin D supplementation (with or without omega-3) reduced the incidence of autoimmune disease — rheumatoid arthritis, psoriasis, lupus and others — by 22% over roughly five years.[9] In the trial's inflammation sub-study, vitamin D3 lowered hs-CRP by about 19% at two years.[10] The fine print, in Manson's own framing, is that the people who benefit most are those who start with lower intake; the already-replete may gain little, and very high doses carry their own risks.[18] This is the figure that vindicates the field's emphasis on testing first — a lesson long associated with vitamin D researcher Michael Holick.
Curcumin
Moderate evidence.
Curcumin, the active polyphenol in turmeric, has repeatedly reduced inflammatory markers such as CRP in randomized trials, though it sits a notch below omega-3 and vitamin D on both effect size and bioavailability — most of it is poorly absorbed without formulation help.[18] A reasonable adjunct; not a foundation.
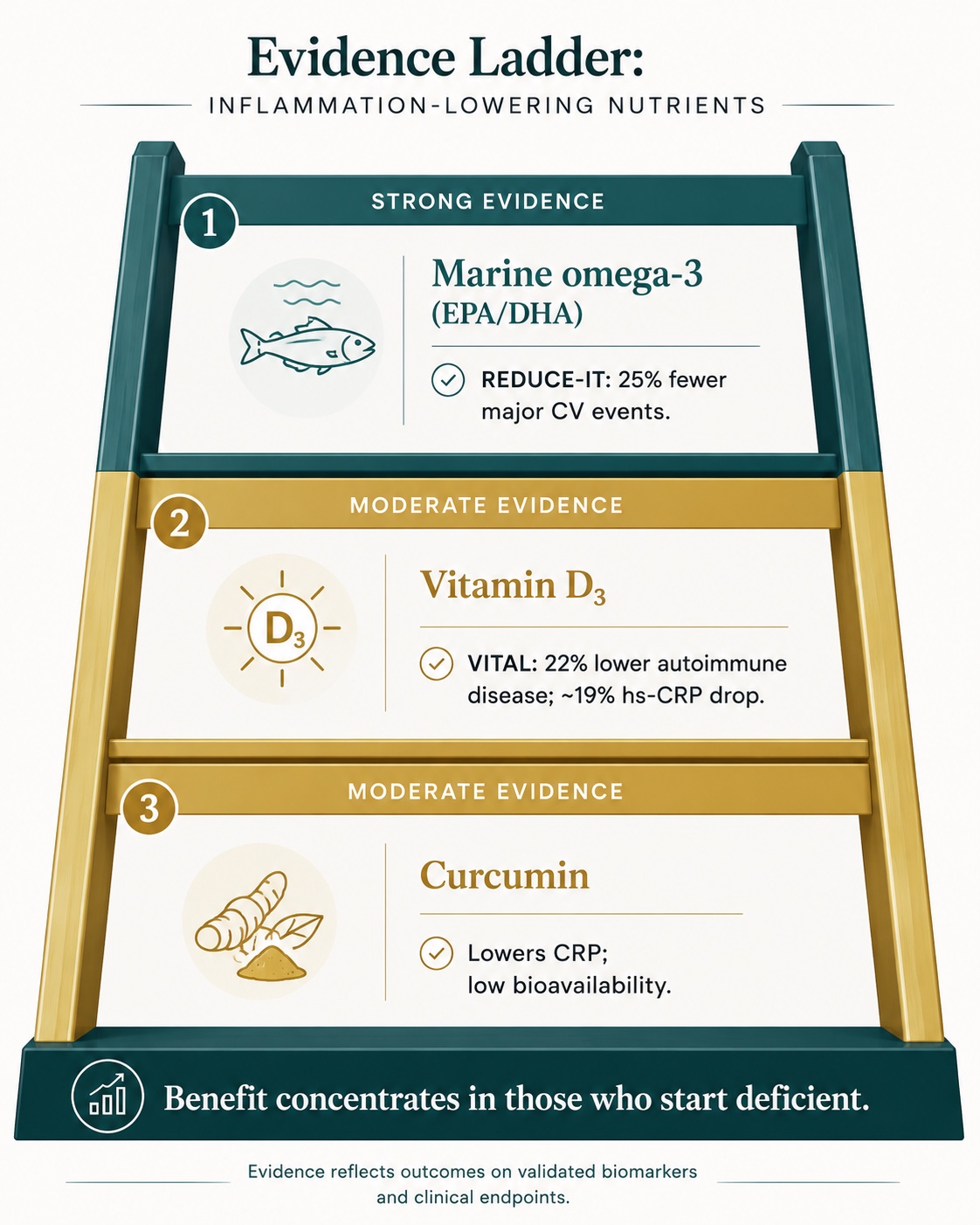
Figure 5. Evidence-Graded Anti-Inflammatory Supplements: Omega-3, Vitamin D, and Curcumin Ranked by Randomized-Trial Support
Only a short list of supplements has randomized-trial support for lowering inflammation — and the benefit concentrates in people who began deficient. Omega-3 leads; vitamin D and curcumin follow.
