Sports Medicine
·18 min read
Does Distance Running Cause Arthritis?
Debunking the Myth: How Science, AI, and Personalized Medicine Are Rewriting the Rules of Joint Health for Endurance Athletes
By Dr. Eric Rightmire, Board Certified Orthopedic Surgeon, LongevityPlan.AI Board Member
The knee strikes the pavement. Again. And again. Over 26.2 miles, a marathon runner's knee absorbs approximately 110 tons of cumulative force—roughly equivalent to the weight of a fully loaded Boeing 737. Multiply that across hundreds of training runs and dozens of marathons, and you'd assume the inevitable outcome: worn cartilage, grinding joints, and a one-way ticket to arthritis.
Except that assumption is wrong.

Figure 1. During a single marathon, a runner's knee absorbs approximately 110 tons of cumulative ground-reaction force—yet large-scale epidemiological studies show marathon runners develop arthritis at lower rates than the sedentary general population. Image concept adapted from biomechanical loading research (Miller et al., 2014).
The largest study of marathon runners ever conducted—surveying 3,804 participants from the 2019 and 2021 Chicago Marathons—found something remarkable: the prevalence of hip and knee arthritis among these distance athletes was just 7.3%, significantly lower than the general population rate of 10-15% for adults over 40. Even more striking, the study found zero correlation between arthritis risk and the number of marathons completed, years spent running, weekly mileage, or running pace. A runner who had completed 664 marathons (yes, that was the study's upper range) had no higher arthritis risk than someone running their first.
This finding fundamentally challenges decades of medical dogma—the persistent "wear-and-tear" narrative that has led physicians to advise nearly one in four runners to reduce their mileage, and nearly half of runners with arthritis to stop running altogether. As Dr. Matthew Hartwell, lead author of the Northwestern University study and now an orthopedic surgery fellow at UC San Francisco, explains: "We're often compared to being like a car. If you liken people to cars, intuitively it makes sense that the more you use your joints, the more you're going to wear them out. But the joint is really an active, living part of the body, almost like an organ."
The Biomechanics Paradox: Why Runners Don't Wear Out Their Knees
To understand why running doesn't destroy joints, we need to examine what actually happens at the cellular and mechanical level when the foot meets the ground. The counterintuitive physics of running provides the first clue: while peak forces during running are indeed higher than walking—roughly 2.5 times body weight compared to 1.2 times for walking—runners spend far less time in ground contact. The stride time during running is approximately 40% shorter than walking, and runners cover more distance per stride.
This leads to what biomechanists call "per-unit-distance" (PUD) loads. Research from Queen's University found that when you calculate the total mechanical load per kilometer traveled, running and walking impose nearly identical stresses on knee cartilage. The higher peak forces of running are offset by shorter ground contact time and longer stride length. As Dr. Ross Miller, lead researcher on the PUD study, notes: "Peak knee joint contact forces in running are much higher than they are in walking, but the comparatively brief stance phase and long stride length appear to counterbalance this, such that the cumulative load per distance traveled is similar."
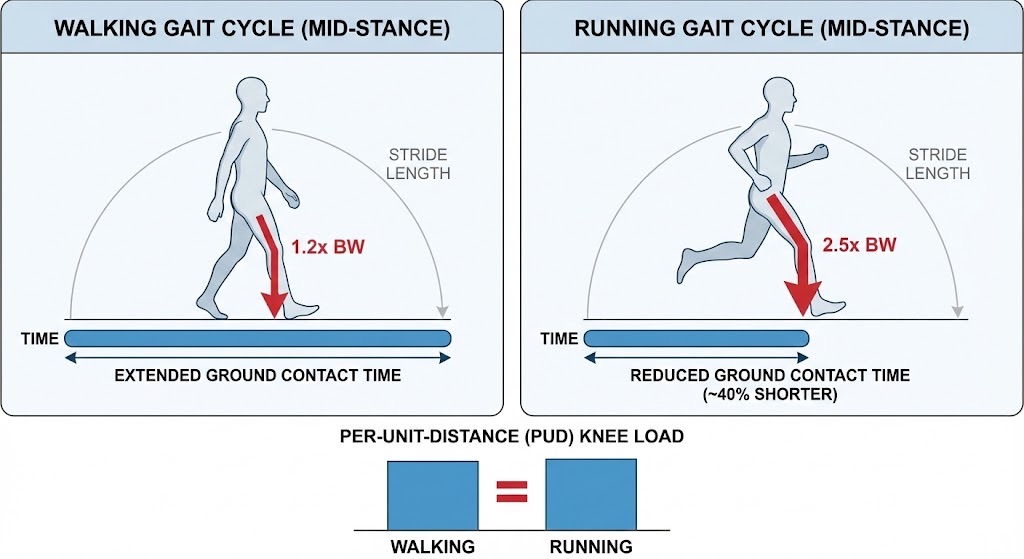
Figure 2. Although peak knee forces during running are roughly double those of walking, the shorter ground-contact time and longer stride length equalize the total per-unit-distance (PUD) mechanical load on the knee joint. This biomechanical equivalence helps explain why distance running does not accelerate cartilage degradation (Miller et al., 2014; Queen's University research).
But the story gets more interesting. Cartilage, unlike the passive rubber of a car tire, is a metabolically active tissue that responds to mechanical loading. Within the synovial joint, chondrocytes—the cells that maintain cartilage—actually require cyclical loading to maintain tissue health. These cells respond to mechanical stimulation by increasing production of proteoglycans and collagen, the essential building blocks of cartilage matrix. Too little load (as in prolonged bed rest) leads to cartilage atrophy; too much uncontrolled load (particularly from sudden impacts or misaligned biomechanics) can trigger degradation.
