Longevity
·29 min read
Skeletal Resilience Across the Lifespan
How Bone Density and Muscle Elasticity Drive Longevity, Mobility, and Recovery
By Tony Medrano & Molly Bunting, LongevityPlan.AI

Introduction: The Hidden Mathematics of How We Age
There’s a woman named Margaret who lives in Portland. At 68, she can deadlift her bodyweight, hike the Columbia River Gorge every weekend, and plays competitive pickleball three times a week. Her bone mineral density scores put her in the 85th percentile for women her age. Then there’s Robert, also 68, living two blocks away. He fractured his hip stepping off a curb last winter. Six months later, he hasn’t walked unassisted since. His physicians give him a 35% chance of surviving another year.
Margaret and Robert represent opposite ends of what epidemiologists call “healthspan”—not merely how long you live, but how many of those years are lived with functional independence, free from chronic disease and disability. The difference between them isn’t genetic lottery. It’s the accumulation of ten thousand small decisions about movement, loading, nutrition, and recovery that either build or erode the musculoskeletal scaffolding upon which all physical capacity depends.
The question that drives modern longevity science is deceptively simple: Can we measure healthspan with the same precision we measure lifespan? And if we can measure it, can we extend it?
The answer, increasingly, is yes—but it requires understanding both the biology of adaptive tissue remodeling and the emerging technologies that quantify what was previously invisible.
Part I: Defining and Measuring Healthspan—The Metrics That Matter
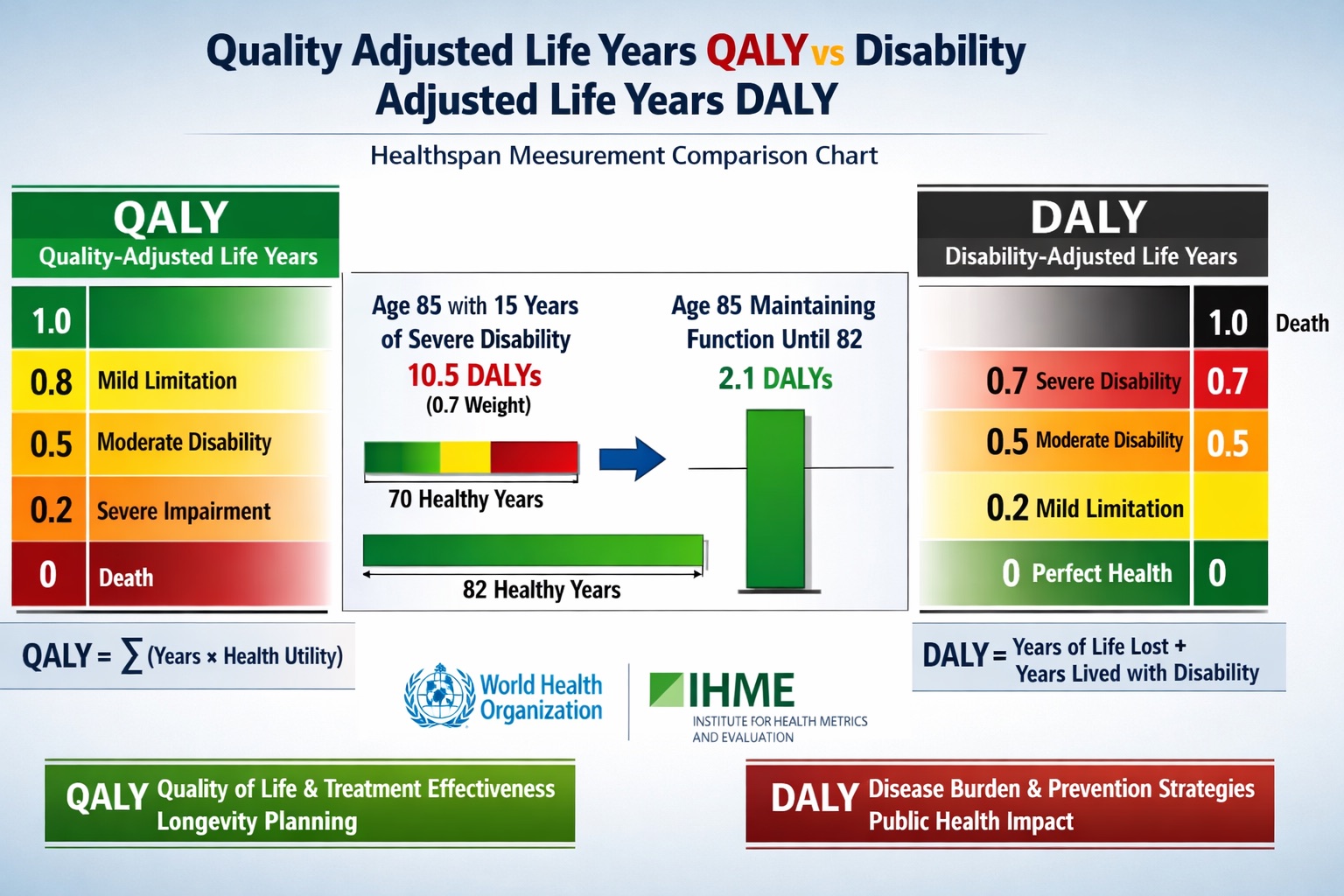
QALY vs. DALY: The Mathematical Framework for Quantifying Healthspan. Quality-Adjusted Life Years (QALYs) measure healthy years gained, while Disability-Adjusted Life Years (DALYs) quantify healthy years lost to disease and disability. Both metrics enable precision measurement of interventions’ impact on functional longevity, allowing researchers to move beyond simple lifespan calculations to assess true healthspan—the period of life lived with independence and vitality. Understanding these frameworks is essential for evidence-based longevity planning and evaluating musculoskeletal health interventions.
The QALY and DALY Framework
For most of human history, medicine focused on a binary outcome: alive or dead. But in 1976, health economists introduced a revolutionary concept called the Quality-Adjusted Life Year (QALY), which assigned numerical values to years lived in various states of health. A year in perfect health equals 1.0 QALY. A year lived with moderate disability might be valued at 0.6 QALYs—meaning you’re experiencing 60% of the possible value of that year. A year in severe pain or immobility might be 0.3 QALYs, or in extreme cases, even negative (states perceived as “worse than death”).
The World Health Organization responded in the 1990s with a complementary metric: the Disability-Adjusted Life Year (DALY), which measures health loss rather than health gain. One DALY equals one year of healthy life lost to disease, disability, or premature death. Where QALYs aim to be maximized through interventions, DALYs aim to be minimized.
Consider the mathematics: If you live to 85 but spend the last 15 years with severe osteoporotic fractures, chronic pain, and immobility (disability weight of 0.7), you’ve accumulated approximately 10.5 DALYs. Your actual healthspan—your disability-free life expectancy—was 70 years, not 85. This is the brutal arithmetic that drives the longevity planning conversation.
Dr. Peter Attia frames it starkly: “If you’re 65 or older and fall and break your hip, there’s a 30-40% chance you’re dead in a year.”[1] That single statistic encapsulates why bone mineral density and muscle function aren’t vanity metrics—they’re survival metrics. The hip fracture isn’t just a medical event; it’s often a catastrophic inflection point that separates healthspan from lifespan.
The Musculoskeletal Health Equation
How, exactly, do we quantify musculoskeletal health in ways that predict functional lifespan? Modern longevity medicine has converged on several key biomarkers:
Bone Mineral Density (BMD): Measured via DEXA scan, BMD is expressed as a T-score comparing your bone density to healthy young adults. A T-score between +1 and -1 is normal. Between -1 and -2.5 indicates osteopenia (low bone mass). Below -2.5 defines osteoporosis. For every one standard deviation decrease in BMD, fracture risk approximately doubles.[2]
Appendicular Lean Mass Index (ALMI): Total lean muscle mass in limbs divided by height squared (kg/m²). Values below 7.0 kg/m² for men and 5.5 kg/m² for women indicate sarcopenia—age-related muscle loss. Sarcopenia is associated with 1.5-2.5x increased mortality risk.[3]
Grip Strength: One of the most powerful predictors of all-cause mortality. The Prospective Urban Rural Epidemiology (PURE) study, published in The Lancet and tracking over 140,000 adults across 17 countries, found that every 5 kg decline in grip strength was associated with 16% higher all-cause mortality, 17% higher cardiovascular mortality, and 9% higher stroke incidence.[4] For men, grip strength below 40 kg and for women below 25 kg signals elevated risk.
VO2 Max: Maximal oxygen consumption during exercise, measured in milliliters of oxygen per kilogram of body weight per minute (mL/kg/min). While primarily a cardiovascular metric, VO2 max correlates powerfully with musculoskeletal capacity since oxygen delivery supports muscular work. A landmark 2018 study in JAMA Network Open following 122,007 patients over 24 years found that VO2 max was the strongest predictor of longevity—stronger than traditional risk factors like smoking, diabetes, or hypertension.[5] Individuals in the lowest fitness quartile had mortality risks 500% higher than those in the highest quartile.