The pattern, not the pill
Notice the through-line: omega-3, vitamin D, and curcumin all post their best numbers in people who were short on them. That is the entire argument for measurement-first supplementation. Blanket dosing wastes money on the sufficient and under-doses the deficient. A panel that includes 25-hydroxyvitamin D, an omega-3 index, and hs-CRP turns "should I take this?" into a number.
07 / Lever Three: Peptides
The most promising — and most overhyped — frontier in inflammation
A clear-eyed split between peptides with real human evidence and those with a marketing budget.
Peptides are short chains of amino acids — the body's own signaling vocabulary — and they are genuinely one of the most exciting frontiers in anti-inflammatory medicine. They also sit at the center of more hype, and more legal gray area than anything else in this guide. Honesty requires splitting the category into two.
The legitimate frontier: therapeutic anti-inflammatory peptides
In the research literature, peptides are being engineered to do precisely what small-molecule drugs do clumsily: hit a single inflammatory target with high selectivity and few side effects.[1] A 2018 review out of the University of Naples Federico II cataloged the state of the art — SOCS-mimetic peptides that dampen the JAK-STAT pathway driving autoimmune and inflammation-linked cancers; an annexin-A1-derived tripeptide (MC-12) that suppresses NF-κB in models of inflammatory bowel disease; an IL-15 antagonist aimed at rheumatoid arthritis; and a cyclotide that calms T-cell proliferation in multiple sclerosis.[1] This is real, mechanistically grounded science, and it is where the field's credibility lives.
The consumer frontier: "repair" peptides, and a hard dose of reality
Then there is the world the over-40 athlete actually encounters — the med-spa and telehealth menu of BPC-157, TB-500 (a thymosin-β4 fragment), thymosin-α1, CJC-1295, ipamorelin, and KPV, marketed for healing, recovery, and "longevity optimization." The mechanistic stories are plausible, and the preclinical data are real: BPC-157 alone has well over a hundred animal studies behind it.[13] But plausible is not proven. Here is the unvarnished status:
What every buyer must know about repair peptides
None are FDA-approved for these uses. Human clinical evidence is thin to nonexistent — a handful of small trials, none meeting the bar for drug approval.[13]
In late 2023, the FDA moved roughly 17–19 of these peptides — including BPC-157 and TB-500 — to Category 2 bulk substances, citing immunogenicity, impurity, and safety concerns, which barred compounding pharmacies from legally preparing them.[13] Much of what's sold online carries a "research chemical, not for human consumption" label as a legal dodge.[14]