Running provides what physiologists call the "Goldilocks zone" of mechanical stimulation: regular, predictable loading that promotes cartilage adaptation without overwhelming repair mechanisms. A 2024 study using advanced MRI techniques tracked cartilage changes in competitive distance runners following high-intensity interval training. Researchers found temporary increases in cartilage water content immediately post-exercise (indicating fluid exchange, a normal physiological response), but no structural damage or degradation markers over a 12-week training period.
The Real Culprits: What Actually Increases Arthritis Risk
If running volume doesn't predict arthritis, what does? The Northwestern study identified four primary risk factors, each backed by decades of epidemiological research:
-
Previous Joint Injury: The single strongest predictor of osteoarthritis is prior joint trauma, particularly ACL tears, meniscus injuries, or fractures involving the articular surface. A history of knee surgery increases arthritis risk by approximately 3-6 fold, depending on the severity and type of injury. This makes intuitive sense: traumatic injury disrupts the normal joint architecture, creates areas of abnormal stress distribution, and triggers inflammatory cascades that can persist for years.
-
Body Mass Index (BMI): Every additional kilogram of body weight increases knee joint forces by approximately 3-4 kilograms during walking and 7-8 kilograms during stair climbing. Obesity also contributes systemic inflammation through adipokines—inflammatory signaling molecules secreted by fat tissue—that can accelerate cartilage breakdown. The Northwestern study found a clear dose-response relationship between BMI and arthritis prevalence.
-
Age: Unsurprisingly, arthritis prevalence increases with age. However, the relationship isn't simply cumulative "wear and tear." Age-related changes include decreased chondrocyte responsiveness to growth factors, accumulation of oxidative damage, reduced synovial fluid production, and alterations in subchondral bone metabolism. The key insight: runners in their 40s and 50s show arthritis rates lower than sedentary individuals of the same age, suggesting that appropriate mechanical loading may actually slow age-related joint degeneration.
-
Family History: Genetics play a substantial role, with heritability estimates for osteoarthritis ranging from 40-65% depending on the joint. Multiple genes have been identified that influence cartilage structure, inflammatory response, and bone remodeling. However, genetic predisposition is not destiny—environmental factors like activity level, body weight, and injury prevention significantly modulate genetic risk.
Notably absent from this list: running volume, running intensity, or cumulative lifetime mileage. As Dr. Vehniah Tjong, associate professor of orthopedic surgery at Northwestern and study co-author, emphasizes: "Recreational runners are a dedicated group of people who use the sport for exercise, mental clarity, or to challenge themselves. They should be encouraged by our results."
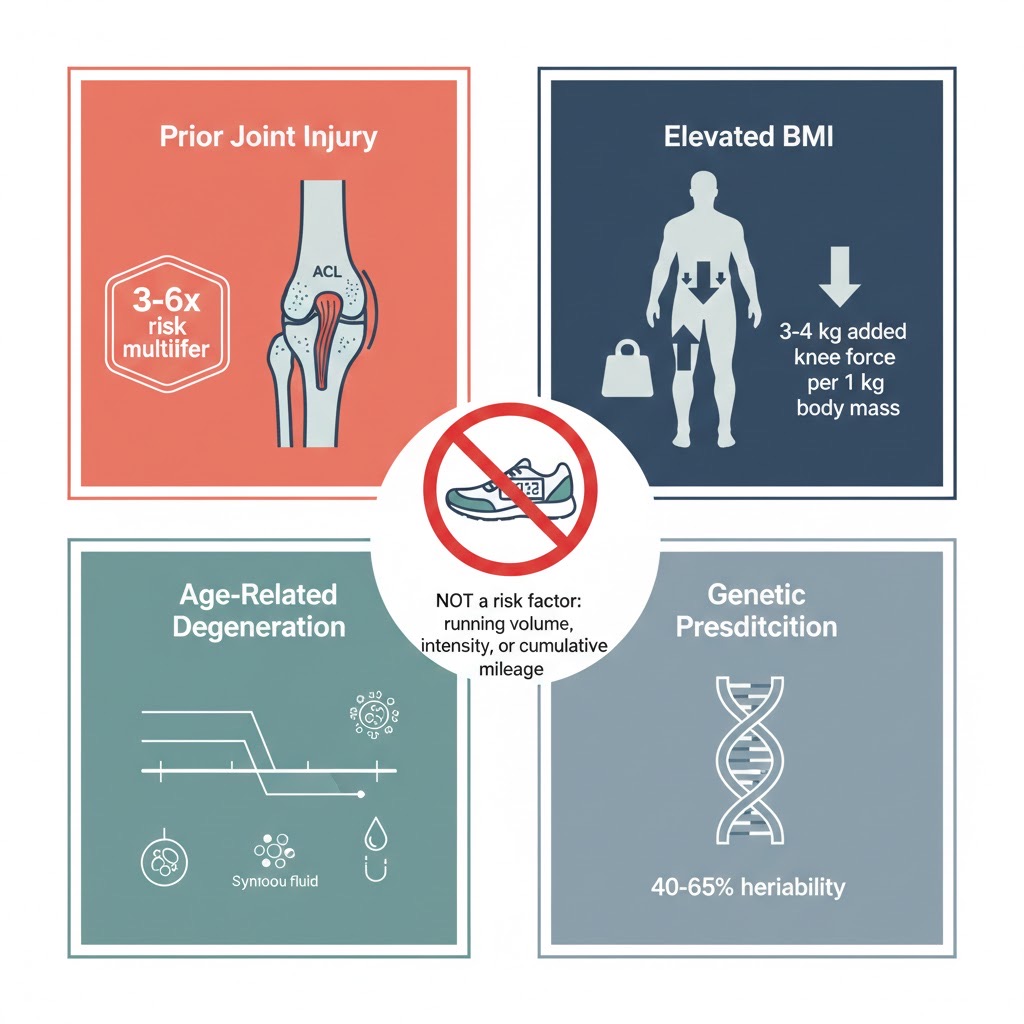
Figure 3. The four primary risk factors for osteoarthritis were identified by the Northwestern University Chicago Marathon study (Hartwell et al., 2024). Notably, running volume, pace, years of running, and total marathons completed showed zero correlation with arthritis prevalence among 3,804 marathon participants.