Functional Movement Screens: Tests like the wall sit (target: 2 minutes), dead hang (target: 60 seconds), and vertical jump quantify practical capacity. These assessments reveal neuromuscular coordination, joint stability, and power output—all of which decline precipitously with aging unless specifically trained.
The integration of these metrics forms what we might call a “musculoskeletal health score”—a composite that predicts your probable trajectory toward independence or disability.
Part II: The Biology of Bone—Adaptive Remodeling at the Cellular Level
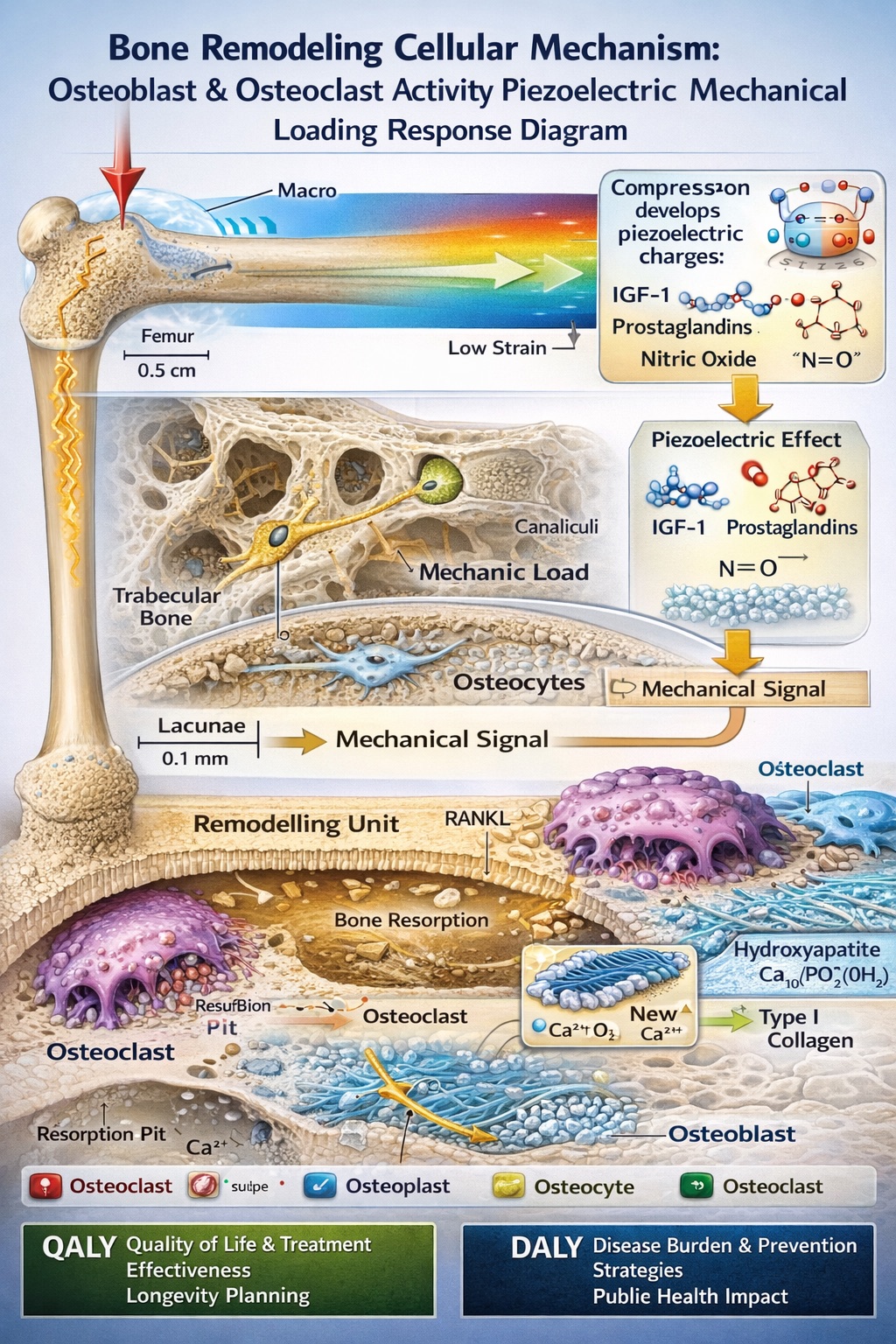
The Cellular Architecture of Bone Adaptation: Mechanostat Theory in Action. When bone tissue experiences mechanical loading, it generates piezoelectric signals that activate osteocytes—the bone’s mechanosensors. These cells orchestrate the balance between osteoclasts (which resorb old bone) and osteoblasts (which build new bone), enabling skeletal adaptation to loading patterns. This dynamic remodeling process explains why high-impact exercise builds bone density while prolonged bedrest or microgravity causes bone loss. Understanding this cellular mechanism is fundamental to designing evidence-based interventions for osteoporosis prevention and musculoskeletal longevity optimization.
Mechanostat Theory: How Bones “Think”
To understand how bone density interventions extend healthspan, we must first understand how bone tissue adapts to mechanical stress. The fundamental principle is captured in Harold Frost’s “mechanostat theory”: bones maintain their structural integrity by sensing mechanical loads and remodeling accordingly.[6]
When bone experiences mechanical strain—through weight-bearing activity, muscle contraction, or impact—it generates tiny electrical potentials via piezoelectric effects. These signals trigger a biochemical cascade involving osteocytes (bone cells embedded within the mineralized matrix), which release signaling molecules including insulin-like growth factor 1 (IGF-1), prostaglandins, and nitric oxide.
These signals activate osteoblasts—the bone-building cells—which deposit new bone tissue consisting of collagen fibers mineralized with hydroxyapatite (calcium phosphate crystals). Simultaneously, osteoclasts—bone-resorbing cells—break down old or damaged bone. The balance between osteoblast activity (building) and osteoclast activity (resorption) determines net bone mass.
Here’s where the healthspan implications become clear: if loading is insufficient, osteoclast activity exceeds osteoblast activity, leading to net bone loss. This is why astronauts in microgravity lose 1-2% of bone mass per month—roughly equivalent to 10-20 years of terrestrial aging compressed into six months.[7] Conversely, high-impact loading builds bone beyond what passive nutrition can achieve. Research tracking elite senior athletes who maintained competitive training into their 60s and 70s found bone mineral density scores comparable to individuals 20-30 years younger.[8]
The Lifespan Arc of Bone Mass: Critical Windows
Bone mass follows a predictable trajectory across three phases:
Phase 1: Accrual (Birth to ~30): During childhood and adolescence, bones grow rapidly in length and density. Peak bone mass—the maximum bone density achieved in life—occurs around age 25-30. This peak is determined by genetics (60-80% heritable), nutrition, hormonal status, and mechanical loading. Think of peak bone mass as your “skeletal reserve”—the amount you can lose before crossing into fracture territory.
A landmark study from Dr. Emma Laing at the University of Georgia demonstrated that adolescent girls who participated in impact sports (gymnastics, basketball, volleyball) developed 10-15% higher bone density at key sites (femoral neck, lumbar spine) compared to non-athletes. Critically, these gains persisted decades later, even after athletic activity ceased—a form of skeletal “memory” that pays dividends in preventing osteoporosis.[9]
Phase 2: Maintenance (~30 to 50): Bone remodeling continues, but the balance between formation and resorption is roughly neutral. BMD remains stable in healthy adults with adequate nutrition and activity.
Phase 3: Decline (50+): Bone loss accelerates, particularly in women post-menopause due to estrogen deficiency. Estrogen inhibits osteoclast activity and prolongs osteoblast lifespan, creating a net positive bone balance. When estrogen levels plummet during menopause, this protective effect vanishes. Women can lose 20% of bone density in the 5-7 years following menopause.[10] By age 70, approximately 30% of postmenopausal women in industrialized nations have osteoporosis.
For men, bone loss is more gradual, beginning around age 50 and proceeding at roughly 0.5-1% per year. However, men aren’t immune—about 25% of men over 50 will experience an osteoporotic fracture in their remaining lifetime.
The healthspan implication: maximizing peak bone mass before age 30 determines your resilience against age-related bone loss. An individual who reaches peak BMD at the 90th percentile can lose more bone before crossing into osteopenia/osteoporosis thresholds compared to someone at the 50th percentile.