For any tested athlete, this is also a four-year-ban problem: BPC-157 and TB-500 are prohibited at all times under the World Anti-Doping Agency's S0 "unapproved substances" category.[14]
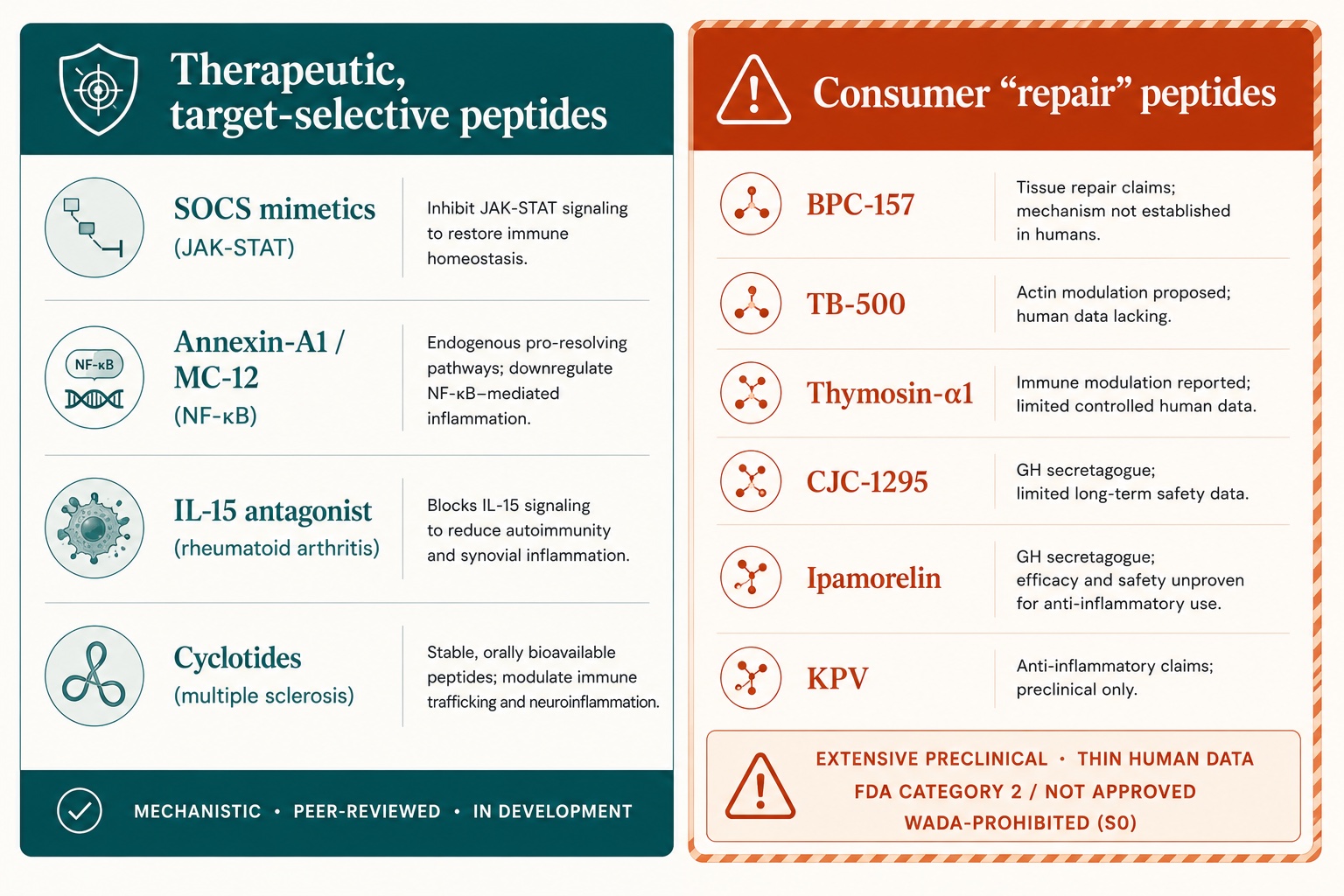
Figure 6. Therapeutic vs. Consumer "Repair" Peptides: Evidence Level and FDA / WADA Status for Inflammation
Anti-inflammatory peptides split into two worlds: target-selective therapeutics with peer-reviewed mechanisms, and popular "repair" peptides (BPC-157, TB-500) that remain largely preclinical, are not FDA-approved, and are banned in tested sports.
So where does that leave the serious, skeptical reader? Not at "never" — the science may yet earn approval, and a 2026 reclassification debate is underway — but at "not yet, and not blind." If Peptide Therapy enters your plan at all, it belongs under a qualified physician, with informed consent about the evidence gap, sourced through legitimate channels, and — crucially — measured. Which is exactly the problem the next section was built to solve.
08 / The Intelligence Layer
A Digital Twin for Predictive Peptide Performance™
If peptides are the highest-variance lever, they are also the one that most needs measurement, modeling, and a human in the loop. Here's how AI changes the equation.
The honest weakness of the entire peptide category is the same as its appeal: high individual variability and almost no population data to anchor a dose. That is precisely the kind of problem AI is built for — not to manufacture certainty, but to turn one person's response into a learning signal. At LongevityPlan.AI, the conceptual architecture we describe as a Digital Twin for Predictive Peptide Performance™ is designed to do for an individual what iAge did for a population: compress messy, multi-dimensional inputs into an actionable read.
It works in two strata. The sensor layer gathers multimodal health data — wearable recovery and heart rate variability signals, sleep architecture, continuous glucose monitoring where relevant, training load, and quarterly bloodwork (hs-CRP, IL-6, uric acid, omega-3 index, vitamin D). The intelligence layer then models how a given individual's inflammatory and recovery markers respond to a given intervention over time, flags non-responders early, and surfaces trends that a single lab draw would hide. The output is not a prescription; it is evidence, handed to a Coach / Practitioner who makes the call with the Athlete / Patient in front of them.