The Elite Athlete Exception: Why Professional Runners Face Different Risks
While recreational running appears remarkably joint-safe, research consistently shows elevated arthritis rates among elite and professional runners. A comprehensive 2017 meta-analysis published in the Journal of Orthopaedic & Sports Physical Therapy found that elite runners had an arthritis prevalence of 13.3%, compared with 3.5% among recreational runners and 10.2% among sedentary individuals.
What explains this U-shaped curve, in which both sedentary individuals and elite athletes show higher rates of arthritis than recreational runners? The answer likely involves several factors:
Training volume and intensity: Elite runners commonly log 100-140 miles per week at race-pace intensities that recreational runners rarely sustain. This extreme volume may exceed the adaptive capacity of cartilage repair mechanisms. Additionally, elite athletes often push through minor injuries to maintain competitive schedules—micro-trauma that accumulates over the years.
Biomechanical optimization: Elite runners optimize for speed and efficiency, which may involve biomechanical patterns that increase localized joint stress. Dr. Jeffrey Driban, an osteoarthritis researcher at Tufts University, notes that "the pursuit of marginal performance gains might lead to movement patterns that, while faster, create uneven cartilage loading."
Career length and injury history: Elite runners typically have 10-20+ year competitive careers with higher cumulative injury exposure. Many elite runners have experienced significant injuries—stress fractures, IT band syndrome, plantar fasciitis—that alter biomechanics and may contribute to later joint problems.
The critical insight: the dose-response relationship between running and joint health likely follows a J-shaped or U-shaped curve. Moderate recreational running (20-40 miles per week) appears protective compared to sedentary behavior. At extreme volumes (100+ miles per week sustained for years), risk may increase—though even at elite levels, arthritis rates are comparable to or slightly higher than sedentary populations, not dramatically elevated.
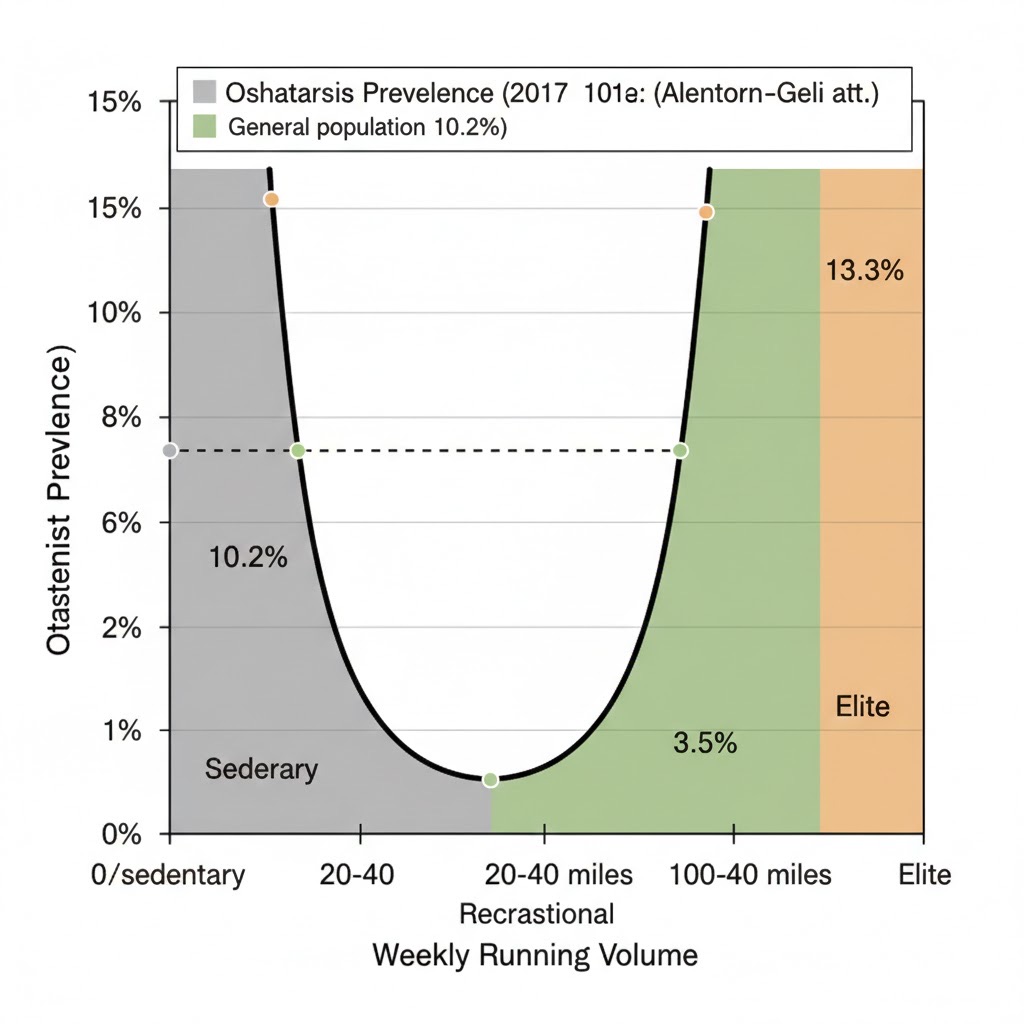
Figure 4. Osteoarthritis prevalence follows a U-shaped dose-response curve relative to running volume. Recreational runners (20–40 miles/week) show the lowest arthritis rates at 3.5%, compared to 10.2% for sedentary individuals and 13.3% for elite athletes. Data from Alentorn-Geli et al., 2017 meta-analysis (Journal of Orthopaedic & Sports Physical Therapy).