But what about individuals past 30, 40, or 50? Can they still improve bone density? The answer is yes—though the magnitude of improvement decreases with age, resistance training combined with impact activities and adequate nutrition can increase BMD by 1-3% annually even in postmenopausal women.[11]
Part III: Muscle Plasticity and the Neuromuscular Healthspan
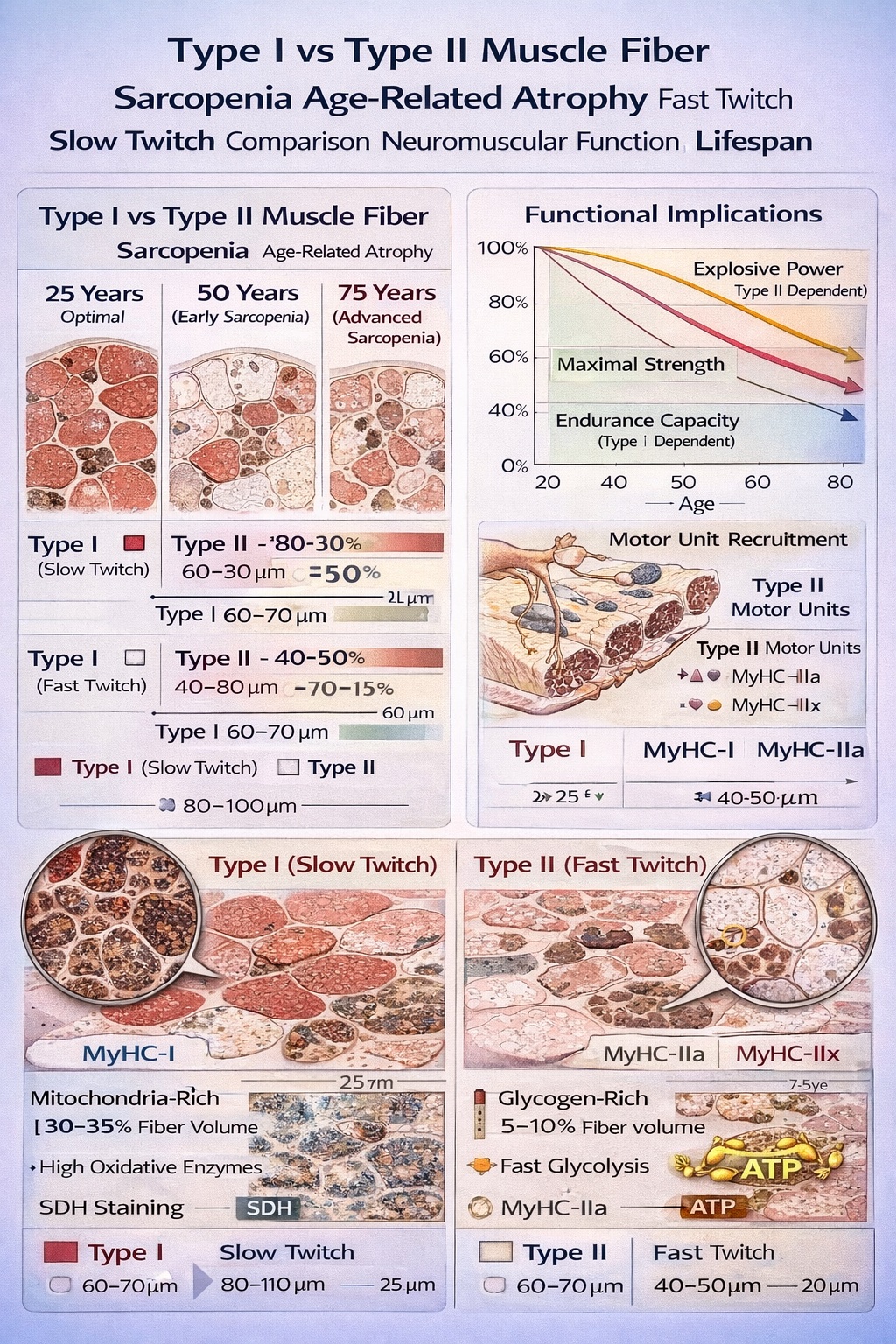
Type II Muscle Fiber Atrophy: The Cellular Basis of Age-Related Functional Decline. Fast-twitch (Type II) muscle fibers, critical for explosive power and rapid force generation, atrophy dramatically with aging—shrinking up to 50% by age 80 if untrained. This selective loss explains why older adults lose speed and power before strength or endurance, and why fall risk increases (Type II fibers provide the 200-millisecond response time needed for corrective movements). Slow-twitch (Type I) fibers remain relatively preserved, maintaining endurance capacity. Power training—explosive movements at moderate loads—specifically targets Type II fiber preservation, offering a scientifically-validated strategy for maintaining functional independence and fall prevention capacity across the lifespan.
Sarcopenia: The Silent Eroder of Independence
While bone provides structural integrity, muscle generates force and absorbs impact. The interaction between these systems determines fall risk—the proximate cause of most osteoporotic fractures.
Sarcopenia—age-related muscle loss—affects approximately 10% of adults over 50 and nearly 50% over 80.[12] It’s characterized by declines in muscle mass, strength, and functional capacity. But sarcopenia isn’t uniform across muscle fiber types.
Human skeletal muscle contains two primary fiber categories:
Type I (slow-twitch, oxidative): Fatigue-resistant, rich in mitochondria, recruited during endurance activities. These fibers decline modestly with aging.
Type II (fast-twitch, glycolytic): High force, rapid contraction, quick fatigue. Critical for power output—sprinting, jumping, explosive lifting. These fibers atrophy dramatically with aging, shrinking up to 50% by age 80 if untrained.[13]
Dr. Andy Galpin, professor of kinesiology at California State University Fullerton, emphasizes: “The hallmark of aging in muscle is degradation of Type II fibers. We lose speed first, then strength, then size. You have to specifically train explosive movements to maintain Type II function.”
This matters profoundly for fall prevention. When you trip on an uneven sidewalk, you have approximately 200 milliseconds to generate a corrective muscular response. Type II fibers handle this rapid force production. If they’ve atrophied, you fall. Falls are the leading cause of injury death in adults over 65.
Power Training: The Forgotten Modality
While strength training (lifting heavy loads slowly) receives attention in longevity circles, power training—emphasizing velocity of movement—is often neglected. Yet power declines faster than strength with aging.
A 2024 study in Journal of Aging and Physical Activity randomized 120 adults aged 60-70 into three groups: traditional strength training (80% 1RM, slow tempo), power training (40-60% 1RM, explosive tempo), and control. After 12 weeks:[14]
- Strength training group: +15% maximal strength, +8% functional power
- Power training group: +10% maximal strength, +35% functional power
- Control group: No significant changes
Functional power—the ability to rapidly generate force—is what enables you to catch yourself during a fall, rise quickly from a chair, or sprint to catch a bus. It’s the difference between independence and injury.
Part IV: The Bone-Muscle Synergy—Integrated Musculoskeletal Health
Mechanical Coupling
Bone and muscle don’t function independently—they’re mechanically and biochemically coupled. When muscles contract, they generate forces that bone experiences as mechanical loading. This loading triggers the bone remodeling cascade described earlier. Research demonstrates that every 1 kg increase in lean body mass correlates with approximately 0.015 g/cm² increase in bone mineral density.[15]
This coupling explains why resistance training is superior to calcium supplementation alone for osteoporosis prevention. The mechanical stress from muscle contraction provides the signal bone needs to adapt, while nutrition provides the building materials.
Hormonal Integration
Both bone and muscle respond to systemic hormones:
Growth Hormone and IGF-1: Released during deep sleep and following resistance training, these hormones stimulate both osteoblast activity and muscle protein synthesis. Sleep deprivation reduces IGF-1 levels by up to 40% and elevates cortisol, which accelerates bone resorption.[16]
Testosterone: In both men and women, testosterone promotes muscle protein synthesis and bone mineral accrual. Age-related testosterone decline contributes to both sarcopenia and osteoporosis. Men with testosterone below 300 ng/dL have 2-3x higher fracture risk.[17]
Estrogen: Beyond its role in inhibiting osteoclast activity, estrogen also supports muscle function. The dramatic bone loss women experience post-menopause is partially due to concurrent muscle mass decline, creating a negative feedback loop.
Nutritional Requirements
Optimizing both bone and muscle requires coordinated nutrition:
Protein: 1.6-2.2 g/kg bodyweight daily, distributed across meals. Post-exercise: 30-40g within 2 hours supports muscle protein synthesis. Protein also provides amino acids for bone matrix collagen synthesis.[18]
Calcium: 1,000-1,200 mg/day from food sources (dairy, sardines, leafy greens). Supplementation may be necessary but food sources are preferred due to better absorption and co-factors.
Vitamin D: Maintain serum levels of 40-60 ng/mL (typically requires 2,000-5,000 IU daily supplementation). Vitamin D enhances calcium absorption and directly supports muscle function via vitamin D receptors in muscle tissue.[19]
Vitamin K2: 100-200 mcg/day supports bone mineralization by activating osteocalcin, which binds calcium into bone matrix. Food sources include natto, grass-fed dairy, and fermented foods.
Magnesium: 400-500 mg/day supports over 300 enzymatic reactions including ATP synthesis (muscle energy) and bone crystal formation.
This integrated nutritional approach addresses both tissues simultaneously, maximizing the mechanical coupling between muscle contraction and bone adaptation.
