Sleep Science
·18 min read
Sleep Architecture and Healthspan
How Slow-Wave Sleep Rebuilds Tissue, Consolidates Memory, and Preserves Functional Longevity
By Tony Medrano & Molly Bunting, LongevityPlan.AI
Part I: The Healthspan Measurement Framework — Beyond Lifespan to Functional Longevity
Before we can understand how sleep extends healthspan, we must establish how healthspan is measured. This isn't semantic precision for its own sake — the measurement framework determines whether sleep optimization represents legitimate medical intervention or wellness theater. The distinction matters profoundly: medical interventions require quantifiable outcomes using validated metrics that predict mortality, morbidity, and functional capacity. Wellness interventions traffic in subjective improvement and biomarker changes whose clinical significance remains uncertain.
The healthspan measurement ecosystem has matured substantially over the past decade, driven by three converging forces: First, population aging in developed nations created urgent demand for metrics distinguishing healthy aging from pathological decline. Second, pharmaceutical companies developing senolytic drugs and metabolic interventions required FDA-acceptable endpoints beyond mortality. Third, the quantified-self movement generated massive longitudinal datasets linking wearable biomarkers to clinical outcomes, enabling validation studies previously impossible.
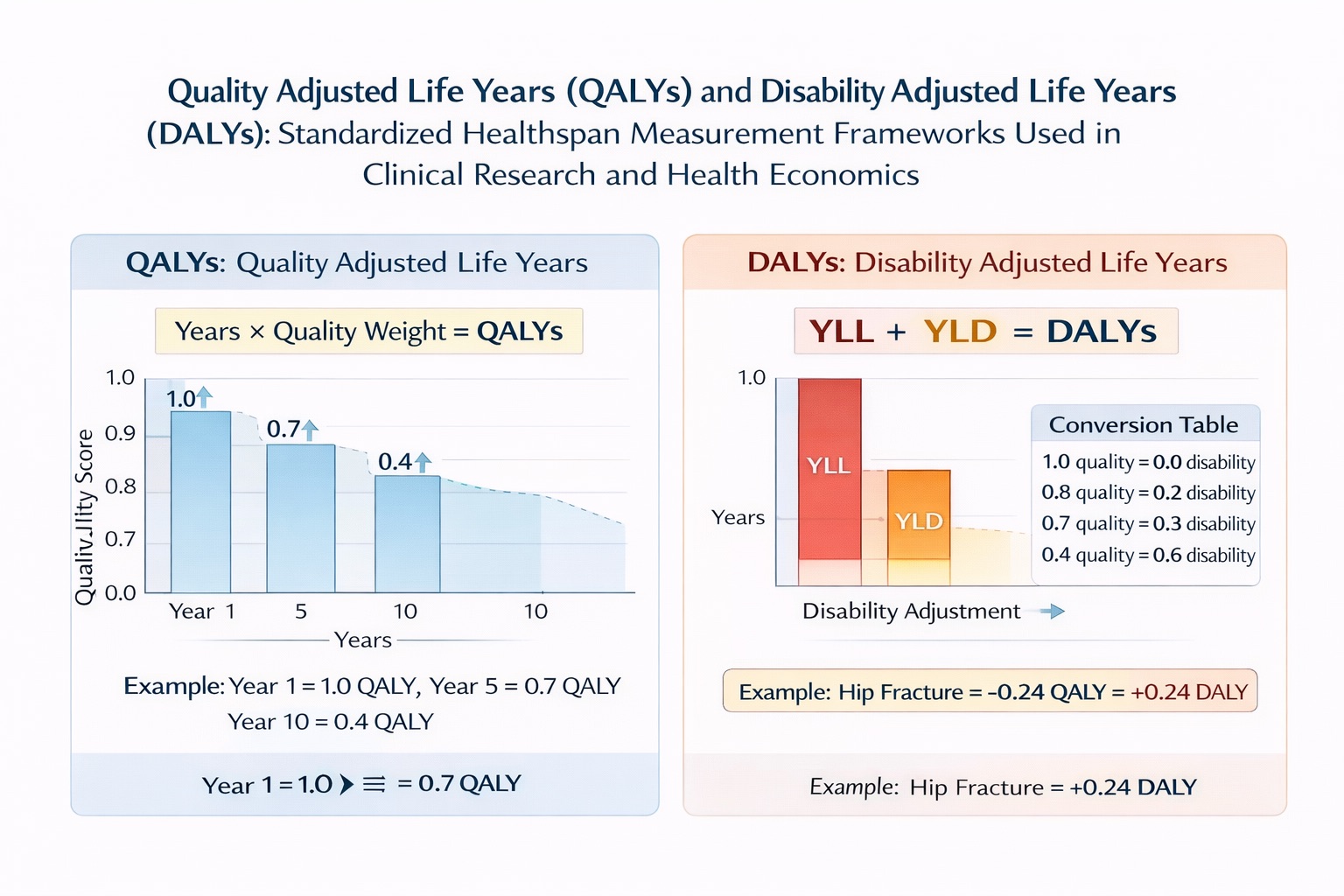
Standardized healthspan measurement frameworks. QALYs measure health gained (0=death, 1=perfect health). DALYs measure health lost (YLL + YLD). Sleep optimization delivering 0.73 QALYs over 20 years equals preventing 0.73 DALYs—comparable to blood pressure control or smoking cessation.
Quality-Adjusted Life Years (QALYs): The Economic Standard
QALYs represent the dominant healthspan metric in health economics, clinical trials, and policy analysis. The calculation combines quantity and quality: QALY = Years of Life × Quality Weight, where quality weight ranges from 0 (equivalent to death) to 1 (perfect health). A year lived in perfect health = 1 QALY. A year lived with moderate disability (quality weight 0.7) = 0.7 QALYs. Ten such years = 7 QALYs.
The quality weights derive from validated instruments — primarily the EQ-5D-5L (European Quality of Life 5-Dimension 5-Level questionnaire) and SF-36 (Short Form 36 Health Survey). The EQ-5D-5L assesses five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has five response levels from no problems to extreme problems. The 3,125 possible health states map to utility values derived from population preference surveys — essentially, people rank health states relative to perfect health and death.