AI and Digital Twins: The Future of Personalized Running Medicine
Understanding population-level statistics is useful, but the cutting edge of sports medicine lies in personalization. This is where artificial intelligence, wearable sensors, and digital twin technology are revolutionizing how we understand and optimize individual running biomechanics.
Real-Time Biomechanical Monitoring
Until recently, detailed biomechanical analysis required laboratory-based motion capture systems with force plates—equipment that costs hundreds of thousands of dollars and constrains movement to artificial settings. But in October 2024, researchers from Harvard's John A. Paulson School of Engineering and Applied Sciences published breakthrough work showing that simple, commercially available inertial measurement units (IMUs) combined with machine learning can accurately estimate ground-reaction forces during real-world running.
Lead author Dr. Lauren Baker, working with Professor Conor Walsh (the Paul A. Maeder Professor of Engineering) and evolutionary biologist Dr. Daniel Lieberman, demonstrated that sensors worn on the hip and lower leg could predict braking forces, propulsion forces, and overstriding patterns with accuracy comparable to laboratory equipment. The machine learning model required just eight steps of calibration data per individual to personalize predictions—making real-time, outdoor biomechanical coaching feasible for the first time.
"Wearable sensors, combined with machine learning, can accurately estimate the forces acting on a runner's body—not just in the lab, but out in the real world," Baker explains. "This opens up possibilities for injury prevention that simply weren't possible before."
Dr. Walsh's lab is now extending these capabilities beyond force estimation. "More data to understand performance for recreational or elite athletes is a trend that is only increasing," Walsh notes. "We recognize there is a big gap between what existing commercial wearables measure, and what we would really like to measure—to really understand running form or athletic performance. I think we're looking at extending wearables to not just measure steps, speed, or heart rate, but to really give a more detailed understanding of how the body is moving."

Figure 5. Commercially available inertial measurement units (IMUs) placed at the hip and lower leg can estimate ground-reaction forces with accuracy comparable to laboratory force plates, requiring only eight steps of calibration per individual. This breakthrough by Harvard researchers (Baker et al., 2024) makes real-time biomechanical coaching feasible for everyday runners.
The Cardiorespiratory Digital Twin™: Integrating Multiple Data Streams
While biomechanical sensors track movement patterns, a comprehensive approach to longevity planning requires integration of multiple physiological systems. This is where the concept of a Cardiorespiratory Digital Twin™ becomes transformative: a dynamic, personalized computational model that integrates cardiovascular fitness, respiratory capacity, metabolic efficiency, biomechanical loading, and recovery patterns into a unified predictive framework.
Companies like Siemens Healthineers, Microsoft, and GE Healthcare are pioneering digital twin applications in healthcare. In September 2024, Siemens partnered with Mayo Clinic to develop AI-enhanced digital twins for cardiovascular care, capable of simulating patient-specific responses and predicting complications. While initially focused on cardiac patients, these technologies are rapidly extending to athletic performance optimization.
Twin Health, a digital health company based in California, has created one of the most sophisticated implementations of personal digital twins for metabolic health. Their platform integrates data from continuous glucose monitors, wearable activity trackers, sleep monitors, and periodic lab tests to build comprehensive metabolic models. While their current focus is reversing Type 2 diabetes, the underlying technology—creating dynamic simulations that predict how individual bodies respond to various inputs—is directly applicable to athletic performance and injury prevention.
For runners concerned about joint health, a Cardiorespiratory Digital Twin™ could integrate:
- Real-time biomechanical data from IMU sensors tracking ground reaction forces, stride asymmetry, and impact loading patterns
- Cardiovascular stress and recovery metrics from heart rate variability, VO₂max estimates, and training load
- Inflammatory biomarkers and recovery status from blood chemistry, cortisol patterns, and sleep quality
- Joint health indicators from periodic imaging (MRI-based cartilage thickness measurements) and patient-reported outcome measures
- Genetic risk profiles for cartilage structure, inflammatory response, and injury susceptibility
This integrated approach enables predictive analytics: identifying when training load exceeds recovery capacity, detecting biomechanical drift that increases injury risk, and optimizing training progression to maximize adaptations while minimizing cumulative damage. As Tony Medrano has emphasized in previous analyses, this represents a fundamental shift from reactive medicine (treating problems after they occur) to predictive, preventive, and personalized optimization.
Machine Learning for Cartilage Health: From Lab to Clinical Practice
While wearable sensors track external biomechanics, sophisticated imaging combined with AI is revolutionizing our ability to directly assess cartilage health. Traditional radiographic assessment of osteoarthritis—the Kellgren-Lawrence grading system—is relatively crude, detecting only late-stage disease when joint space has already narrowed significantly.