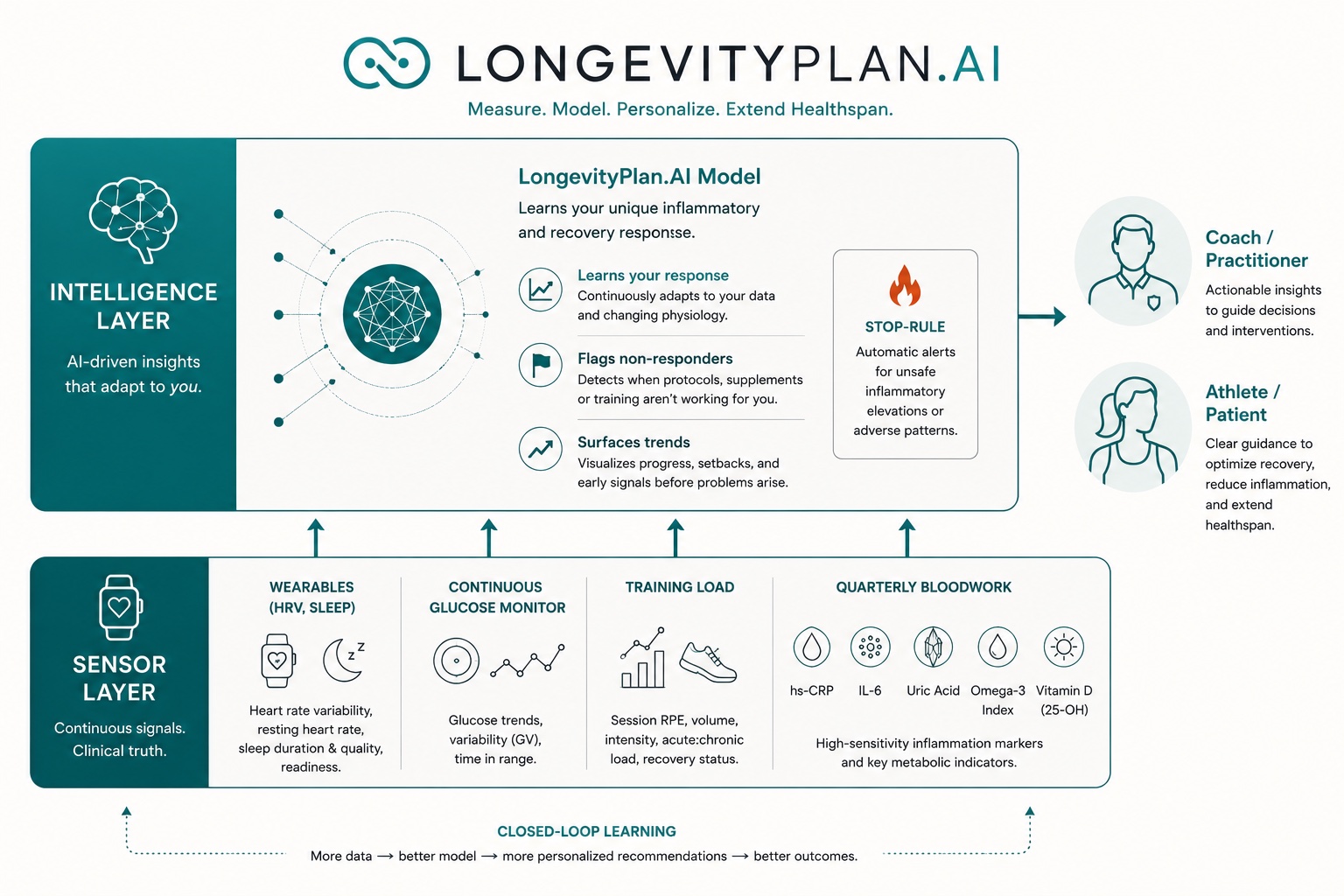
Figure 7. Digital Twin for Predictive Peptide Performance™: Sensor-Layer and Intelligence-Layer Architecture
A conceptual two-layer architecture: a sensor layer of multi-modal health data feeds an intelligence layer that models each individual's inflammatory response — turning a high-variance intervention into a monitored experiment of one, with a practitioner in the loop.
What the twin does — and pointedly does not do
It does not launder an unapproved drug into legitimacy, and it does not replace a physician's judgment. What it does is convert a high-uncertainty intervention into a monitored experiment of one: a documented baseline, a single changed variable, a measured response, and a clear stopping rule if inflammatory or safety markers move the wrong way. For a category this thin on human data, disciplined measurement is not a luxury — it is the only responsible way in.