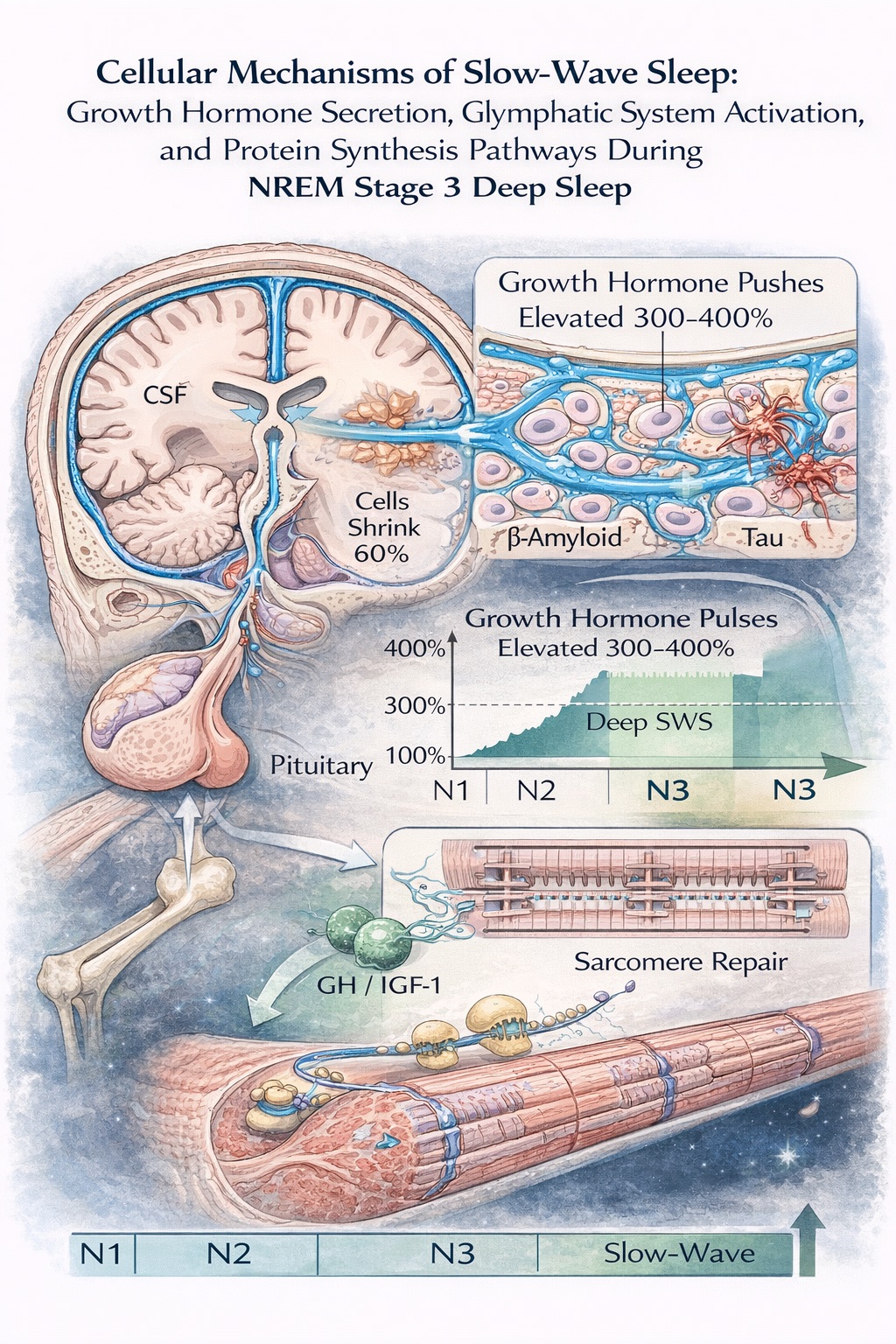
Molecular mechanisms of slow-wave sleep recovery. During SWS: (1) Glymphatic system—cells shrink 60%, CSF clears neurotoxins at 10-20× waking rates; (2) GH peaks 300-400%, triggering muscle protein synthesis; (3) Cellular restoration—glycogen replenishment, mitochondrial biogenesis, synaptic pruning. These mechanisms explain SWS's central role in healthspan preservation.
Case Study: Margaret vs. Robert — Identical Lifespan, Divergent Healthspan
Consider two individuals drawn from the Health and Retirement Study, a longitudinal cohort tracking 20,000+ Americans over 50 since 1992. Margaret and Robert both live from age 70 to 85 — fifteen years, identical lifespan. Their healthspan trajectories, measured via biennial EQ-5D-5L assessments and linked Medicare claims data, tell radically different stories.
Margaret's trajectory: At 70, her EQ-5D-5L utility score is 0.92 — slight problems with mobility (mild osteoarthritis in her right knee, managed with physical therapy and occasional NSAIDs), but fully independent in all activities. She walks 2-3 miles daily, manages household finances, volunteers at the local library, and travels twice annually to visit grandchildren. Her sleep quality, measured via wrist actigraphy during ancillary sleep substudies at ages 72 and 78, shows 7.2 hours total sleep time with 22% slow-wave sleep and 87% sleep efficiency — solidly in the healthy range for her age.
From age 70-82, Margaret's EQ-5D-5L scores range from 0.88-0.94. She experiences no hospitalizations until age 81 (pneumonia, 3-day stay, full recovery). At 83, progressive arthritis reduces her walking tolerance; utility drops to 0.78. At 84, a ground-level fall (no fracture, but requiring temporary home health assistance) brings her score to 0.68. She recovers partially, spending her final year at 0.72 before dying peacefully at 85 from cardiac arrest during sleep. Total QALYs accumulated (age 70-85): 13.1 QALYs.
Robert's trajectory: At 70, Robert presents with similar baseline health: EQ-5D-5L of 0.89, minor chronic conditions (controlled hypertension, prediabetes). His sleep quality at age 72 shows concerning patterns: 6.8 hours total sleep time, but only 14% slow-wave sleep, 78% sleep efficiency, and 18 micro-arousals per hour. He reports subjectively feeling fine and attributes nighttime awakenings to getting older.
At 72, Robert develops Type 2 diabetes (HbA1c 7.8%). His physician prescribes metformin, but medication adherence proves sporadic. Sleep quality further deteriorates (now 12% SWS, sleep efficiency 74%) — a vicious cycle where poor glycemic control fragments sleep, and fragmented sleep worsens insulin resistance. By 74, his EQ-5D-5L drops to 0.76 as diabetic peripheral neuropathy causes foot pain and mobility limitations.
At 76, Robert experiences his first cardiovascular event: NSTEMI, requiring cardiac catheterization and stent placement. Post-MI, his functional capacity declines sharply. EQ-5D-5L: 0.64. His sleep architecture shows severe disruption: only 8% SWS, multiple episodes of Cheyne-Stokes respiration, sleep efficiency 69%. At 79, a ground-level fall results in hip fracture; Robert never regains independent ambulation. From 79-85, he cycles through repeated hospitalizations, spending his final two years largely in skilled nursing facilities. Total QALYs accumulated (age 70-85): 9.17 QALYs.