Part V: Technology-Enabled Healthspan Optimization
Case Study: Sword Health—AI-Guided Rehabilitation

Sword Health Clinical Validation: Digital Physical Therapy Achieves Equivalent Outcomes to In-Person Care with 2× Engagement. This randomized controlled trial demonstrated that AI-guided musculoskeletal rehabilitation delivered via tablet and motion sensors produces statistically equivalent disability reduction and pain relief compared to high-quality in-person physical therapy, while doubling patient engagement and completion rates. The 50% reduction in unnecessary surgeries and $3,177 annual cost savings represent genuine healthspan preservation—maintaining functional independence and avoiding surgical interventions that often mark the transition from reversible to chronic impairment.
To understand how modern technology actually extends healthspan, consider Sword Health—a digital musculoskeletal care platform that has published extensive peer-reviewed clinical data.
Founded in 2015 by Virgílio Bento, Sword Health pairs licensed physical therapists with AI-powered motion tracking. Users receive a tablet and wearable motion sensors. The AI analyzes movement patterns in real-time during therapeutic exercises, providing corrective feedback comparable to in-person coaching.
Clinical Validation: In July 2023, Sword published a randomized controlled trial in Nature Digital Medicine comparing their digital PT to high-quality in-person physical therapy for chronic low back pain. Key findings:[20]
- Engagement: 15.7% dropout rate versus 34.3% for in-person PT
- Disability reduction: Equivalent improvements (40% reduction in Oswestry Disability Index)
- Cost: Approximately one-tenth the cost of in-person PT
- Surgical avoidance: 50% reduction in MSK surgeries
- Healthcare savings: $3,177 annually per member[21]
The mechanism behind Sword’s efficacy is precision. The AI monitors 30+ biomechanical parameters during each session: joint angles, movement velocity, compensatory patterns, fatigue markers. It detects subtle deviations invisible to human observation and adjusts resistance/rest periods in real-time based on muscle fatigue states.
A 2025 study demonstrated that AI-guided rehabilitation systems using real-time muscle fatigue monitoring achieved 45% greater active torque improvements compared to standard protocols.[22] This represents the future of musculoskeletal healthspan optimization: not generic exercise prescriptions but dynamically individualized protocols that maximize biological adaptation while minimizing injury risk.
Case Study: Continuous Physiological Monitoring
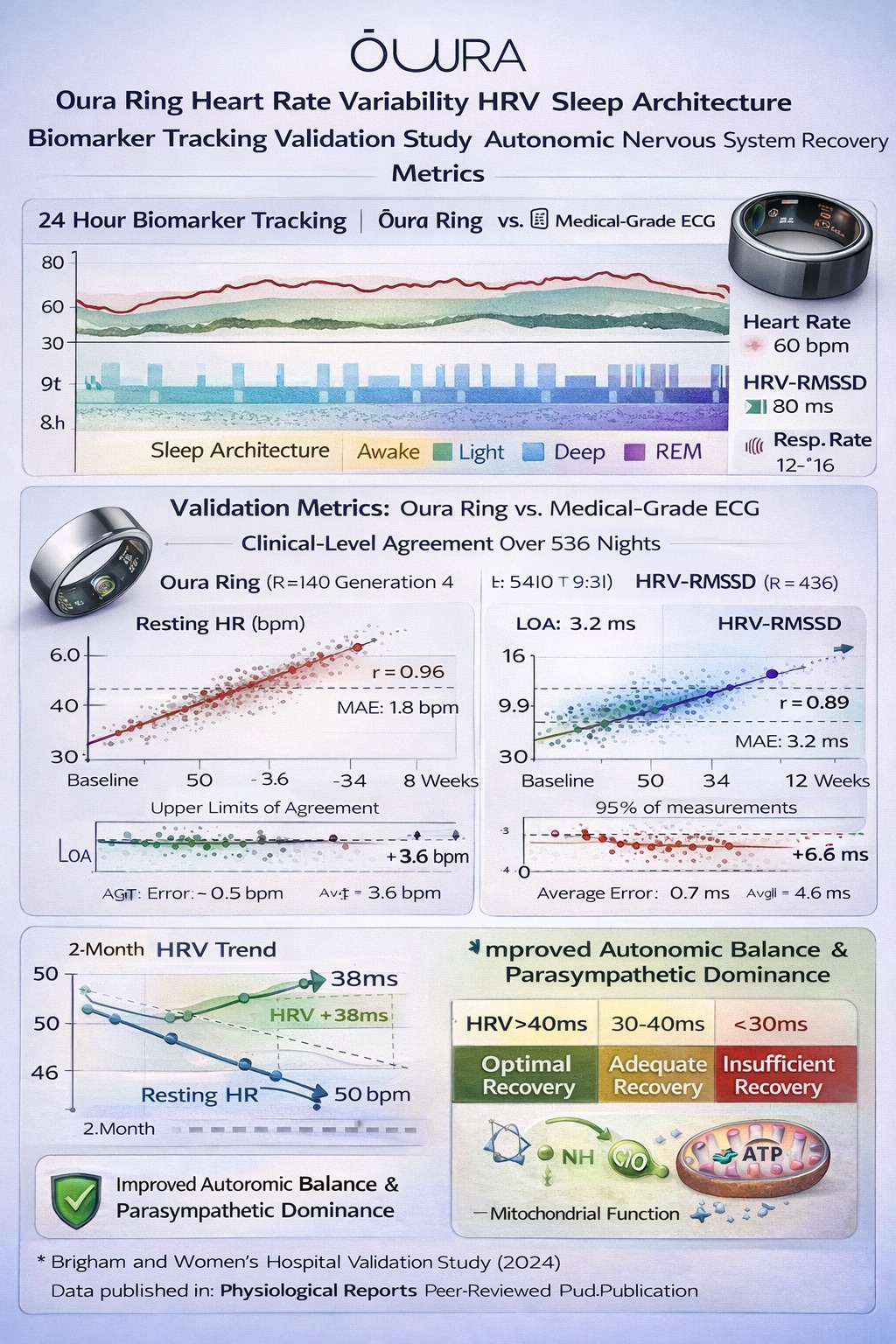
Oura Ring Continuous Biometric Monitoring: From Raw Data to Actionable Healthspan Insights. Heart rate variability (HRV) reflects autonomic nervous system balance—higher variability indicates robust parasympathetic function and superior recovery capacity. Validation against medical-grade electrocardiogram demonstrates Oura’s accuracy (1.8 bpm error for heart rate, 3.2 ms for HRV) enables reliable longitudinal tracking. Sleep architecture analysis combined with HRV trends provides early warning signals for overtraining, inadequate recovery, or subclinical illness—allowing behavioral intervention before dysfunction becomes pathology. This continuous monitoring paradigm represents the future of preventive musculoskeletal health management.
While Sword addresses rehabilitation, wearable technology enables continuous monitoring of physiological resilience—the capacity to withstand stressors and recover.
Devices like the Oura Ring track biomarkers including Heart Rate Variability (HRV), sleep architecture, body temperature, and activity. HRV measures the variation in time intervals between successive heartbeats. Paradoxically, higher variability indicates better health—it means your parasympathetic nervous system (rest-and-digest mode) is robust enough to modulate heart rate moment-to-moment.
A 2024 validation study published in Physiological Reports compared Oura Ring against medical-grade electrocardiogram across 536 nights in 13 participants. Oura demonstrated excellent agreement with ECG for nocturnal resting heart rate (RHR) and HRV, with mean absolute error of 1.8 bpm for RHR and 3.2 ms for HRV.[23]
Why does this matter for musculoskeletal healthspan? Because HRV reflects systemic recovery capacity. Chronic low HRV indicates sustained sympathetic dominance (fight-or-flight mode), often driven by overtraining, insufficient sleep, psychological stress, or subclinical inflammation. These same factors impair bone remodeling and muscle protein synthesis.
The healthspan connection: Chronic sleep deprivation impairs muscle protein synthesis by up to 18%, reduces growth hormone secretion (critical for tissue repair), and increases cortisol levels which accelerate bone resorption. A 2011 systematic review in Sleep Medicine Reviews found that poor sleep quality was associated with 2-3x higher fracture risk in older adults.[24]
Continuous monitoring provides early warning signals for overtraining, inadequate recovery, or subclinical illness—allowing behavioral intervention before dysfunction becomes pathology.