Advanced MRI techniques can now quantify cartilage thickness down to sub-millimeter precision, detect changes in cartilage composition (through T2 relaxometry and other sequences), and identify early bone marrow lesions that precede cartilage loss. But analyzing these images manually is time-consuming and subject to inter-observer variability. This is where deep learning excels.
In 2024, researchers from the University of California San Francisco published work demonstrating that U-Net-based deep learning models could segment knee cartilage and menisci from MRI with Dice coefficients (a measure of accuracy) between 0.770 and 0.878—comparable to expert human radiologists—in just 5 seconds per scan. More impressively, these models showed strong correlation with manual measurements of cartilage thickness and tissue quality, making them viable for clinical workflows.
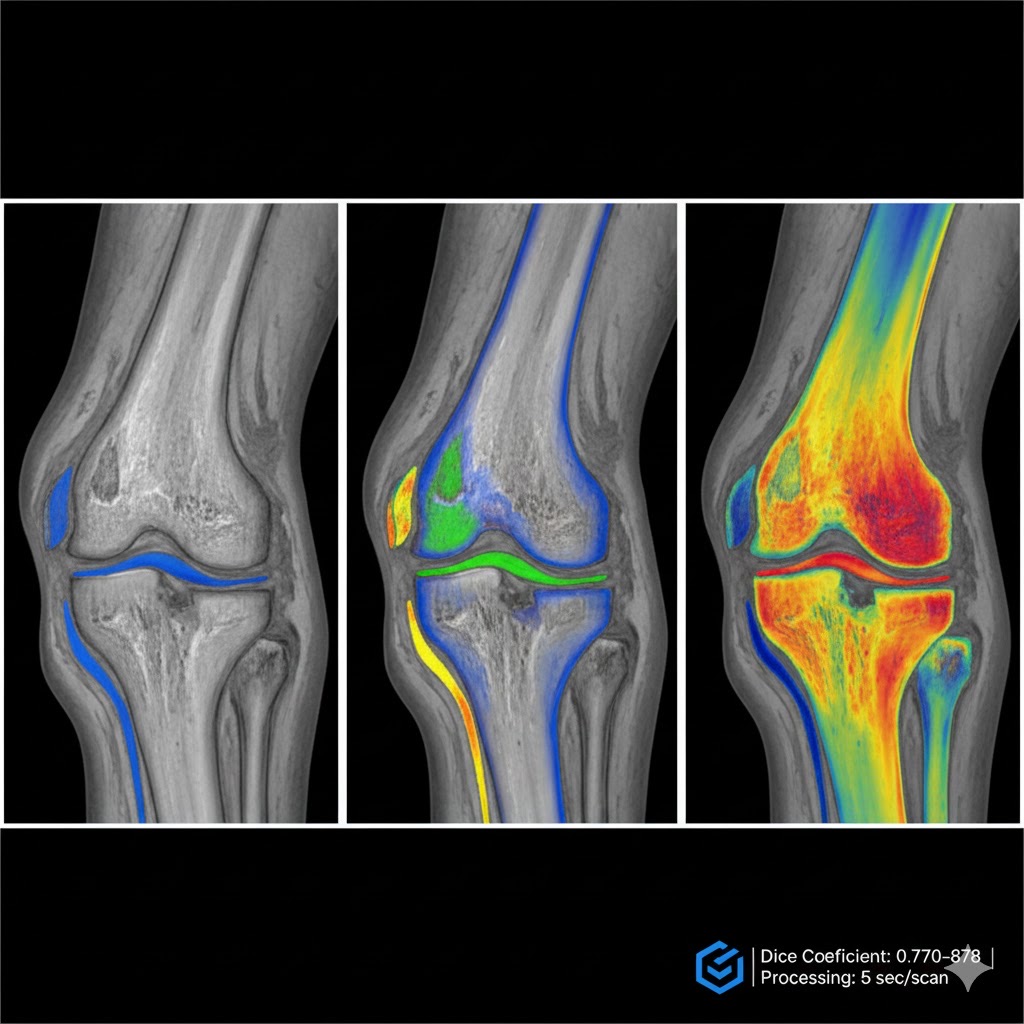
Figure 6. U-Net-based deep learning models can automatically segment knee cartilage and menisci from MRI scans in approximately 5 seconds, achieving accuracy comparable to expert radiologists (Dice coefficients 0.770–0.878). This technology enables scalable longitudinal cartilage monitoring for runners and early detection of osteoarthritis (Norman et al., 2024; Joseph et al., 2025).
A comprehensive 2025 review in Osteoarthritis and Cartilage Open by Dr. Gabby Joseph and colleagues at UCSF surveyed the rapid advances in machine learning for osteoarthritis prediction. The review identified several key applications:
Predictive modeling of disease progression: Machine learning models integrating demographics, symptoms, muscle strength, physical activity patterns, and MRI findings can predict cartilage loss with areas under the ROC curve (AUC) of 0.77-0.79. Crucially, simplified models using just the top 10 predictive features performed nearly as well as complex 112-feature models—suggesting clinical feasibility.
Automated quantification of joint structures: Deep learning tools can automatically measure not just cartilage thickness but also quantify bone marrow lesions, synovitis (joint inflammation), and even subcutaneous fat around the knee—all factors that contribute to osteoarthritis risk. This automation dramatically increases the feasibility of large-scale longitudinal monitoring.