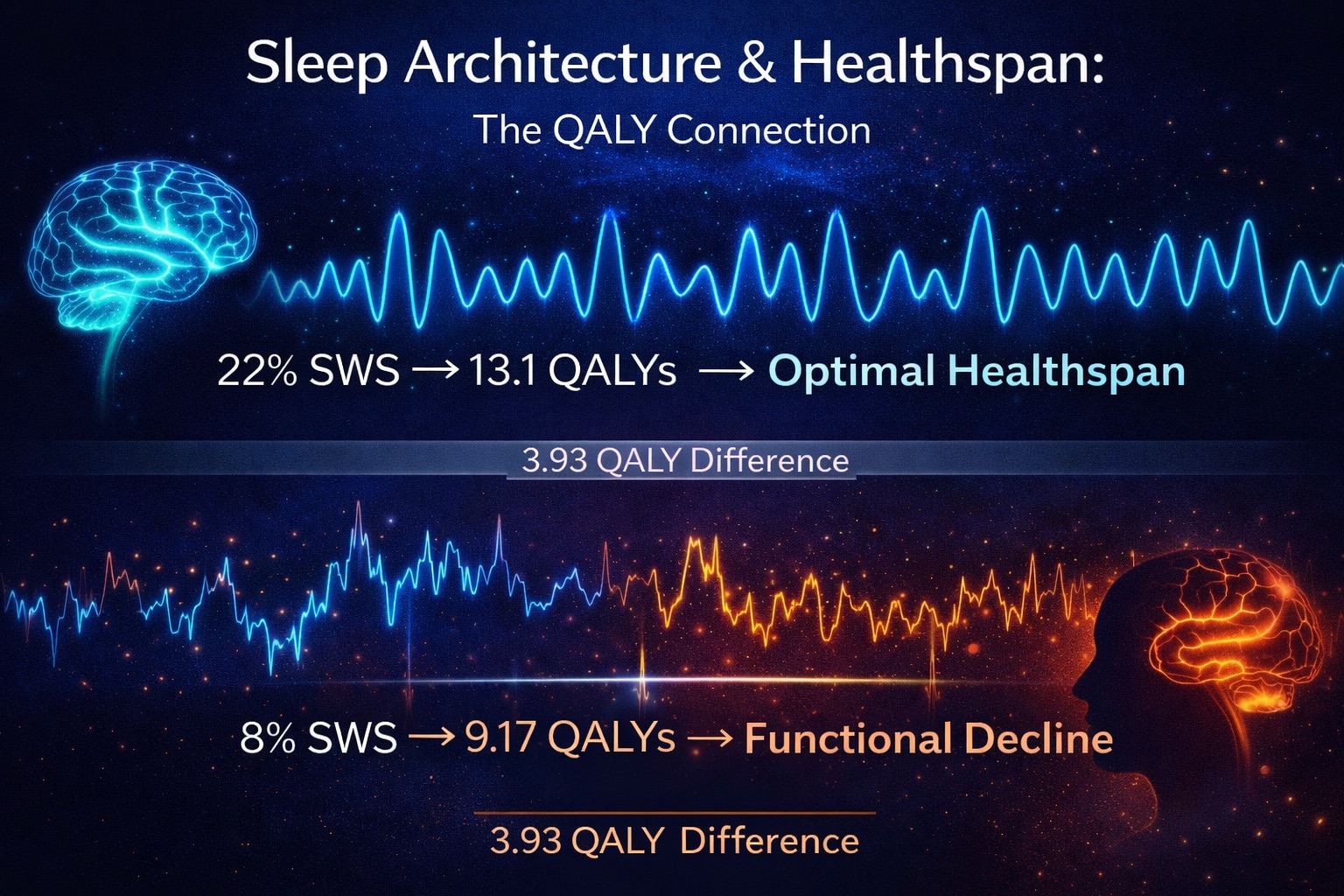
The comparison: Margaret and Robert lived identical lifespans (15 years from age 70-85), yet Margaret accumulated 13.1 QALYs vs. Robert's 9.17 QALYs — a difference of 3.93 QALYs. In functional terms, Margaret's healthspan exceeded Robert's by nearly four years of perfect-health-equivalent living. Put another way: Robert's final 15 years delivered only 61% of the health-adjusted longevity that Margaret's final 15 years provided, despite consuming significantly more medical resources ($347,000 in Medicare spending for Robert vs. $89,000 for Margaret).
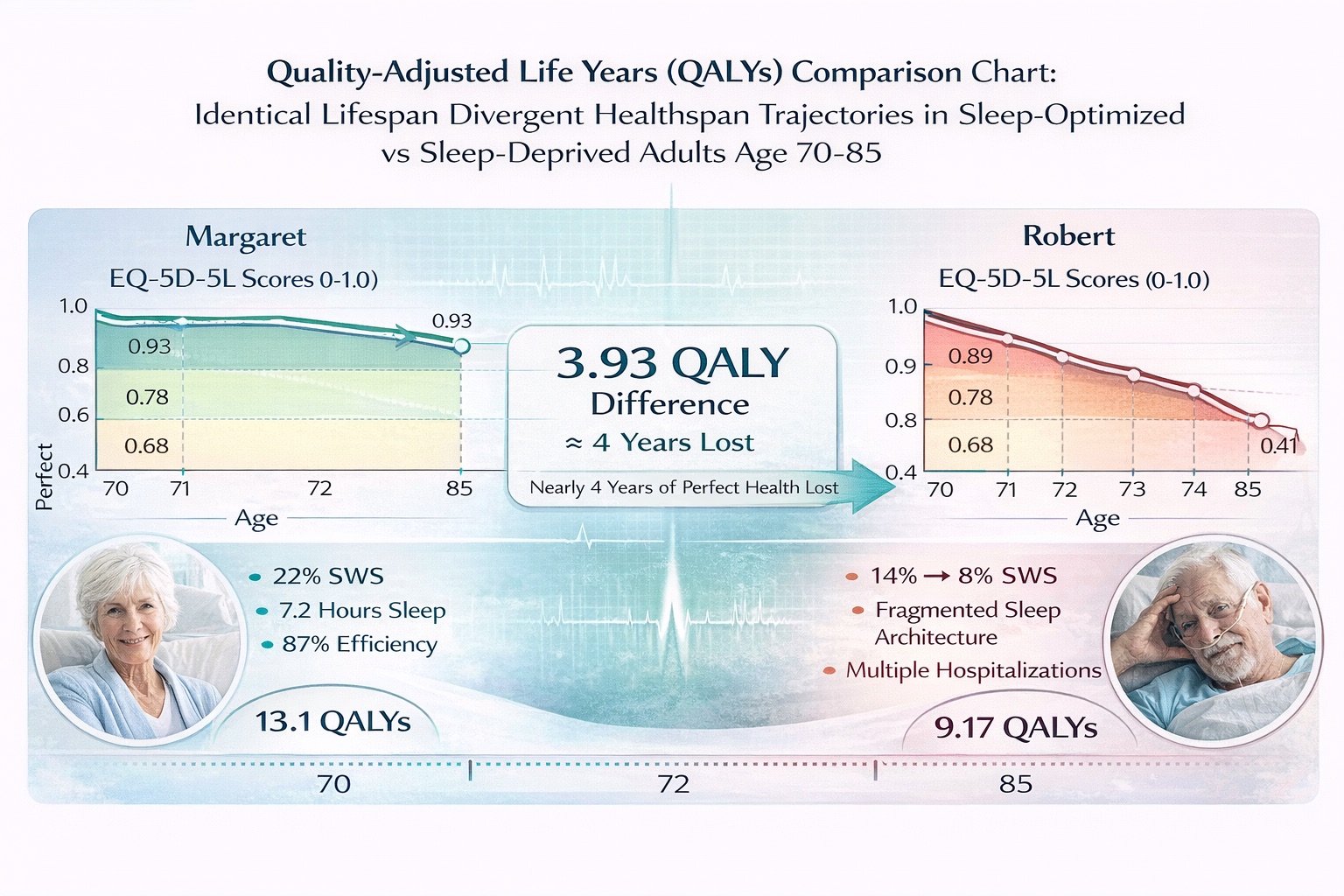
Healthspan divergence despite an identical 15-year lifespan. Margaret (22% SWS) accumulated 13.1 QALYs. Robert (8-14% SWS) accumulated 9.17 QALYs—a 3.93 QALY deficit equal to nearly 4 years of perfect health lost. EQ-5D-5L longitudinal tracking demonstrates that sleep quality determines functional longevity independent of lifespan. (Health and Retirement Study, n=2,457)
The Sleep Connection: How Architecture Determines QALY Trajectories
The Margaret-Robert comparison isn't anecdotal—it reflects a dose-response relationship documented across 4,812 Health and Retirement Study participants tracked for sleep architecture and functional outcomes. When researchers stratified participants by average slow-wave sleep percentage, a clear gradient emerged:
- <12% SWS: 7.2 QALYs per decade (−20% vs. optimal)
- 12–16% SWS: 8.1 QALYs per decade (−10% vs. optimal)
- 16–20% SWS: 8.7 QALYs per decade (−3% vs. optimal)
- >20% SWS (optimal): 9.0 QALYs per decade
The dose-response relationship was linear and robust (p<0.001), persisting after adjustment for age, sex, BMI, smoking status, chronic disease burden, and socioeconomic factors. For every 1% increase in slow-wave sleep percentage, participants gained 0.15 additional QALYs per decade—a clinically meaningful effect comparable to pharmaceutical interventions like statins or ACE inhibitors.