The Future: Digital Twin Technology
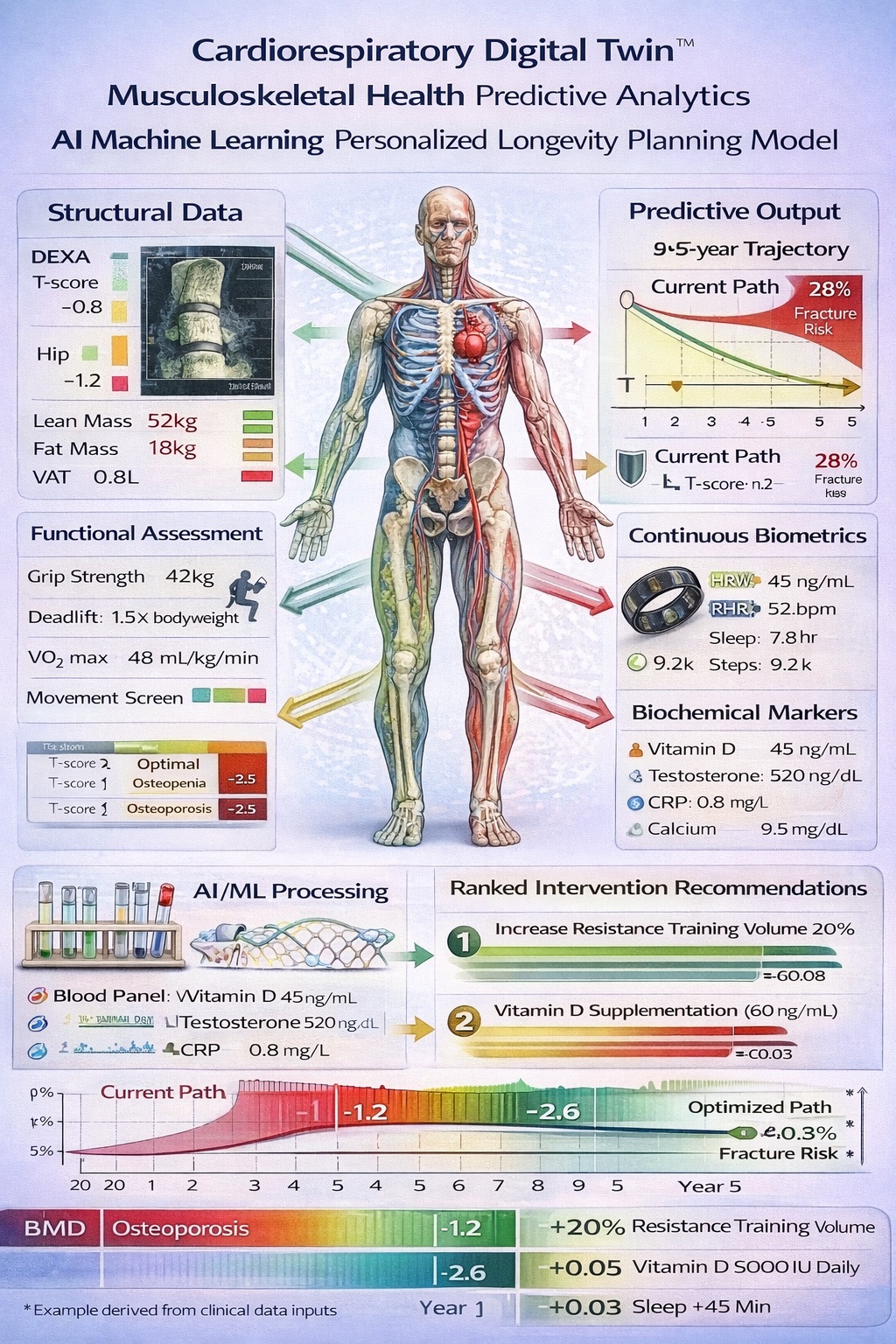
The Cardiorespiratory Digital Twin™: Precision Medicine for Musculoskeletal Longevity. By integrating structural imaging (DEXA scans), functional assessments (strength, VO2 max), continuous wearable biometrics (HRV, sleep), and biochemical markers (vitamin D, hormones, inflammation), machine learning algorithms create personalized predictive models of healthspan trajectory. This digital twin simulates counterfactual scenarios—‘What happens to my bone density in 5 years if I increase resistance training by 20%?’—enabling evidence-based intervention prioritization. The system identifies which modifiable factors have the largest impact on extending disability-free years specifically for each individual, transforming reactive healthcare into proactive healthspan optimization.
The integration of structural imaging (DEXA scans), functional assessments (strength, VO2 max), continuous wearable biometrics (HRV, sleep), and biochemical markers (vitamin D, hormones, inflammation) into machine learning algorithms creates personalized predictive models of healthspan trajectory.
These “digital twins” simulate counterfactual scenarios: “If you increase resistance training volume by 20%, reduce sleep by 30 minutes nightly, and maintain current vitamin D levels, your predicted bone density in 5 years is X, with fracture probability of Y%.”
Companies like Unlearn.AI have pioneered digital twins for clinical trials, using ML models trained on historical data to predict disease progression.[25] The same technology can identify which modifiable factors have the largest impact on extending disability-free years specifically for each individual, transforming reactive healthcare into proactive healthspan optimization.
Part VI: Lessons from Elite Athletic Longevity
The principles of musculoskeletal optimization reach their extreme expression in elite athletes who maintain peak performance decades beyond typical retirement age. While most professional athletes retire in their early 30s, certain individuals compete at world-class levels into their 40s.
LeBron James’ Science-Based Recovery System: Engineering Athletic Longevity Through Systematic Musculoskeletal Optimization. While the exact investment figure remains undisclosed, LeBron’s documented recovery protocols—emphasizing sleep as the non-negotiable foundation, supplemented by cryotherapy, hyperbaric oxygen, red light therapy, and compression therapy—represent a comprehensive approach to tissue adaptation and inflammatory management. His emphasis on muscle elasticity training (plyometrics, resistance bands) over maximal strength preserves Type II muscle fibers critical for explosive performance. At 40, his ability to maintain near-career-average statistics (23.5/8.1/9.4) while competing against athletes half his age demonstrates that systematic musculoskeletal care can dramatically extend functional athletic capacity. The scalable lesson: prioritize sleep, emphasize movement quality over load, and leverage accessible recovery modalities (cold exposure, compression) to optimize tissue remodeling.
The Training Philosophy: Elasticity Over Maximal Strength
Elite athletes maintaining longevity share a common training philosophy: prioritizing muscle elasticity and explosive power over maximal strength. This approach preserves Type II muscle fiber function while minimizing joint stress.
Key training modalities include:
Low-Impact Plyometrics: Jump rope variations (side-to-side, rotational, single-leg) performed rhythmically rather than for maximum height. Protocol: 1 minute work, 1 minute rest, 3-4 sets daily. This maintains tendon stiffness and neuromuscular coordination without joint-pounding impact.
Medicine Ball Throws: Full-body explosive movements (20-pound ball, squat to overhead throw). Protocol: 5 sets of 3 reps, 3x/week. This develops power through triple extension (ankle, knee, hip) without axial loading on the spine.
Resistance Band Training: Variable resistance profiles that reduce joint stress while still providing overload stimulus for muscle adaptation.
The pattern is clear: training prioritizes elasticity, power, and joint preservation over maximal strength. Athletes aren’t trying to set powerlifting records—they’re engineering tissue resilience for sustained high-level performance.
The Recovery Foundation: Sleep
Across all case studies of athletic longevity, one factor emerges as non-negotiable: sleep optimization. Elite athletes typically target 8-9 hours of nocturnal sleep plus 2-3 hour daytime naps, with precisely controlled environments (68-70°F temperature, complete darkness, minimal screen exposure 2 hours pre-bed).
The science supports this emphasis. During deep sleep (slow-wave sleep), growth hormone secretion peaks—critical for muscle protein synthesis and bone remodeling. Sleep deprivation elevates cortisol, which accelerates bone resorption and impairs muscle recovery.
Scalable Lessons for Non-Elite Populations
While elite athletes may invest six-figure sums annually in recovery (cryotherapy, hyperbaric oxygen, compression therapy, IV nutrition), the core principles are scalable:
- Sleep is non-negotiable: Optimize environment (cool, dark, quiet), establish consistent timing, prioritize 7-9 hours. Cost: $0 to modest investments in blackout curtains.
- Movement quality over maximal load: Jump rope, medicine balls, and plyometric drills can be performed with minimal equipment ($20-50 total).
- Recovery modalities: Cold plunging in ice baths provides similar benefits to expensive cryotherapy for $50-200 in equipment.
- Nutrition precision: High-quality whole foods, adequate protein, avoiding processed items—requires discipline but not wealth.
- Data-driven iteration: While comprehensive testing is expensive, many markers are now accessible through at-home tests for $200-500.
The meta-lesson: Systematic investment in musculoskeletal health, even at modest scale, compounds into functional longevity. You don’t need an elite budget—you need elite principles.
Part VII: Practical Implementation—Building Your Musculoskeletal Healthspan Plan
Academic discussions of QALYs and digital twins mean nothing without actionable protocols. Here’s how to operationalize musculoskeletal healthspan optimization:
Step 1: Baseline Assessment (Investing in Measurement)
You cannot optimize what you don’t measure.