The same engine produces ordinary AI-powered coaching improvements for the far larger group who will never touch a peptide: the executive whose hs-CRP reveals silent metabolic inflammation, the masters cyclist optimizing the omega-3 index for faster resolution between hard blocks, the post-injury patient tracking whether recovery markers are actually trending home. The peptide use case is simply the most demanding stress test of a principle that applies to every lever in this guide — measure, model, intervene, re-measure.
09 / The Buyer's Guide
How the major platforms actually use data and AI
Five ways to put a number on your inflammation — and what each is really selling.
The consumer longevity market has, in the last three years, turned inflammatory measurement into a product. Each platform makes a different bet on the trade-off between raw data, AI interpretation, and human clinical oversight. For the inflammation-focused buyer, each one leads with hs-CRP — the differences lie in what happens next.
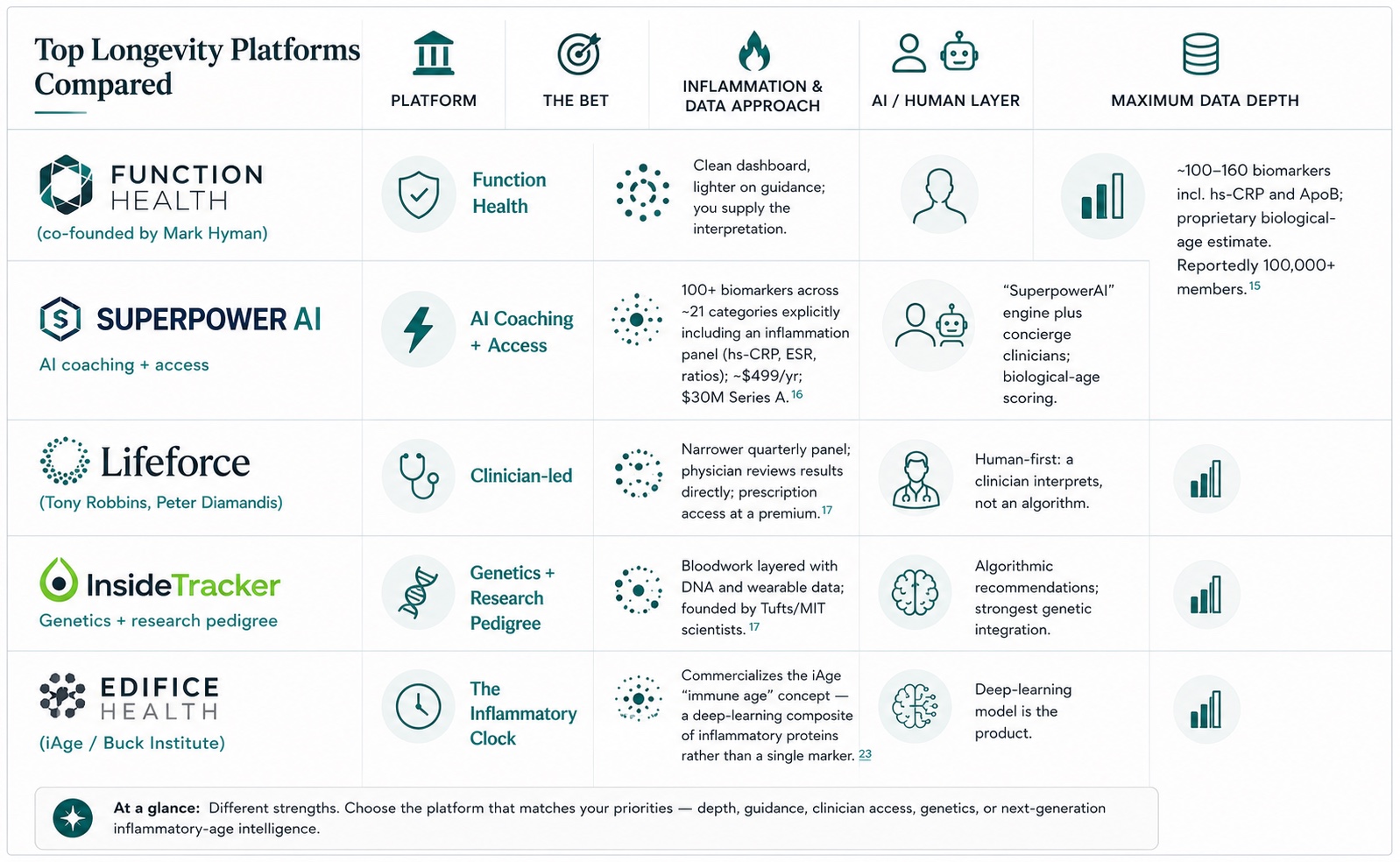
The honest read across the table: data is now cheap, and interpretation is the bottleneck. A panel of 160 biomarkers is worthless to the person who can't tell which three matter, and a beautiful dashboard is not the same as a decision. This is the gap LongevityPlan.AI is built to close — not by selling another blood draw, but by turning the data you already have into a longitudinal model and a plan, with a human practitioner in the loop. The platforms above measure. The work is in what you do with the measurement, quarter after quarter.