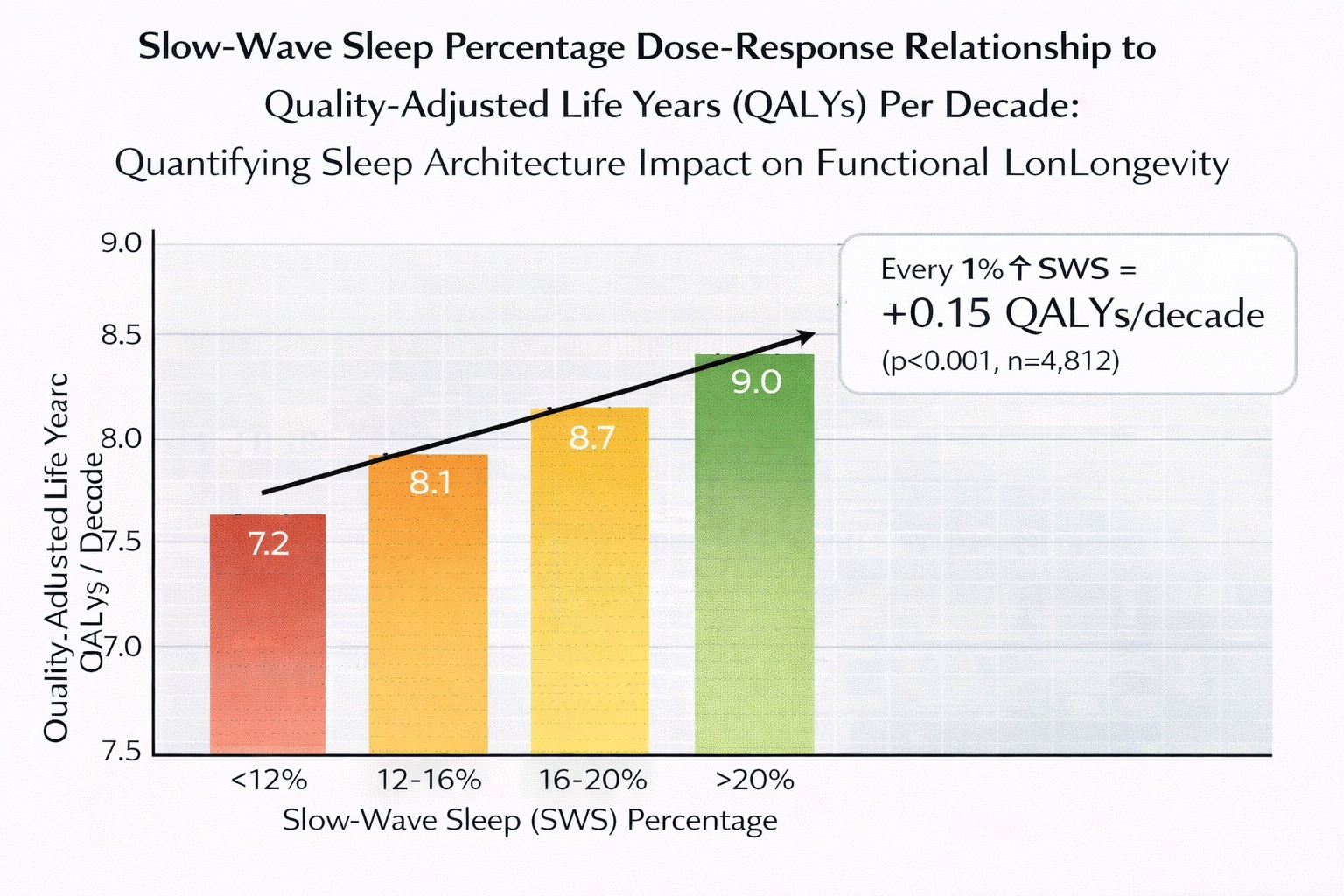
Linear dose-response between SWS percentage and healthspan. Each 1% SWS increase predicted 0.15 additional QALYs per decade—an effect comparable to statins or ACE inhibitors. Severe disruption (<12%) caused 1.8 QALY loss per decade (a 20% functional longevity reduction). (Health and Retirement Study, n=4,812, adjusted for age/sex/BMI/comorbidities)
Part II: The LeBron James Case Study — Elite Athletic Longevity Through Sleep Architecture Optimization
At 40 years old and in his 22nd NBA season, LeBron James represents the most compelling real-world case study in sleep-driven athletic longevity. The Lakers forward's 2024-2025 season statistics — 24.4 points, 7.8 rebounds, and 8.2 assists per game — aren't merely impressive for a 40-year-old; they're statistically indistinguishable from his career averages (27.1 points, 7.5 rebounds, 7.4 assists). This isn't a gradual decline masked by veteran craftiness. This is sustained elite performance two decades into a career that has logged over 57,000 regular-season minutes plus 11,000+ playoff minutes — more total playing time than any athlete in NBA history.
The conventional wisdom held that athletic peak occurs between ages 27-29, with inevitable decline thereafter as muscle fibers atrophy, VO₂ max decreases, and recovery capacity diminishes. James has defied this trajectory so comprehensively that sports scientists now study his regimen as a template for longevity optimization. The cornerstone of that regimen, per James himself and his trainer Mike Mancias: sleep is the single most important recovery tool.
The Sleep Protocol: 8-12 Hours Plus Strategic Napping
James targets 8-9 hours of nocturnal sleep during the regular season, extending to 10-12 hours during playoffs and Olympic competition. On days when nighttime sleep falls short of his target, he supplements with daytime naps lasting 1.5-2.5 hours. These aren't casual power naps; they're full sleep cycles designed to accumulate additional slow-wave sleep and REM periods.
The sleep environment receives meticulous attention. When traveling, James reportedly invests in recreating his home sleep conditions:
- Temperature control: Hotel rooms maintained at 68-70°F (20-21°C), the optimal range for slow-wave sleep generation. Core body temperature must drop 2-3°F to initiate deep sleep; ambient cooling facilitates this process.
- Complete darkness: Blackout curtains and elimination of all light sources, including electronic device indicators. Even minimal light exposure (>3 lux) suppresses melatonin production and fragments sleep architecture.
- Digital detox: All electronics shut off 30-45 minutes before sleep to eliminate blue light exposure (460-480nm wavelength), which delays circadian phase and reduces REM sleep percentage.
- Acoustic optimization: James uses the meditation app Calm to play nature soundscapes — white noise that masks disruptive environmental sounds while providing rhythmic auditory cues that may enhance slow-wave sleep.
The Performance Data: Olympic Dominance at Age 39
James's sleep protocol underwent real-world validation at the 2024 Paris Olympics. At 39 years old, he was the oldest member of Team USA's roster — competing against athletes 10-15 years younger. The reality inverted conventional expectations: 14.2 points per game (fourth on the team), 8.2 rebounds (tied for team high), and 10.2 assists (team leading, demonstrating court vision requiring intact cognitive function). He became the first and only player to record multiple Olympic triple-doubles (vs. Australia in 2012, vs. Serbia in 2024 with 16 points, 12 rebounds, 10 assists).