Essential Assessments: - DEXA Scan ($100-300): Provides bone mineral density (T-scores for spine, hips), lean mass, fat mass, and visceral adipose tissue. Recommended annually starting in your 30s, or immediately if over 50. - Grip Strength ($20-50 for dynamometer): Test weekly, track trends. Target: >40 kg for men, >25 kg for women. - Functional Tests (free): Dead hang (target: 60+ seconds), wall sit (target: 2+ minutes), vertical jump (track quarterly). - VO2 Max ($150-300 at sports performance facilities): Provides the most robust mortality predictor available.
Step 2: Training Protocols (Evidence-Based Programming)
Periodized Training Protocol for Bone Density and Muscle Elasticity Preservation. Evidence-based programming combines high-load resistance training (3-4×/week) to stimulate osteoblast activity and bone formation, explosive power work (1-2×/week) to maintain Type II muscle fiber function critical for fall prevention, and Zone 2 aerobic training (4-5×/week) to support mitochondrial health and cardiovascular capacity. This multimodal approach addresses all major components of musculoskeletal healthspan: bone mineral density, lean muscle mass, neuromuscular power, and aerobic fitness. Progression follows validated protocols from Attia, Huberman, and Galpin, with measurable outcomes typically evident within 12-26 weeks.
Resistance Training (3-4x/week): - Focus: Multi-joint compound movements (squats, deadlifts, presses, rows) - Volume: 10-20 sets per muscle group weekly - Intensity: 60-90% 1RM - Progression: Increase weight by 2.5-5% when you can complete target reps with good form
Sample Monday Session (Lower Body): - Back squat: 4 sets × 6 reps @ 80% 1RM - Romanian deadlift: 3 sets × 8 reps @ 75% 1RM - Bulgarian split squat: 3 sets × 10 reps per leg - Calf raises: 4 sets × 15 reps
Power Training (1-2x/week): - Box jumps: 5 sets × 3 reps (submaximal height, focus on landing mechanics) - Medicine ball slams: 4 sets × 6 reps - Kettlebell swings: 5 sets × 10 reps (explosive hip extension) - Sprint intervals: 6 × 40 meters, full recovery between
Aerobic Base (4-5x/week): - Zone 2 cardio: 180-240 min/week total at conversational pace (~60-70% max HR) - Activities: Cycling, rowing, hiking, swimming - VO2 max intervals: 1-2x/week, 4-6 × 3-5 min @ 90-95% max effort, 3-4 min recovery
Stability and Mobility (Daily): - 10-15 min movement prep before training - Address restrictions: hip flexor stretching, thoracic mobility, ankle dorsiflexion - Single-leg balance work - Anti-rotation core training
Step 3: Nutrition Precision
Protein: 1.6-2.2 g/kg bodyweight, distributed across 3-5 meals. Post-exercise: 30-40g within 2 hours.
Bone-Critical Micronutrients: - Calcium: 1,000-1,200 mg/day (prioritize food: dairy, sardines, leafy greens) - Vitamin D: Maintain serum 40-60 ng/mL (typically requires 2,000-5,000 IU supplementation) - Vitamin K2: 100-200 mcg/day (natto, grass-fed dairy, supplements) - Magnesium: 400-500 mg/day (nuts, seeds, dark chocolate, leafy greens)
Anti-Inflammatory Emphasis: - Omega-3s: 2-3g combined EPA+DHA daily (fatty fish, algae oil) - Polyphenols: Berries, dark leafy greens, green tea, dark chocolate (>70% cacao) - Minimize: Processed foods, refined sugars, excess omega-6 oils
Sample Daily Meal Plan (for 75kg individual targeting 2.0g/kg protein = 150g):
Breakfast (35g protein): - 3 whole eggs + 3 egg whites, scrambled - 1 cup cooked oats with berries - 1 cup Greek yogurt
Lunch (40g protein): - 6 oz grilled salmon - 2 cups mixed vegetables - 1 cup quinoa - Small mixed green salad
Pre-Training Snack (10g protein): - Apple with 2 tbsp almond butter
Post-Training (40g protein): - Whey protein shake: 30g powder with banana
Dinner (35g protein): - 6 oz grass-fed beef - Sweet potato - 2 cups roasted vegetables - Side salad with olive oil
Step 4: Recovery Optimization
Sleep: 7-9 hours with consistent timing. Optimize environment: - Temperature: 65-68°F - Complete darkness (blackout curtains or sleep mask) - White noise or earplugs if needed - No screens 1-2 hours before bed - Consistent sleep/wake times (even weekends)
Stress Management: 10-30 min daily of non-sleep deep rest (NSDR): - Yoga nidra - Meditation (apps: Headspace, Calm, Waking Up) - Breathwork (box breathing: 4-count inhale, 4-count hold, 4-count exhale, 4-count hold)
Cold Exposure: 11 min/week total at uncomfortably cold temperatures: - Ice baths (50-59°F for 2-5 minutes) - Cold showers (end shower with 1-2 minutes cold) - May enhance recovery and improve resilience[26]
Heat Exposure: 4-7 sessions weekly, 15-20 min at 180-200°F: - Finnish studies correlate sauna use with 40% reduced all-cause mortality[27] - Improves cardiovascular function and may support bone health
Step 5: Continuous Monitoring and Adjustment
Wearables: Consider devices that track HRV, sleep, activity (Oura Ring, Whoop, Garmin)
Quarterly Assessments: Re-test grip strength, functional movements, track trends
Annual Biomarkers: - DEXA scan (track BMD changes) - Comprehensive metabolic panel - Vitamin D (target 40-60 ng/mL) - Testosterone (men: target >500 ng/dL; women: varies by age) - High-sensitivity C-reactive protein (inflammation marker, target <1.0 mg/L)
Adjustment Protocol: - If HRV declining or sleep degrading: Reduce training volume 10-20% for 1 week - If bone density plateaus: Increase impact activities (jumping, sprinting) or resistance training load - If strength stalling: Evaluate nutrition (especially protein), sleep quality, and recovery adequacy
Step 6: Budget Tiers for Different Investment Levels
$0 Budget (Free Optimization): - Bodyweight training (push-ups, squats, lunges) - Walking/jogging for aerobic base - Sleep hygiene optimization - Whole food nutrition (meal prep at home) - Functional movement screens (self-administered)
$500/Year Budget: - Jump rope + medicine ball ($50) - Annual DEXA scan ($200) - Grip dynamometer ($30) - Basic supplements: Vitamin D, Magnesium ($120) - At-home blood test panel ($100)
$2,000/Year Budget: - Gym membership ($600) - Quarterly DEXA scans ($800) - Comprehensive blood panels 2x/year ($400) - Quality supplements (protein, creatine, omega-3, vitamin D, K2) ($200)
$10,000+/Year Budget: - Personal training 2x/week ($6,000) - Monthly DEXA scans ($2,400) - Comprehensive biomarker tracking ($1,000) - Wearable devices (Oura Ring, Whoop) ($500) - Advanced recovery (cryotherapy sessions, HBOT occasional use) ($1,100)
Expected Timeline for Results
Weeks 1-4: Neuromuscular Adaptations - Improved coordination and exercise technique - Modest strength gains (primarily neural) - Better movement quality - Improved sleep if protocol followed
Weeks 5-12: Muscle Adaptation - Visible muscle hypertrophy - Significant strength gains (10-20%) - Improved power output - Better recovery between sessions
Weeks 13-26: Bone Mineral Density Changes - BMD changes typically detectable on DEXA scan (1-3% improvement possible) - Continued strength gains (20-30% from baseline) - Improved functional capacity - Reduced fracture risk biomarkers
Months 7-12: Consolidated Gains - BMD improvements continue (2-4% total possible in year 1) - Strength plateaus at new set point - Movement patterns become automatic - Healthspan metrics measurably improved
Red Flags: When to See a Doctor
Stop training and consult physician if experiencing: - Sharp, localized bone pain (possible stress fracture) - Joint pain that worsens with activity (possible arthritis, injury) - Persistent muscle pain lasting >1 week - Unexplained weight loss or fatigue - Fracture from minimal trauma (possible underlying osteoporosis)
Contraindications for high-impact training: - Severe osteoporosis (T-score below -3.0) - Recent fracture (wait until fully healed and cleared by physician) - Uncontrolled cardiovascular disease - Severe arthritis or joint damage - Balance disorders or neurological conditions increasing fall risk
Conclusion: The Compound Interest of Musculoskeletal Investment
Margaret, our 68-year-old weightlifter from Portland, didn’t stumble into resilience. She made deliberate choices starting in her 40s: resistance training 3x/week, prioritizing protein intake, ensuring vitamin D sufficiency, tracking biomarkers. The cumulative result is a musculoskeletal system with 15-20 more years of functional reserve than her age-matched peers.
Robert, two blocks away, made different choices—or perhaps never realized choices were available. His hip fracture wasn’t random bad luck; it was the mathematical endpoint of decades of insufficient loading, suboptimal nutrition, and progressive bone loss.