Behind these consumer brands sit larger players proving the same thesis at a clinical scale. Novartis's canakinumab (Ilaris) supplied the CANTOS proof that lowering inflammation alone prevents heart attacks.[7] Amarin's icosapent ethyl (Vascepa) carried REDUCE-IT.[8] And the CLIA-certified laboratory infrastructure that runs every hs-CRP on the table above — Quest Diagnostics, Labcorp, and the assay makers behind them — is the quiet utility layer making consumer inflammation testing possible at all. Metabolic-inflammation monitoring, in turn, increasingly leans on continuous glucose hardware from companies like Abbott, closing Richard Johnson's fructose loop in real time.
10 / The Plan
From biology to a quarter-by-quarter program
What a measurement-first inflammation strategy looks like for an individual — and an organization.
Pulling the levers together, a credible anti-inflammatory program is less a list of products than a closed loop. Establish a baseline that names the fire: hs-CRP and IL-6 for inflammatory tone, uric acid and fasting insulin for the metabolic source, an omega-3 index and 25-hydroxyvitamin D for the substrate-and-deficiency question, and waist or visceral-fat metrics for the adipose contribution. Then change the highest-yield variable first — almost always diet and the metabolic accelerants — and re-measure in 90 days. Layer the evidence-graded supplements where the panel shows a deficit. Reserve the experimental, physician-supervised tier — including any Peptide Therapy — for last, and only inside the monitored-experiment discipline described above. This is the spine of what we call a Peptide Longevity Plan™: not a peptide stack, but a sequenced, measured progression in which peptides are the final, optional, closely-watched step rather than the first impulsive one.
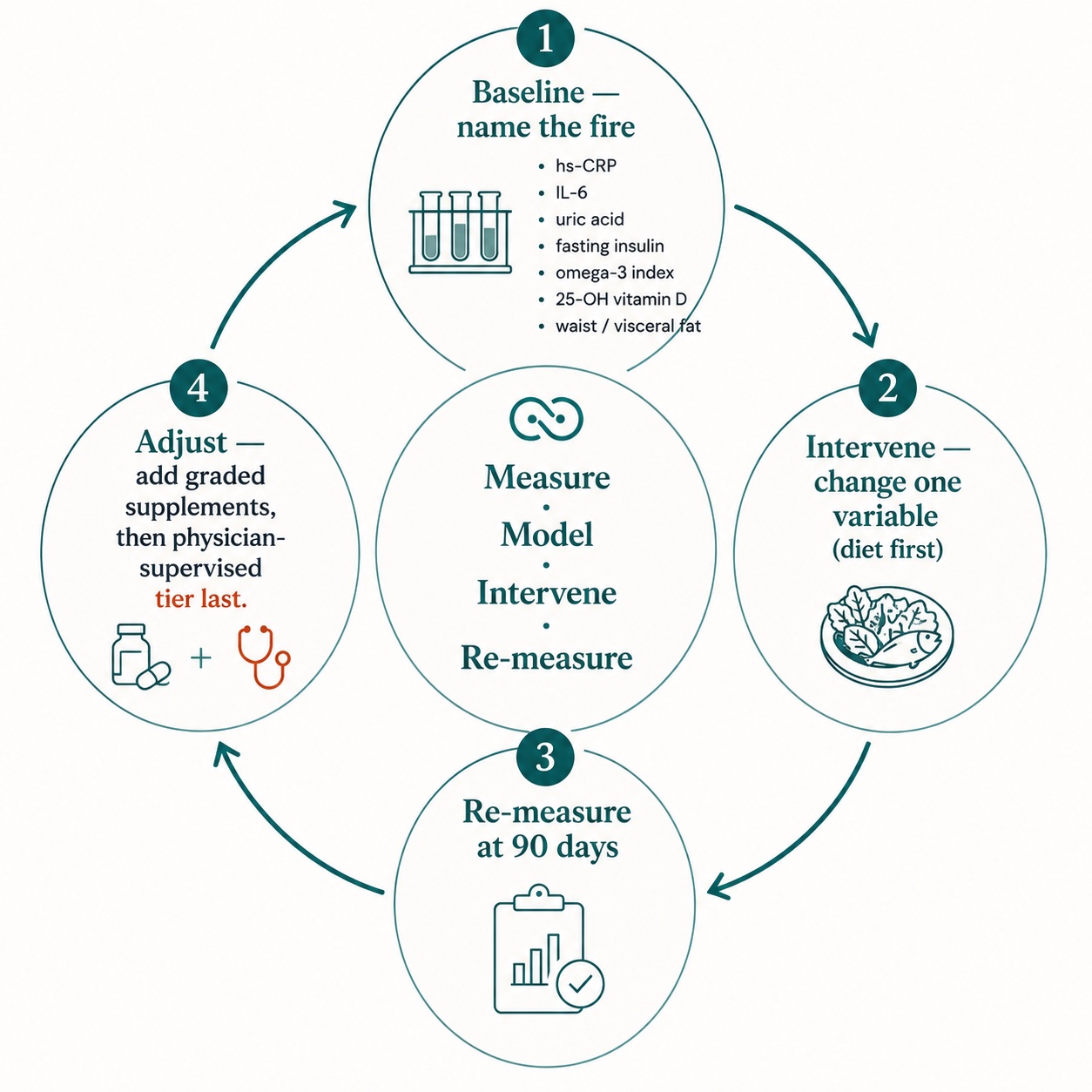
Figure 8. The 90-Day Inflammation Feedback Loop: Baseline, Single-Variable Intervention, Re-Measure, Adjust
A credible anti-inflammatory program is a closed loop, not a product list: establish a biomarker baseline, change the highest-yield variable first, re-measure at 90 days, and reserve experimental tiers for last.
The same architecture scales. The cardiorespiratory and recovery signals that feed an individual's plan are the same ones a Cardiorespiratory Digital Twin™ uses to model an athlete's training load against inflammatory recovery. And for employers, inflammatory load is a remarkably efficient lens on workforce health — much of the multimorbidity that drives healthcare spend traces to systemic chronic inflammation that screening catches years early.[2] A Corporate Wellness Program built on quarterly inflammatory panels, or a peer-supported Longevity Club that keeps members accountable to their own trend lines, applies the identical loop at population scale: measure, intervene, re-measure, and let the data — not the marketing — write the plan.