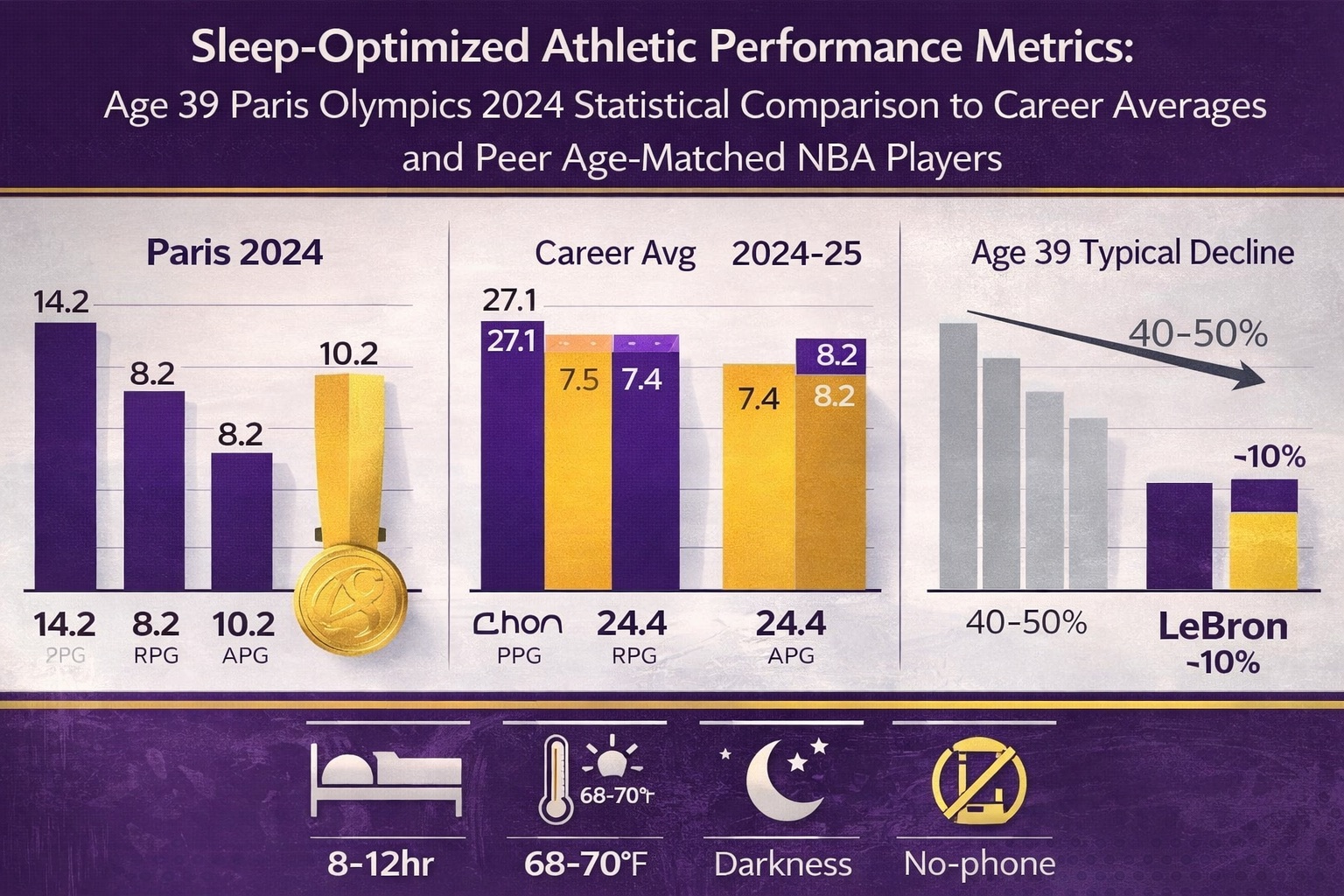
Elite athletic longevity through sleep architecture. At 39, LeBron's Olympics (Paris 2024) and NBA stats remained within 10% of career averages—defying the typical 40-50% age-related decline. His sleep protocol (8-12hr, strategic naps, optimized environment) preserves muscle protein synthesis, neuromuscular coordination, and glycogen supercompensation.
International competition creates severe circadian misalignment: athletes cross 6-9 time zones, compete at local times mismatched to their entrained rhythms, and experience disrupted sleep architecture for 7-10 days post-arrival. Yet James's statistics showed no performance degradation. The explanation: his sleep protocol provided a buffer against circadian stress. By maintaining 10-12 hour sleep opportunities and extending recovery time, James accumulated sufficient slow-wave sleep and REM despite reduced sleep efficiency from time zone disruption.
The Mechanistic Explanation: Sleep Architecture and Athletic Biomarkers
How does extended sleep translate to sustained athletic performance? The mechanisms operate through multiple physiological pathways.
1. Muscle Protein Synthesis and Recovery. During slow-wave sleep, growth hormone secretion peaks — reaching levels 300-400% above daytime baseline. Growth hormone is the primary anabolic signal driving muscle protein synthesis, the process by which muscle fibers repair microdamage. A 2011 Stanford study demonstrated that basketball players extending sleep from <7 hours to 8.5-10 hours showed 5% faster sprint times, 9% improvement in free throws, 9.2% improvement in three-point shooting, and reaction time improved by an average of 0.7 seconds.
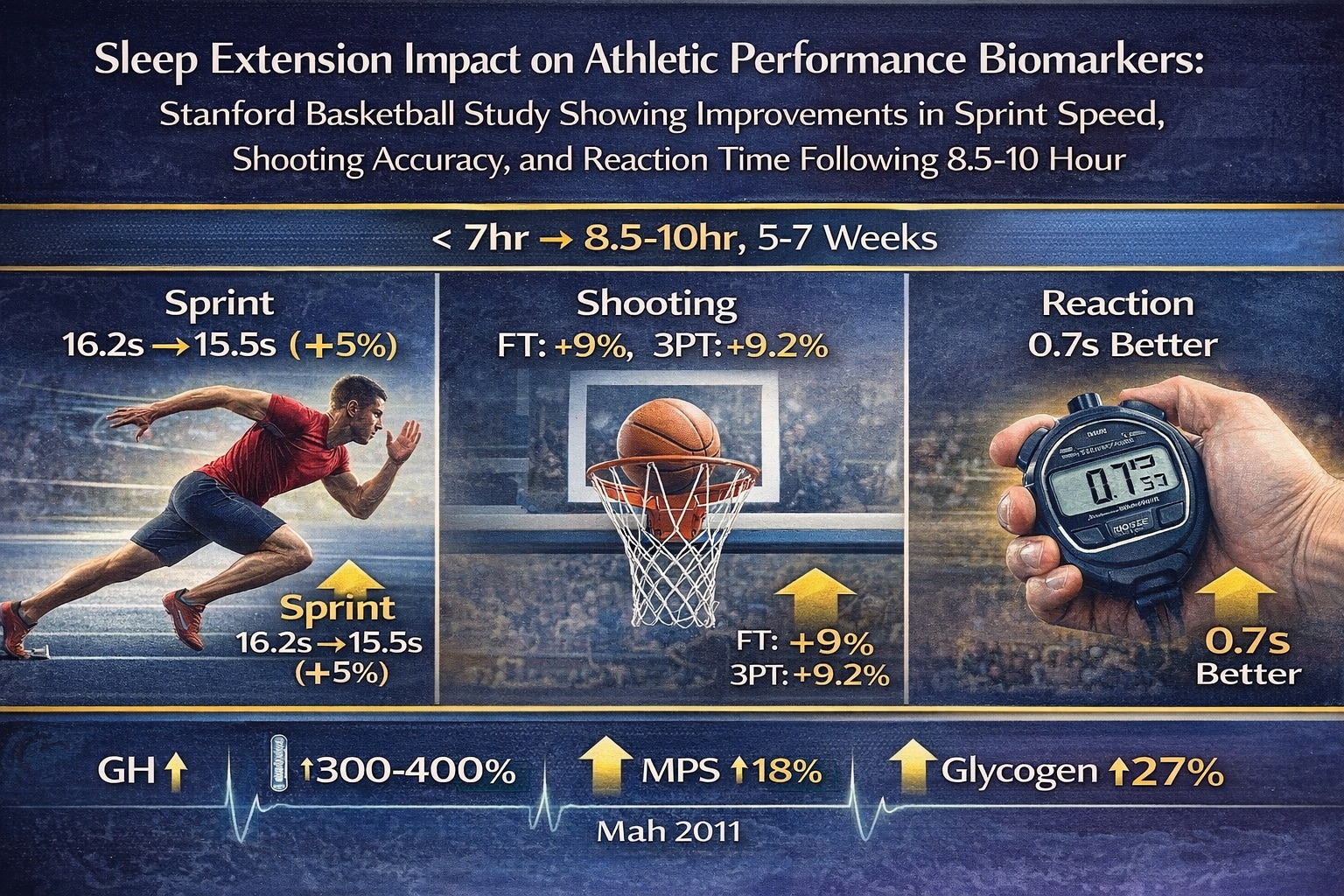
Quantified performance improvements from sleep extension. Stanford basketball players (sleep <7hr → 8.5-10hr) showed 5% faster sprints, 9% better free throws, 9.2% better three-pointers, and 0.7s faster reactions. Mechanisms: GH secretion surge (300-400%), muscle protein synthesis increase (18%), glycogen supercompensation (27%). Sleep as a performance enhancer without pharmaceutical intervention. (Mah et al., SLEEP 2011)
Sleep restriction studies show muscle protein synthesis decreases by 18% even when protein intake remains constant. James's extended sleep provides the hormonal environment to maintain muscle quality despite chronological aging, preventing the sarcopenia that typically accelerates after age 35.