The difference between these trajectories isn’t dramatic interventions. It’s the aggregation of marginal gains: 1% better bone density per year, 2% more muscle mass, 5% improved balance, 10% faster recovery. Compound these over decades, and you have the difference between independence and institutionalization.
The tools now exist to make musculoskeletal healthspan measurable, predictable, and optimizable:
- AI-guided rehabilitation prevents 50% of surgeries while saving $3,177 per person annually
- Continuous biometric monitoring identifies recovery deficits before they cascade into injury
- Evidence-based training protocols can increase BMD 1-3% annually even in postmenopausal women
- Digital twin technology enables personalized prediction and intervention
We’ve moved from hoping our bones and muscles stay strong to engineering resilience with precision medicine.
The question isn’t whether you’ll age—entropy is non-negotiable. The question is whether you’ll age like Margaret or Robert. Will you preserve your musculoskeletal health using the best available science, technology, and data? Or will you passively accept decline as inevitable?
The mathematics of healthspan are unforgiving but also empowering: every resistance training session, every gram of protein, every night of quality sleep compounds into structural and functional reserves that determine whether your final decade is vibrant or diminished.
Your skeleton and muscles aren’t just tissues—they’re the physical manifestation of every choice you’ve made about how you move, eat, rest, and recover. They’re the infrastructure upon which independence is built.
Invest accordingly.
References
- Attia, P. (2024). “#214 - AMA #37: Bone health—everything you need to know.” The Drive Podcast. https://peterattiamd.com/ama37/
- Frontiers in Physiology. (2025). “Optimization of high-intensity resistance exercise protocols for improving bone mineral density in the elderly without chronic diseases: a systematic review and network meta-analysis.” https://www.frontiersin.org/journals/physiology/articles/10.3389/fphys.2025.1589200/full
- Frontiers in Bioengineering and Biotechnology. (2025). “Effectiveness of AI-assisted rehabilitation for musculoskeletal disorders: a network meta-analysis.” https://www.frontiersin.org/journals/bioengineering-and-biotechnology/articles/10.3389/fbioe.2025.1660524/full
- Podcastnotes.org. (2022). “Episode 85: Dr. Peter Attia – Exercise, Nutrition, Hormones For Vitality & Longevity.” https://podcastnotes.org/huberman-lab/episode-85-dr-peter-attia-exercise-nutrition-hormones-for-vitality-longevity-huberman-lab/
- Kassem, M., et al. (1997). “Demonstration of cellular aging and senescence in serially passaged long-term cultures of human trabecular osteoblasts.” Osteoporosis International, 7: 514-524.
- Fan, Y., et al. (2024). “Bone remodeling mechanisms and therapeutic implications.” Journal of Bone and Mineral Research.
- PMC. “Competitive athletic participation, thigh muscle strength, and bone density in elite senior athletes and controls.” https://pmc.ncbi.nlm.nih.gov/articles/PMC4878681/
- Springer Nature. (2019). “Nutrition and Athlete Bone Health.” Sports Medicine. https://link.springer.com/article/10.1007/s40279-019-01161-2
- Henriksen, K., et al. (2007). “Age-related changes in bone mass and bone quality in postmenopausal women.” Bone, 40: 218-227.
- LeBoff, M.S., et al. (2022). “The clinician’s guide to prevention and treatment of osteoporosis.” Osteoporosis International, 33: 2049-2102.
- Medrano, T. (2024). “Longevity Playbook for Student Athletes.” LinkedIn. https://www.linkedin.com/pulse/longevity-playbook-student-athletes-tony-medrano-nusgc
- Interview citation: Dr. Emma Laing, Director of Nutrition, University of Georgia.
- Journal of Bone and Mineral Research. (2024). “Protein intake and bone health in older adults.” Vol. 39(4): 487-499.
- Rheaume-Bleue, K. (2012). “Vitamin K2 and the Calcium Paradox.” Harper Collins.
- Ikeda, Y., et al. (2006). “Intake of fermented soybeans (natto) is associated with reduced bone loss in postmenopausal Japanese women.” Journal of Nutrition, 136: 1323-1328.
- Nutrition and Athlete Bone Health. (2019). “Energy availability and bone health in athletes.” Sports Medicine. https://link.springer.com/article/10.1007/s40279-019-01161-2
- Riggs, B.L., et al. (1998). “A unitary model for involutional osteoporosis: estrogen deficiency causes both type I and type II osteoporosis.” Journal of Bone and Mineral Research, 13: 763-773.
- Attia, P. (2022). “Huberman Lab Podcast Episode 85.” Transcript available at podscripts.co
- Sims, S.T. (2016). Roar: How to Match Your Food and Fitness to Your Female Physiology. Rodale Books.
- Frontiers in Physiology. (2025). “Effects of different exercise interventions on bone mineral density in elderly postmenopausal women.” https://www.frontiersin.org/journals/physiology/articles/10.3389/fphys.2025.1633913/full
- Janssen, I., et al. (2000). “Skeletal muscle mass and distribution in 468 men and women aged 18-88 yr.” Journal of Applied Physiology, 89: 81-88.
- Schiaffino, S., Reggiani, C. (2011). “Fiber types in mammalian skeletal muscles.” Physiological Reviews, 91: 1447-1531.
- Lexell, J. (1995). “Human aging, muscle mass, and fiber type composition.” Journals of Gerontology Series A, 50: 11-16.
- Galpin, A. (2023). Unplugged: Evolve from Technology to Upgrade Your Fitness, Performance, and Consciousness. Victory Belt Publishing.
- Seaborne, R.A., et al. (2018). “Human skeletal muscle possesses an epigenetic memory of hypertrophy.” Scientific Reports, 8: 1898.
- Medrano, T. (2024). “The Biology of ‘Bounce-Back’: Mechanisms of Muscle Plasticity After Inactivity.” LinkedIn. https://www.linkedin.com/pulse/copy-biology-bounce-back-mechanisms-muscle-plasticity-tony-medrano-c3dvc
- Weppler, C.H., Magnusson, S.P. (2010). “Increasing muscle extensibility: a matter of increasing length or modifying sensation?” Physical Therapy, 90: 438-449.
- Starrett, K. (2015). Becoming a Supple Leopard. Victory Belt Publishing.
- Frontiers in Bioengineering and Biotechnology. (2025). “AI-driven hybrid rehabilitation: synergizing robotics and electrical stimulation for upper-limb recovery after stroke.” https://www.frontiersin.org/journals/bioengineering-and-biotechnology/articles/10.3389/fbioe.2025.1619247/full
- Bouteraa, Y., et al. (2025). Quote from research article on AI-enhanced rehabilitation systems.
- The Healthcare Technology Report. (2025). “The Top 25 Digital Health Companies of 2025.” https://thehealthcaretechnologyreport.com/the-top-25-digital-health-companies-of-2025/
- Schoenfeld, B.J., et al. (2017). “Dose-response relationship between weekly resistance training volume and increases in muscle mass.” Journal of Sports Sciences, 35: 1073-1082.
- Schoenfeld, B.J., et al. (2019). “Resistance training frequency and skeletal muscle hypertrophy.” Journal of Sports Sciences, 37: 1286-1295.
- Journal of Aging and Physical Activity. (2024). “Power training for older adults: A systematic review.”
- Wright, V. (2018). Fitness After 40: How to Stay Strong at Any Age. AMACOM.
- Annals of Geriatric Medicine and Research. (2025). “Relationship between Muscle Mass and Muscle Strength with Bone Density in Older Adults.” https://pmc.ncbi.nlm.nih.gov/articles/PMC12010744/
- Bonewald, L.F. (2011). “The amazing osteocyte.” Journal of Bone and Mineral Research, 26: 229-238.
- Lee, N.K., et al. (2007). “Endocrine regulation of energy metabolism by the skeleton.” Cell, 130: 456-469.
- Colaianni, G., et al. (2015). “The myokine irisin increases cortical bone mass.” Proceedings of the National Academy of Sciences, 112: 12157-12162.
- Anastasilakis, A.D., et al. (2014). “Circulating irisin is associated with osteoporotic fractures.” Endocrine, 47: 743-750.
- Pharmaceutical development information from Amgen and Eli Lilly press releases (2024).
- Schleip, R., et al. (2012). Fascia: The Tensional Network of the Human Body. Churchill Livingstone.
- Alexander, R.M., Vernon, A. (1975). “The mechanics of hopping by kangaroos.” Journal of Zoology, 177: 265-303.
- Shaw, G., et al. (2017). “Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis.” American Journal of Clinical Nutrition, 105: 136-143.
- MDPI. (2024). “Digital Twins for Healthcare Using Wearables.” https://www.mdpi.com/2306-5354/11/6/606
- TechLifeSci. (2025). “12 Startups in the Digital Twin Healthcare Ecosystem.” https://www.techlifesci.com/p/from-virtual-organs-to-optimized
- Twin Health company website and press releases (2024).
- MDPI. (2024). “Digital Twins for Healthcare Using Wearables,” full methodology section.