The goal was never to "fight inflammation." It is to keep the acute fire that heals you, restore the resolution that ages out of you, and extinguish the chronic smolder that's quietly costing you decades — and to prove you're doing it, one quarter at a time.
Ridker's heart-attack survivors didn't lower their cholesterol; they lowered their inflammation, and they lived longer for it. Furman's centenarians carry inflammatory ages decades below their birthdays. Serhan's resolution mediators clean up where suppression leaves a mess. None of this is wellness theater. It is measurable biology, and it is finally cheap enough to measure. The only remaining question is the one this newsletter keeps asking: are you guessing, or are you measuring? Plan accordingly — ideally, before the data would have told you to.
Endnotes & Sources
- La Manna S, Di Natale C, Florio D, Marasco D. "Peptides as Therapeutic Agents for Inflammatory-Related Diseases." Int J Mol Sci. 2018;19(9):2714. PMC6163503.
- Sayed N, Huang Y, Nguyen K, … Davis MM, Furman D. "An inflammatory aging clock (iAge) based on deep learning tracks multimorbidity, immunosenescence, frailty and cardiovascular aging." Nature Aging. 2021;1:598–615. PMC8654267.
- Buck Institute for Research on Aging, "First actionable clock that predicts immunological health and chronic diseases of aging," 2021; and Furman's "10th hallmark" remarks via BioTechniques / Longevity.Technology, 2021.
- Franceschi C, Campisi J. "Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases." J Gerontol A Biol Sci Med Sci. 2014;69(S1):S4–S9.
- Serhan CN, Levy BD. "Resolvins in inflammation: emergence of the pro-resolving superfamily of mediators." J Clin Invest. 2018;128(7):2657–2669. jci.org/97943.
- Serhan CN. "Discovery of specialized pro-resolving mediators marks the dawn of resolution physiology and pharmacology." Mol Aspects Med. 2017;58:1–11; and STEM-Talk Ep. 170 interview, 2024 (age-related decline in resolution mediators).
- Ridker PM, et al. "Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease" (CANTOS). N Engl J Med. 2017;377:1119–1131. 10,061 patients; ~15% reduction in primary CV endpoint, independent of LDL. Ridker quotation via ESC/ScienceDaily, 2017. ACC summary.