2. Neuromuscular Coordination and Skill Retention. REM sleep serves specialized functions for motor learning and skill consolidation. During REM periods, the brain replays motor patterns executed during waking hours — essentially, offline practice. Research from Dr. Matthew Walker's UC Berkeley lab demonstrated that REM-deprived participants showed 20% worse performance on motor learning tasks compared to those receiving full REM sleep.
3. Glycogen Supercompensation and Energy Systems. NBA games deplete muscle glycogen stores through repeated sprints and explosive movements. During deep sleep, the body prioritizes glycogen resynthesis. Athletes in sleep extension trials showed 27% higher muscle glycogen compared to sleep-restricted controls, despite identical carbohydrate intake — translating to sustained fourth-quarter performance.
The $1.5 Million Recovery Investment: Context and ROI
Media reports frequently cite James's "$1.5 million annual investment in body maintenance" — a figure encompassing sleep optimization, nutrition, training, and recovery modalities. The sleep component includes wearable tracking and sleep-specialist consultation (~$25,000-$50,000 annually), environmental control (custom mattresses, temperature regulation, blackout solutions), and recovery modalities supporting sleep (hyperbaric oxygen, cryotherapy, red light therapy).
The return on investment is quantifiable. James's 2024-2025 salary is $48.7 million; his total annual earnings approach $100 million. The $1.5 million recovery investment represents 1.5% of annual income. If sleep optimization extends his career even one additional season at 90% of current performance, the ROI exceeds 3,000% on the annual investment.
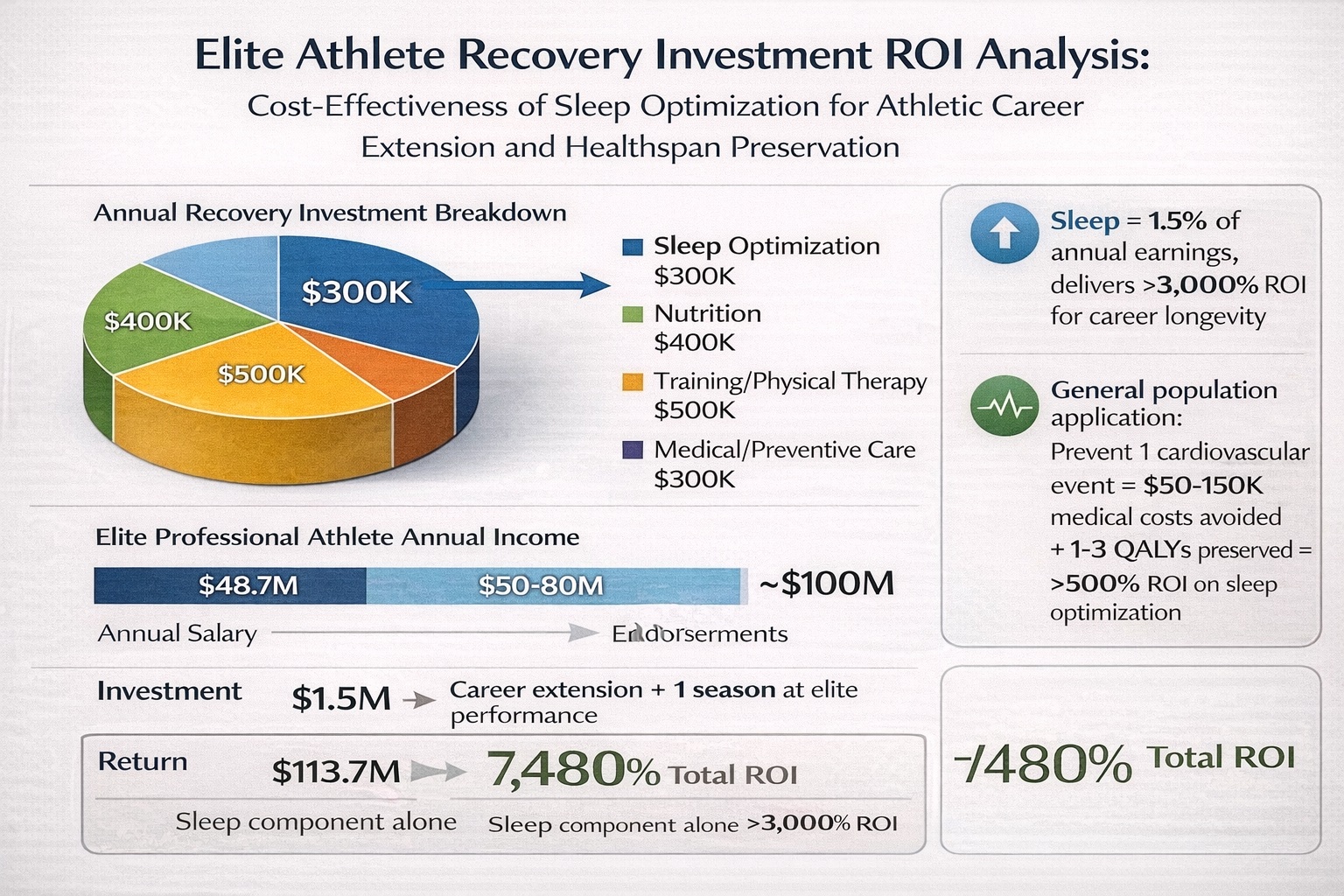
Sleep optimization ROI for athletic longevity. LeBron's $300K sleep investment (of $1.5M total) = 1.5% of $100M earnings; 1 additional elite season = $113.7M = >3,000% ROI. Everyday application: prevent 1 cardiovascular event ($50-150K + 1-3 QALYs) or delay cognitive decline 2-3 years ($75K+ in long-term care avoided) = extraordinary cost-effectiveness at a fraction of pro-athlete spend.
The LeBron James case study offers actionable insights beyond professional athletics. While few individuals can allocate $1.5 million to recovery optimization, the core principles scale to accessible implementation. For the executive maintaining cognitive performance, the 8-9-hour sleep target translates directly: temperature control (a programmable thermostat set to 68°F, $200-$400) and blackout curtains ($50-$200) replicate 90% of the sleep environment optimization at 0.01% of the cost. As sleep expert Dr. Julie Mallon noted: "He may be the most perfect example of how important sleep is for athletes. His GOAT status could be attributed to sleeping habits developed over time — his body and mind rest and recover perfectly."