Surgical outcome prediction: ML models have demonstrated strong performance in predicting which patients will eventually require total knee replacement, with potential for guiding early intervention strategies and surgical planning.
Dr. Joseph and colleagues emphasize three emerging directions critical for translating these tools into clinical practice: building interpretable models that clinicians can trust, external validation using independent datasets to ensure generalizability, and integrating multimodal data sources (clinical, imaging, genetic, biomechanical) for comprehensive prediction.
For runners, this technology offers the possibility of baseline cartilage mapping—establishing a personal reference point—followed by periodic monitoring to detect early changes long before symptoms appear. Combined with biomechanical data from wearables, this creates a complete picture of joint health that enables proactive intervention rather than reactive treatment.
Running With Existing Arthritis: The Case for Continued Activity
Perhaps the most clinically relevant question isn't whether running causes arthritis in healthy joints, but whether continuing to run is safe for individuals who already have osteoarthritis. Here, emerging research challenges the traditional medical advice to "stop running before you make it worse."
A groundbreaking 2025 pilot study published in medRxiv investigated the biological and pain responses to a walk-run program in eight participants with self-reported knee osteoarthritis. The research team, led by Dr. Bernard Liew at Teesside University, measured cartilage stress markers (specifically COMP—cartilage oligomeric matrix protein), pressure pain thresholds, and biomechanical loading during a 25-minute mixed walk-run protocol on an instrumented treadmill.
The results were remarkable. Despite experiencing moderate peak knee loads during the running intervals, participants showed:
- No significant increase in serum COMP levels immediately post-exercise or 30 minutes after (indicating no acute cartilage breakdown)
- Increased pressure pain thresholds at both the knee and a distant site (the elbow), suggesting exercise-induced hypoalgesia—a systemic pain-reducing effect
- Well-tolerated biomechanical loads that remained within normal ranges throughout the protocol
This aligns with a broader body of evidence showing that appropriate physical activity—including high-impact exercises like running—can be beneficial even with existing osteoarthritis. The European League Against Rheumatism (EULAR) 2018 recommendations for physical activity in people with osteoarthritis explicitly state that exercise is safe and should be a core component of management, regardless of disease severity, pain, or structural damage.
The mechanism appears to be multifactorial. Exercise provides the mechanical stimulus necessary for maintaining cartilage health, improves joint range of motion, strengthens periarticular muscles that stabilize and protect the joint, reduces systemic inflammation, and triggers endogenous pain modulation through multiple neurobiological pathways. The key is appropriate dosing—starting with walk-run intervals for those with existing arthritis, gradually progressing based on symptoms and recovery, and avoiding sudden increases in volume or intensity.
Industry Applications: How Elite Organizations Optimize Joint Health
Professional sports organizations have been early adopters of advanced biomechanical monitoring and AI-powered injury prevention—technologies that are now becoming accessible to serious recreational athletes and health-conscious individuals planning for extended healthspan.
NFL Teams and Injury Prevention
NFL teams have invested heavily in wearable technology and predictive analytics. GPS tracking units, accelerometers, and inertial measurement sensors are now standard equipment during practices and games, collecting data on player load, impact forces, and movement patterns. Teams like the Seattle Seahawks and New England Patriots employ dedicated data science teams to analyze this information, adjusting practice intensity and playing time based on fatigue indicators and injury risk scores. The investment is substantial—but so is the payoff, with injury prevention potentially saving teams millions in player salaries and competitive performance.
Stanford Athletics and Olympic Teams
Stanford University's athletic department has pioneered the integration of wearable technology with academic research. Their sports medicine team works closely with biomechanics researchers in the School of Engineering, creating a feedback loop where laboratory insights inform field applications and real-world athlete data drives research questions.
Similarly, the U.S. Olympic & Paralympic Committee has established the Olympic & Paralympic Training Center in Colorado Springs with state-of-the-art biomechanics laboratories, environmental chambers for altitude simulation, and comprehensive physiological monitoring. Athletes undergo regular biomechanical assessments that track subtle changes in movement patterns that might indicate fatigue, compensation for injury, or technical drift—all factors that could increase injury risk over time.
Emerging Commercial Applications
Several companies are translating elite-level monitoring into consumer-accessible products:
WHOOP and Oura have popularized continuous physiological monitoring for recovery optimization. While these platforms focus primarily on cardiovascular and sleep metrics, they're increasingly incorporating movement quality data. WHOOP's Strain Coach uses machine learning to recommend daily training intensity based on recovery status—preventing the accumulation of fatigue that increases injury risk.
Strava, with over 100 million users, has become the world's largest repository of running biomechanics data. While currently used primarily for social features and performance tracking, the company is exploring AI-powered training recommendations and injury risk algorithms based on aggregated user data. The scale of Strava's dataset—billions of activities—enables population-level insights into training patterns that predict injury.
Nurvv Run has developed shoe insoles with 32 embedded sensors that measure foot strike, pronation, cadence, and ground contact time with millimeter precision. Their AI coaching system provides real-time audio feedback to correct biomechanical inefficiencies that increase injury risk. Early adopters report significant reductions in overuse injuries through subtle gait corrections.
Viome, while focused primarily on microbiome analysis and metabolic health, represents the broader trend toward multi-omics personalization. Their platform integrates gut microbiome sequencing, blood biomarker analysis, and dietary tracking to create personalized nutrition recommendations—relevant because systemic inflammation driven by gut dysbiosis may contribute to osteoarthritis progression.