- Bhatt DL, et al. "Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia" (REDUCE-IT). N Engl J Med. 2019;380:11–22. 8,179 patients; 25% reduction in major CV events, 20% reduction in CV death. nejm.org.
- Hahn J, Cook NR, … Manson JE, Costenbader KH. "Vitamin D and marine omega-3 fatty acid supplementation and incident autoimmune disease: VITAL randomized controlled trial." BMJ. 2022. 25,871 participants; vitamin D reduced autoimmune disease ~22%.
- "Effects of Vitamin D3 and Marine Omega-3 Fatty Acids Supplementation on Biomarkers of Systemic Inflammation: 4-Year Findings from the VITAL Randomized Trial." Nutrients. 2022. Vitamin D3 lowered hs-CRP ~19% at year 2. PMC9782648.
- Johnson RJ, et al. "The fructose survival hypothesis for obesity." Phil Trans R Soc B. 2023. PMC10363705; and "Five questions for Richard Johnson," University of Colorado, 2023 (the metabolic "fat switch").
- Johnson RJ lab. Work on uric acid, NLRP3 inflammasome activation, and beta-hydroxybutyrate, University of Colorado Anschutz Medical Campus. See Department of Medicine grand-rounds materials and lab publications, 2024.
- U.S. FDA bulk-substance Category 2 reclassification of ~17–19 peptides (incl. BPC-157, TB-500), late 2023; preclinical-vs-human evidence gap discussed in Pharmacy Times, 2026, and DJ Holt Law regulatory review, 2025.
- U.S. Anti-Doping Agency, "BPC-157: Experimental Peptide Creates Risk for Athletes" (WADA S0 prohibited); BSCG, "TB-500 — Status, Risks, and Bans," on four-year WADA sanctions and "research chemical" labeling.
- Function Health membership and biomarker panel details; Mark Hyman co-founder; ~100,000 members reported. Fierce Healthcare, April 2025; finvsfin platform comparison, 2026.
- Superpower: $30M Series A; 100+ biomarkers across ~21 categories including an inflammation panel; hs-CRP educational materials. Fierce Healthcare, April 2025; superpower.com.
- Platform comparison (Function Health vs Superpower vs InsideTracker vs Lifeforce), finvsfin, 2026; Lifeforce co-founded by Tony Robbins and Peter Diamandis (clinician-led); InsideTracker founded by Tufts/MIT scientists.
- Manson JE, VITAL Research Group; Scientific American, "Three anti-inflammatory supplements can really fight disease" (omega-3, vitamin D, curcumin; benefit concentrated in low-intake individuals), Feb 2026. VITAL principal results, PMC7089819.
- Furman D et al. "Expression of specific inflammasome gene modules stratifies older individuals into two extreme clinical and immunological states." Nat Med. 2017;23:174–184 (foundational to inflammaging stratification).
- Serhan CN. "Pro-resolving lipid mediators are leads for resolution physiology." Nature. 2014;510(7503):92–101 (defining statement of resolution pharmacology).
- Everett BM, … Ridker PM. "Inhibition of Interleukin-1β and Reduction in Atherothrombotic Cardiovascular Events in the CANTOS Trial." J Am Coll Cardiol. 2020;76:1660–1670 (total-event burden analysis).
- Resolvins and metabolic disease: "Resolvins, Specialized Pro-Resolving Lipid Mediators and their Potential Roles in Metabolic Diseases," Serhan lab. PMC3947989. #Longevity #Inflammation #Inflammaging #PreventiveMedicine #PrecisionMedicine #Healthspan #Resolvins #Omega3 #Biomarkers #hsCRP #DigitalTwin #AIinHealthcare #PeptideTherapy #CardiovascularHealth #MetabolicHealth #FunctionalMedicine #LongevityPlanAI
Disclaimer: This article is for educational and informational purposes only and is not medical advice. It is not a substitute for diagnosis or treatment by a licensed physician, and nothing here should be taken as an endorsement of any specific product, company, or therapy. Peptides such as BPC-157 and TB-500 are not FDA-approved for the uses discussed, are restricted from pharmacy compounding, and are prohibited in tested sport; any consideration of peptide therapy should occur only under qualified medical supervision. Clinical-trial figures, biomarker thresholds, and company details were verified against the cited sources as of publication and are subject to change. Always consult your healthcare provider before changing your diet, supplements, or medications.© LongevityPlan.AI · Research. Cardiorespiratory Digital Twin™, Digital Twin for Predictive Peptide Performance™, and Peptide Longevity Plan™ are trademarks of LongevityPlan.AI.