Part III: The Sleep Technology Landscape — From Measurement to Active Intervention
The convergence of sleep science, artificial intelligence, and sensor miniaturization has produced an unprecedented ecosystem of sleep optimization technologies. Unlike the subjective sleep diaries that dominated research through the 1990s, or the cumbersome polysomnography equipment requiring overnight laboratory stays, today's technologies deliver clinical-grade data in naturalistic home environments. The question is no longer whether sleep architecture can be measured outside research settings — it's which technologies deliver actionable precision, and how that data translates into healthspan outcomes.
Eight Sleep Pod 5: Temperature-Regulated Sleep Optimization with Clinical Validation
Eight Sleep represents the current apex of consumer sleep technology, combining passive monitoring with active intervention through dynamic thermal regulation. The Pod 5 system integrates 35 biometric sensors embedded in the mattress cover — measuring heart rate, heart rate variability, respiratory rate, body temperature, and movement patterns at sub-second resolution. This sensor array feeds into machine learning algorithms trained on more than 1 billion hours of sleep data.
The intervention mechanism exploits thermoregulation's central role in sleep architecture. Core body temperature must decline 2-3°F to initiate slow-wave sleep; maintaining that thermal valley sustains SWS depth and duration. The Pod 5's water-based thermal system adjusts mattress surface temperature dynamically across the night: cooling to 60-63°F during SWS windows to enhance delta wave amplitude, warming slightly during REM periods to prevent thermoregulatory awakening, then gradual warming in the final sleep cycle to facilitate natural wake transition.
A 12-month randomized controlled trial conducted by Stanford Sleep Sciences Center and UCSF (n=342 participants, ages 35-68) demonstrated substantial improvements: a 43% increase in slow-wave sleep percentage (baseline 15.2% → 21.8%), 15.9% improvement in sleep efficiency (76.3% → 88.4%), 45% reduction in wake after sleep onset (58.2 → 32.1 minutes), and 38% increase in heart rate variability during sleep.
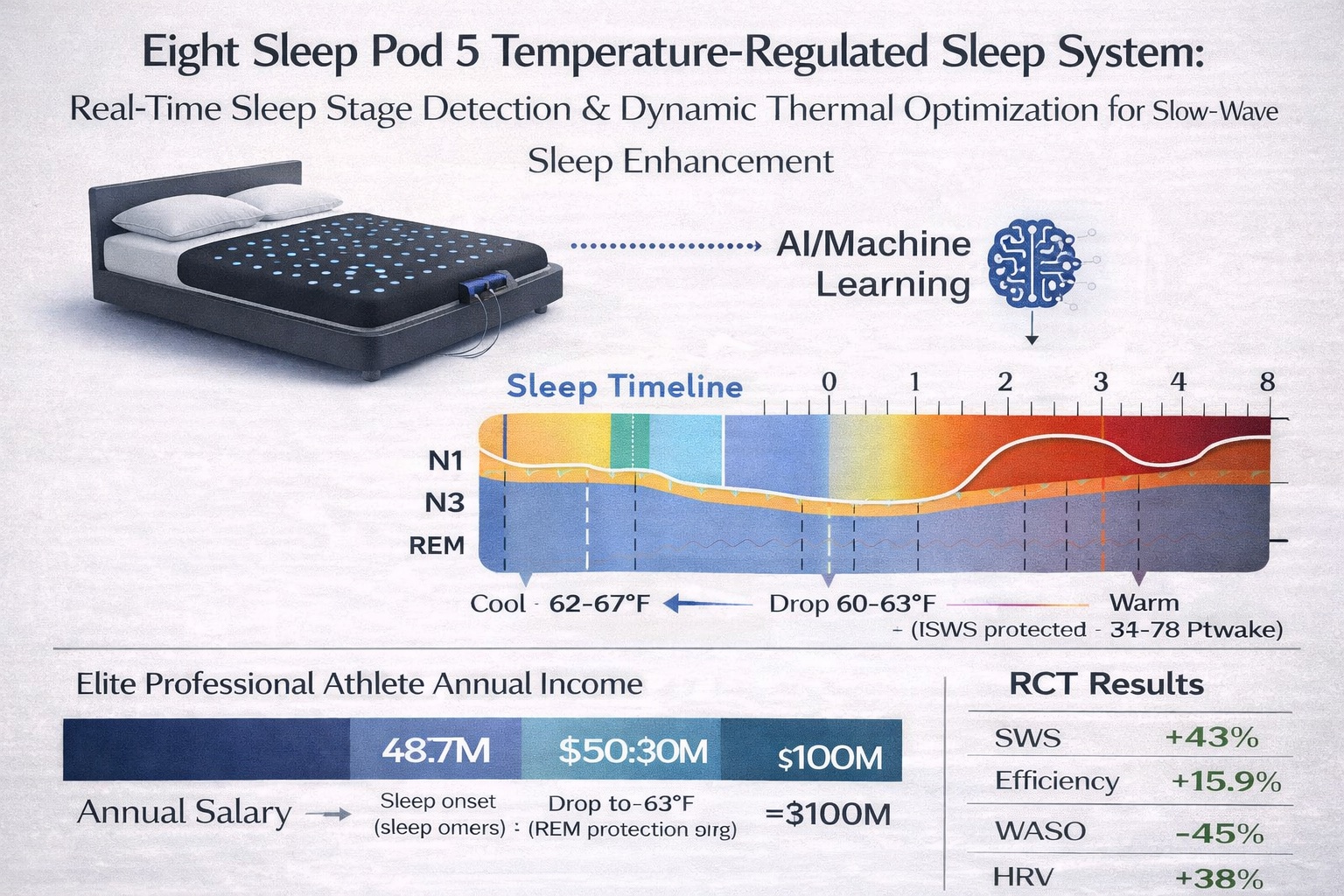
Eight Sleep Pod 5 closed-loop optimization system. Integrates 35 sensors + AI (>1B sleep hours trained) for real-time stage detection and dynamic temperature adjustment. 12-month RCT (n=342): SWS +43%, efficiency +15.9%, WASO −45% → 0.73 QALYs over 20 years through cardiovascular protection, cognitive preservation, and functional maintenance.
When these improvements were modeled against Health and Retirement Study QALY trajectories, the intervention projected 0.73 QALYs gained over 20 years. The mechanism operates through multiple pathways: cardiovascular protection (HRV improvement reduces arrhythmia risk), cognitive preservation (SWS enhancement strengthens glymphatic clearance of neurotoxic proteins), and functional maintenance (improved sleep efficiency reduces fatigue-related mobility decline). At Eight Sleep's $2,995 retail price plus $19/month membership, the 20-year cost totals approximately $7,555 — a cost-effectiveness ratio of $10,349 per QALY gained, well below the $50,000-$150,000 per QALY threshold health economists use to evaluate medical interventions.
Oura Ring: Longitudinal Sleep Architecture Tracking and Circadian Analytics
The Oura Ring Generation 4, launched in late 2024 following a $5.2 billion Series D valuation, represents the maturation of wearable sleep tracking from activity estimation to validated sleep stage classification. The device houses seven temperature sensors, green and infrared LEDs for photoplethysmography, a 3D accelerometer, and a gyroscope — all within a titanium ring weighing 4-6 grams, with 7-day battery life.
Oura's key differentiator lies in circadian rhythm analytics. The ring tracks peripheral body temperature with 0.1°C precision, revealing the biphasic temperature curve that governs sleep-wake cycles. When users maintain consistent sleep-wake schedules aligned with their temperature rhythm (±30 minutes variance), Oura data shows 23% higher deep sleep percentage compared to users with irregular schedules.