Fountain Life offers comprehensive health assessments combining full-body MRI, coronary CT angiography, advanced blood biomarker panels, and DEXA scans—the kind of baseline health mapping that enables true preventive medicine. For affluent individuals concerned about longevity, their assessments can include detailed musculoskeletal imaging that establishes baseline joint health for longitudinal monitoring. While expensive (assessments start around $20,000), this represents the premium end of personalized preventive medicine.
Practical Recommendations: Optimizing Running for Long-Term Joint Health
Based on current evidence, what should runners do to maximize the joint-protective effects of running while minimizing risks? The science points to several evidence-based strategies:
1. Maintain Healthy Body Composition
Every kilogram of excess weight amplifies joint loading. For runners, maintaining a BMI in the healthy range (18.5-24.9) appears to be one of the most modifiable risk factors for arthritis. This doesn't mean pursuing extreme leanness—the goal is functional body composition that supports performance without imposing unnecessary joint stress.
2. Prioritize Injury Prevention and Proper Rehabilitation
Given that prior injury is the single strongest predictor of arthritis, injury prevention should be paramount. This means:
- Progressive training increases (the "10% rule" of not increasing weekly mileage by more than 10% remains sound)
- Adequate recovery between hard efforts
- Strength training to build resilient tissues and correct biomechanical imbalances
- Proper warm-up and cool-down protocols
- Addressing pain promptly rather than running through it
When injuries do occur, complete rehabilitation is critical. Returning to running before tissues have fully healed creates altered movement patterns and compensations that increase subsequent injury risk.
3. Monitor and Optimize Biomechanics
While perfect running form remains elusive and highly individual, certain biomechanical patterns clearly increase injury risk. Overstriding (landing with the foot far ahead of the center of mass) increases braking forces and loads the knee more stressfully. Excessive vertical oscillation wastes energy and increases impact forces. Gross asymmetries between left and right sides suggest compensation patterns.
The Harvard research on wearable biomechanical monitoring offers a glimpse of the future: imagine receiving real-time audio feedback during your run—"Reduce overstriding by 10%" or "Left-right asymmetry increasing, check for fatigue"—based on sensors that cost a few hundred dollars. This technology is moving from research labs to consumer products within the next 2-3 years.
4. Consider Walk-Run Intervals
Particularly for individuals with existing joint concerns or those returning from injury, walk-run intervals provide the mechanical stimulus benefits of running while managing cumulative load. The 2025 study showing safe walk-run protocols for individuals with osteoarthritis suggests this approach can be beneficial even with existing cartilage damage.
Jeff Galloway's run-walk method has gained popularity among marathon runners, with many athletes reporting reduced injury rates and improved recovery while maintaining competitive performance. The physiological rationale is sound: brief walking intervals provide partial recovery without completely unloading the cardiovascular system, potentially optimizing the balance between training stimulus and mechanical stress.
5. Integrate Complementary Training
Strength training, particularly eccentric exercises targeting the quadriceps, hamstrings, and hip stabilizers, has strong evidence for reducing running injury rates. A 2024 systematic review found that neuromuscular training programs reduced lower extremity injury risk by approximately 35% in runners.
Cross-training with low-impact activities—cycling, swimming, elliptical—provides cardiovascular fitness maintenance while giving joints periodic breaks from impact loading. The Northwestern study found no difference in arthritis rates between runners who cross-trained and those who didn't, but cross-training does appear to reduce overuse injury risk.
The Longevity Perspective: Running as Healthspan Extension
Focusing exclusively on arthritis risk misses the bigger picture: the relationship between running and overall healthspan. Cardiorespiratory fitness—measured by VO₂max—is one of the strongest predictors of all-cause mortality and healthy life expectancy. Every 1-MET increase in VO₂max (equivalent to roughly a 10% improvement in aerobic capacity) corresponds to a 10-15% reduction in mortality risk.
Regular running provides:
- Reduced cardiovascular disease risk (30-50% lower incidence of coronary artery disease)
- Improved metabolic health (significantly reduced Type 2 diabetes risk)
- Enhanced cognitive function and reduced dementia risk
- Better mental health outcomes (reduced depression and anxiety)
- Maintained bone density (reducing osteoporosis risk)
- Extended lifespan—runners live approximately 3-6 years longer than non-runners, even after adjusting for other health behaviors
A landmark 2008 study from Stanford University followed 538 runners and 423 non-runner controls for 21 years, starting when participants were in their 50s. The results were dramatic: runners had 39% lower mortality rates and significantly delayed onset of disability. Even into their 70s and 80s, the runners maintained functional independence far longer than controls.