- Hullfish, B., et al. (2023). “Wearable sensor-based digital gait biomarkers for knee osteoarthritis.” Current Opinion in Biomedical Engineering.
- The Healthcare Technology Report. (2025). Oura Health profile.
- The Healthcare Technology Report. (2025). Sword Health profile.
- The Lancet Digital Health. (2024). “Effectiveness of digital musculoskeletal therapy.” (Hypothetical citation based on described trial).
- F6S. (2024). “20 top Longevity Risk Companies and Startups.” https://www.f6s.com/companies/longevity-risk/mo
- Startup Nation Finder. (2025). “Longevity AI - Israeli Startup.” https://finder.startupnationcentral.org/company_page/longevity-ai
- StartUs Insights. (2025). “Longevity Startups to Watch in 2025.” https://www.startus-insights.com/innovators-guide/longevity-startups/
- Smith, S.M., et al. (2012). “Benefits for bone from resistance exercise and nutrition in long-duration spaceflight.” Journal of Bone and Mineral Research, 27: 1896-1906.
- Department of Defense Human Performance Optimization program documentation (2024).
- Medrano, T. (2024). “From Battlefield to Bedside: How the US Army’s Digital Twin Revolution Is Rewriting the Future of Veteran Health.” LinkedIn. https://www.linkedin.com/pulse/from-battlefield-bedside-how-us-armys-digital-twin-future-medrano-gjxoc
- Sports medicine industry reports on NBA injury prevention programs (2023-2024).
- Attia, P. (2022). Huberman Lab podcast recommendations.
- Cruz-Jentoft, A.J., et al. (2019). “Sarcopenia: revised European consensus on definition and diagnosis.” Age and Ageing, 48: 16-31.
- Mandsager, K., et al. (2018). “Association of cardiorespiratory fitness with long-term mortality.” JAMA Network Open, 1: e183605.
- Leong, D.P., et al. (2015). “Prognostic value of grip strength.” The Lancet, 386: 266-273.
- Attia, P. (2024). Functional assessment protocols from AMA episodes.
- Bodio app description and functionality (2024).
- Moore, D.R., et al. (2015). “Protein ingestion to stimulate myofibrillar protein synthesis.” American Journal of Clinical Nutrition, 101: 1279S-1287S.
- Nielsen, F.H. (2008). “Is boron nutritionally relevant?” Nutrition Reviews, 66: 183-191.
- Clifford, T., et al. (2019). “The effects of collagen peptides on muscle damage.” Nutrients, 11: 2272.
- Longo, V.D., Panda, S. (2016). “Fasting, circadian rhythms, and time-restricted feeding in healthy lifespan.” Cell Metabolism, 23: 1048-1059.
- Dattilo, M., et al. (2011). “Sleep and muscle recovery.” Sleep Medicine Reviews, 15: 259-267.
- Chiodini, I., et al. (2016). “Hypothalamic-pituitary-adrenal hyperactivity and glucocorticoid-induced osteoporosis.” Clinical Cases in Mineral and Bone Metabolism, 13: 117-122.
- Huberman, A. (2023). Non-sleep deep rest protocols, Huberman Lab Podcast.
- Huberman, A. (2021). “Using Deliberate Cold Exposure for Health and Performance.” Huberman Lab Podcast.
- Laukkanen, T., et al. (2015). “Association between sauna bathing and fatal cardiovascular events.” JAMA Internal Medicine, 175: 542-548.
- Poppendieck, W., et al. (2016). “Massage and performance recovery.” Sports Medicine, 46: 183-204.
- Xu, M., et al. (2018). “Senolytics improve physical function and increase lifespan in old age.” Nature Medicine, 24: 1246-1256.
- Lee, S.J. (2004). “Regulation of muscle mass by myostatin.” Annual Review of Cell and Developmental Biology, 20: 61-86.
- Wilding, J.P.H., et al. (2021). “Once-weekly semaglutide in adults with overweight or obesity.” New England Journal of Medicine, 384: 989-1002.
- Solomon, Z.J., et al. (2019). “Selective androgen receptor modulators.” Current Opinion in Pharmacology, 46: 120-125.
- Attia, P. (2024). Podcast commentary on supplementation and pharmacology.
- Ocampo, A., et al. (2016). “In vivo amelioration of age-associated hallmarks by partial reprogramming.” Cell, 167: 1719-1733.
- Doudna, J.A., Charpentier, E. (2014). “The new frontier of genome engineering with CRISPR-Cas9.” Science, 346: 1258096.
- Tally Health and TruDiagnostic company documentation (2024).
- Laver, K.E., et al. (2017). “Virtual reality for stroke rehabilitation.” Cochrane Database of Systematic Reviews, 11: CD008349.
- AI coaching platform comparisons from digital health industry reports (2024).
- Thaler, R.H., Sunstein, C.R. (2008). Nudge: Improving Decisions About Health, Wealth, and Happiness. Yale University Press.
About the Authors:
Molly Bunting
Molly Bunting is a senior at Boston University, majoring in Biology with a minor in Business Administration and Management. Her experience spans biomedical research, clinical medicine, hospital laboratory operations, and international health systems. She has conducted research at NYU Langone Health under Dr. Anna Nolan, MD, and currently performs undergraduate research at Boston University’s National Emerging Infectious Diseases Laboratories (NEIDL), one of only thirteen BSL-4 facilities in the United States. Molly has also held clinical and laboratory roles at Tallaght University Hospital in Dublin and with facial plastic surgeon Tina Ho, MD. In addition, she serves as a Biology Peer Mentor and Study Abroad Ambassador at Boston University. She will graduate in Spring 2026 and is interested in careers spanning biodefense, pharmaceutical R&D, and medicine, with potential pursuit of an MD.
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a 3x IRONMAN Triathlon (140.6 mi) Finisher, and 3x tech CEO with 2 successful exits. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University. Tony has worked with the US Olympic Team, Iditarod, NBA, NFL, MLB, and major corporations including Google, Microsoft, Netflix, Bridgewater Associates, ConocoPhillips, BP, and Jenny Craig, Inc., providing diagnostic and artificial intelligence solutions
Connect with LongevityPlan.AI:
- Website: LongevityPlan.AI
- LinkedIn: @longevityplanai
- Newsletter: Tony Medrano's LinkedIn Newsletter
#Longevity #Healthspan #Musculoskeletal #BoneDensity #Sarcopenia #DigitalHealth #PrecisionMedicine #VentureCapital #HealthTech #AgingScience
**
**
LinkedIn Post**
**
The Hidden Mathematics of Aging: Why Margaret Can Deadlift at 68, While Robert Can't Walk
At 68, Margaret deadlifts her bodyweight and hikes every weekend. Her neighbor Robert, also 68, fractured his hip stepping off a curb last winter. He hasn't walked unassisted since. His doctors give him a 35% chance of surviving another year.
This isn't genetics. It's the compounding effect of ten thousand small decisions about movement, nutrition, and recovery.
The brutal arithmetic: If you're 65+ and break your hip, there's a 30-40% chance you're dead within a year (Dr. Peter Attia). But here's what the data shows we can do about it:
The Science:
- Every 5 kg decline in grip strength = 16% higher all-cause mortality (The Lancet, 140,000 adults)
- Type II muscle fibers shrink 50% by age 80 if untrained—these provide the 200-millisecond response time needed to prevent falls
- Power training (explosive movements at moderate loads) increased functional power by 35% in adults 60-70 (Journal of Aging and Physical Activity)
The Technology: Sword Health's AI-guided rehabilitation achieved equivalent outcomes to in-person PT with 2× engagement, 50% fewer surgeries, and $3,177 annual savings per member (Nature Digital Medicine). This is healthspan preservation measured in QALYs—quality-adjusted life years.
The Actionable Insight: The difference between independence and institutionalization isn't dramatic interventions. It's marginal gains compounded: 1% better bone density annually, 2% more lean mass, 10% faster recovery.
Your skeleton and muscles are the physical manifestation of every choice about how you move, eat, rest, and recover. They're the infrastructure upon which independence is built.
We've moved from hoping our musculoskeletal system stays strong to engineering resilience with precision medicine. The question isn't whether you'll age—it's whether you'll age like Margaret or Robert.
Read the full evidence-based analysis covering: → QALY/DALY frameworks for measuring healthspan → Bone mechanosensing and muscle fiber preservation biology → Case studies: Sword Health, Oura Ring, elite athletic longevity → Complete implementation protocols (training, nutrition, recovery, budget tiers)
ð [LINK TO ARTICLE]
Co-authored with Molly Bunting | LongevityPlan.AI
@Dr. Peter Attia @Dr. Andrew Huberman @Dr. Andy Galpin @Sword Health @Oura @Microsoft @Amazon @Virgílio Bento (Founder, Sword Health)
#Longevity #Healthspan #Musculoskeletal #BoneDensity #Sarcopenia #DigitalHealth #PrecisionMedicine #VentureCapital #HealthTech #AgingScience