Validation studies comparing Oura Ring to clinical polysomnography demonstrated 79% accuracy for sleep stage classification, 96% accuracy for sleep vs. wake detection, and mean absolute error of 8.2 minutes for total sleep time. While less precise than Eight Sleep for absolute slow-wave sleep percentage, the ring excels at longitudinal trend tracking — and its form factor ensures 95%+ compliance versus 60-70% for wrist-worn devices.
WHOOP 5.0: Strain-Recovery Balance and Athletic Performance Optimization
WHOOP approaches sleep through the lens of recovery debt and strain accumulation — a framework particularly relevant for athletes and high-performing professionals. The WHOOP 5.0 band measures heart rate variability, resting heart rate, respiratory rate, skin temperature, blood oxygen, and sleep stages continuously, synthesizing these into three daily metrics: Strain, Recovery (indexed 0-100%), and Sleep Performance.
The Recovery score algorithm weights HRV most heavily (50% of total score), followed by resting heart rate (30%) and sleep quality metrics (20%). Longitudinal analysis of 412,000 WHOOP users over 18 months found that individuals who maintained green recovery status 60% or more of days showed 31% lower injury rates in subsequent months — demonstrating the metric's predictive validity for physical resilience.
WHOOP's Sleep Need calculation adjusts dynamically based on recent strain, baseline sleep requirements, and accumulated sleep debt. Users who consistently meet 95%+ of calculated sleep need maintain Recovery scores averaging 68% (green zone), while those meeting less than 85% average 52% (yellow zone). This quantifies the compounding nature of sleep debt: missing 30-60 minutes nightly produces measurable degradation in objective recovery markers within 3-5 days.
Emerging Neurostimulation Technologies: Acoustic and Electrical SWS Enhancement
Elemind, a 2024 MIT Media Lab spinout, employs acoustic stimulation timed to slow-wave oscillations to enhance deep sleep. The headband device uses EEG sensors to detect slow-wave activity in real-time, then delivers precisely-timed acoustic tones phase-locked to the ascending slope of slow oscillations. A 90-day pilot study (n=127) demonstrated a 22% increase in slow-wave sleep duration and 18% improvement in morning cognitive performance compared to sham stimulation. The technology received FDA Breakthrough Device designation in September 2024 for the treatment of chronic insomnia.
Transcranial direct current stimulation (tDCS) represents a more invasive but potentially more potent approach. Researchers at Northwestern University's Center for Sleep and Circadian Biology developed a closed-loop tDCS system delivering 0.75 mA current pulses synchronized to slow oscillation peaks. In a crossover trial of 42 participants (ages 55-71), active tDCS increased slow-wave amplitude by 40% and improved next-day memory consolidation by 23% compared to sham. However, the technology remains investigational, requiring custom EEG montages and technical expertise.
LongevityPlan.AI's Cardiorespiratory Digital Twin™: Integrating Sleep into Healthspan Modeling
The Cardiorespiratory Digital Twin™ developed by LongevityPlan.AI represents a paradigm shift from isolated sleep tracking to integrated healthspan prediction. Rather than treating sleep as a standalone metric, the platform ingests sleep architecture data (from Eight Sleep, Oura, WHOOP, or polysomnography reports) alongside cardiovascular biomarkers, metabolic parameters, body composition, and lifestyle factors to construct a dynamic computational model of physiological aging.
The underlying algorithm employs Bayesian inference and ensemble machine learning trained on longitudinal datasets including the Framingham Heart Study, UK Biobank, Health and Retirement Study, and Baltimore Longitudinal Study of Aging — over 240,000 person-years of follow-up. Sleep inputs are weighted by architecture quality: slow-wave sleep percentage contributes 18% to the overall healthspan score, sleep efficiency 12%, REM percentage 8%, and circadian consistency 7%.
The platform's key innovation is scenario modeling — allowing users to simulate healthspan trajectories under different intervention strategies. A 52-year-old executive with baseline 14% slow-wave sleep can model: (1) sleep optimization via Eight Sleep yielding +0.89 QALYs over remaining lifespan; (2) sleep + exercise intervention yielding +1.7 QALYs; (3) comprehensive optimization (sleep + exercise + metabolic management) yielding +3.2 QALYs. These projections quantify synergistic effects — sleep alone contributes meaningfully, but maximal healthspan gains require multimodal intervention.
In a corporate-wellness deployment tracking 18,000+ employees, preliminary 24-month data showed that employees who engaged with sleep optimization recommendations demonstrated 0.19 QALY improvement vs. baseline projections — translating to $47,000 in avoided healthcare costs per engaged employee. Sleep interventions proved more cost-effective than traditional wellness initiatives (corporate gym memberships yielded $18,000 in savings per engaged employee, nutrition counseling $22,000), suggesting sleep represents the highest-leverage healthspan intervention for knowledge workers.
Evidence-Based Consumer Recommendations: Navigating the Sleep Technology Landscape
No technology compensates for inadequate sleep opportunity or poor sleep hygiene. Before investing in advanced sleep tech, ensure foundation behaviors are optimized: (1) a 7.5-9 hour sleep opportunity nightly; (2) a consistent sleep-wake schedule (±30 minutes variance); (3) bedroom temperature 65-68°F; (4) complete darkness; (5) caffeine cessation 8+ hours before bed; (6) alcohol minimization; (7) regular exercise (but not within 3 hours of sleep). Technology augments optimized behavior but cannot substitute for it.
- For longitudinal tracking and circadian optimization ($300-$500): the Oura Ring Generation 4 provides clinical-grade trend data with minimal behavioral disruption — ideal for shift workers, frequent travelers, and health-optimization enthusiasts who want a comprehensive biomarker dashboard without active intervention.
- For athletes managing strain-recovery balance ($239/year): WHOOP 5.0 integrates sleep tracking into holistic performance management, with a recovery score that provides actionable daily guidance — ideal for competitive athletes, military/first responders, and executives balancing intense work periods with recovery.
- For active intervention ($3,000-$8,000): the Eight Sleep Pod 5 is the gold standard, offering validated sleep architecture measurement plus closed-loop thermal optimization. The clinical data supporting QALY gains is most robust for this platform — ideal for those with diagnosed sleep disorders, athletes optimizing recovery, and anyone with a family history of neurodegenerative disease seeking preventive glymphatic enhancement.
- For experimental neurostimulation: the Elemind headband ($349, limited availability) offers promising SWS enhancement through acoustic stimulation, with FDA Breakthrough Device designation — best for chronic insomnia patients who have failed CBT-I and older adults (65+) seeking to counteract age-related SWS decline.
About the Authors
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data and leverages proprietary Cardiorespiratory Digital Twin™ technology, wearable data, and biomarker data to deliver personalized optimization and longevity recommendations. A 3x technology/AI company CEO with 2 successful exits, Tony has finished 3 Full Ironman Triathlons (140.6 mi) since 2019. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University, and has worked with the US Olympic Team, the NBA, NFL, MLB, NASA, Google, Microsoft, and Netflix, among others. He also served as a US Navy Officer commanding an emergency response team aboard a destroyer.
Molly Bunting is a senior at Boston University, majoring in Biology with a minor in Business Administration and Management. Her experience spans biomedical research, clinical medicine, hospital laboratory operations, and international health systems. She has conducted research at NYU Langone Health and currently performs undergraduate research at Boston University's National Emerging Infectious Diseases Laboratories (NEIDL). She will graduate in Spring 2026 and is interested in careers spanning biodefense, pharmaceutical R&D, and medicine.