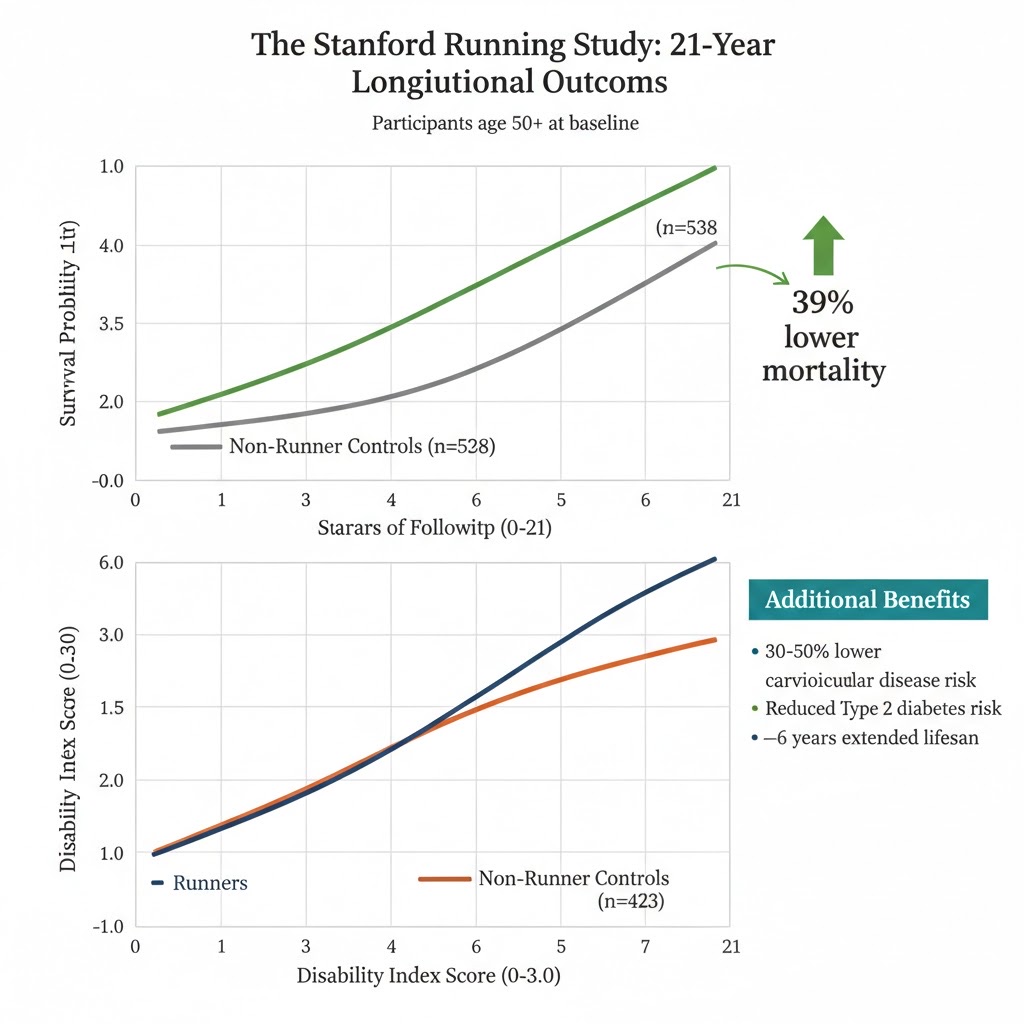
Figure 7. The landmark 21-year Stanford longitudinal study (Chakravarty et al., 2008) demonstrated that runners experienced 39% lower mortality rates and significantly delayed onset of disability compared to non-runner controls, with benefits persisting into participants' 70s and 80s—underscoring that the systemic health benefits of running far outweigh theoretical joint concerns.
The key insight: even if running carried a slightly elevated arthritis risk (which current evidence suggests it doesn't for recreational runners), the overall health benefits would likely still make it worthwhile. An extra 3-6 years of life with slightly higher arthritis risk would be a reasonable trade-off. But the evidence suggests we don't have to make that trade-off—recreational running appears to provide comprehensive health benefits without increasing joint disease risk.
Conclusion: Rewriting the Narrative on Running and Joint Health
The myth that running causes arthritis persists despite mounting evidence to the contrary. The largest studies to date—including the 3,804-participant Northwestern survey and multiple longitudinal cohorts—consistently show that recreational running does not increase arthritis risk and may even be protective compared to sedentary behavior.
The real risk factors for arthritis—prior injury, obesity, genetics, and age—are independent of running volume. Elite athletes do show elevated rates, but this likely reflects extreme training volumes and injury exposure that recreational runners don't experience. For the vast majority of runners logging 20-50 miles per week, joints appear remarkably resilient to repetitive loading.
The future of running medicine lies in personalization. AI-powered biomechanical monitoring, machine learning prediction of injury risk, digital twin simulations integrating multiple data streams, and advanced imaging to track cartilage health are transforming our ability to optimize training for each individual. What once required expensive laboratory equipment and expert interpretation is becoming accessible through consumer wearables and cloud-based analytics.
For health-conscious individuals planning for extended healthspan—the aspirational athletes, executives, and parents seeking to model healthy behavior—running remains one of the most time-efficient, accessible, and effective interventions for overall health. The key is intelligent implementation: progressive training, injury prevention, biomechanical awareness, and periodic assessment to catch problems before they become serious.
As Dr. Hartwell concludes: "We should move away from the idea of our bodies being like a car and our joints being like car tires that we're just going to wear out with more miles. Instead, we should focus on taking care of and paying attention to our bodies as we run, so that if we experience pain, we can address it."
The joint is not a passive mechanical component destined to wear out—it's a living, adaptive organ that thrives on appropriate use. With the right tools, knowledge, and personalized approach, running can be sustained not just for years but for decades, contributing to both longer life and better quality of life. The science is clear: distance running, done intelligently, is not the path to arthritis. It may be one of the most powerful tools we have for joint longevity—and now, for the first time, we have the technology to personalize that tool for every individual who laces up and hits the road.
About the Author
Dr. Eric Rightmire is a dual Board Certified Orthopedic Surgeon specializing in sports medicine. He earned his BA from Harvard University and his MD from SUNY. He completed his residency and internship at Harvard. Dr. Rightmire has served as an orthopedic surgeon to celebrity athletes and is a member of the prestigious Quigley Society. His expertise in sports injuries and arthritis treatment makes him a valuable advisor to the LongevityPlan.AI team.