Longevity
·17 min read
The Biology of 'Bounce-Back': Mechanisms of Muscle Plasticity After Inactivity
How Skeletal Muscle Memory and Recovery Dynamics Are Revolutionizing Longevity Planning for Athletes, Executives, and the Health-Conscious
By Tony Medrano & Molly Bunting, LongevityPlan.AI
The human body possesses a remarkable capability that sounds almost too good to be true: muscles remember their former strength, even after months of inactivity. Exercise physiologist Kristoffer Toldnes Cumming describes this as cellular memory that remembers past glory, and recent research is revealing the sophisticated molecular mechanisms that make this "bounce-back" phenomenon possible—with profound implications for how we approach longevity, healthspan, and recovery throughout our lives.
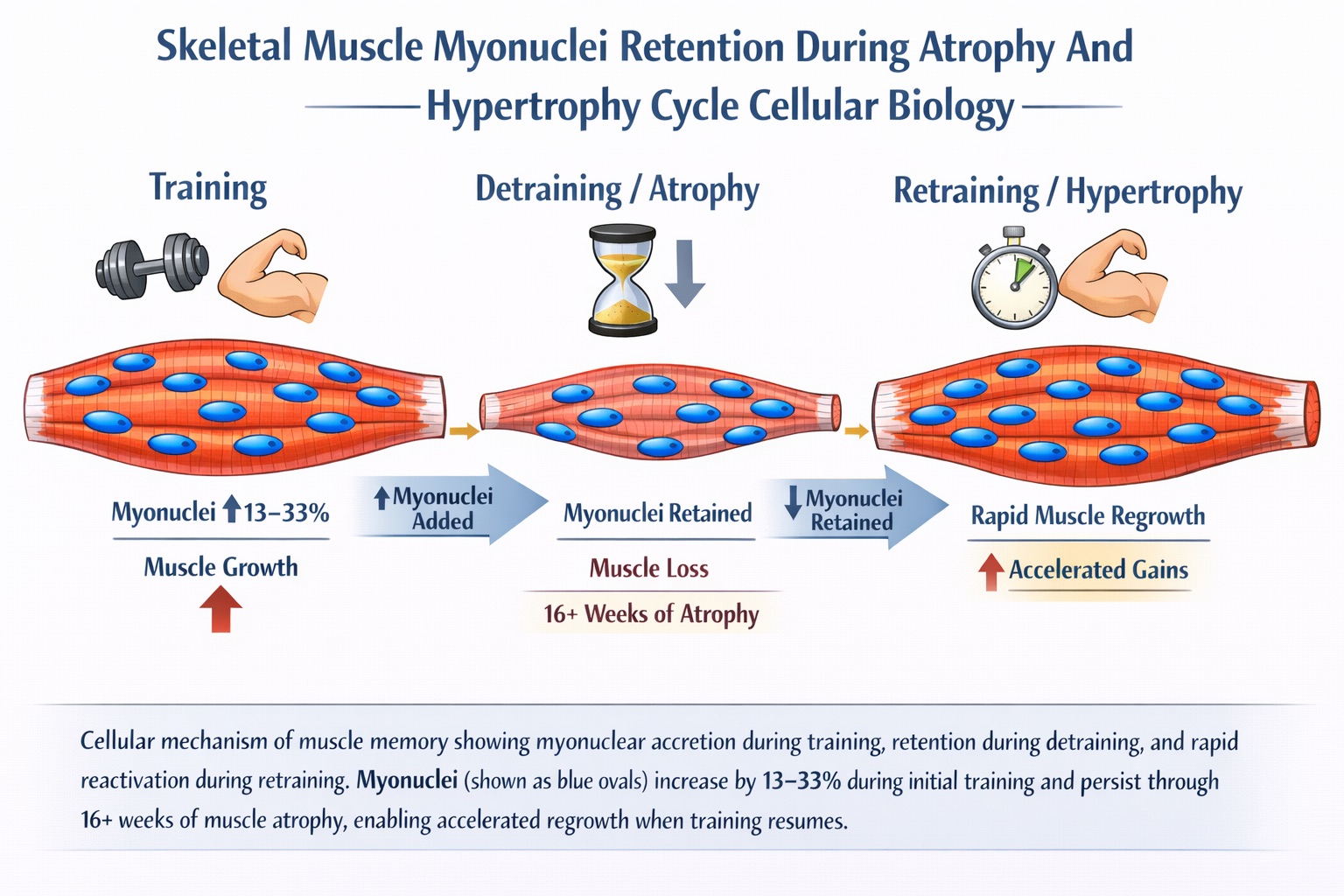
Cellular mechanism of muscle memory showing myonuclear accretion during training, retention during detraining, and rapid reactivation during retraining. Myonuclei (shown as blue ovals) increase by 13-33% during initial training and persist through 16+ weeks of muscle atrophy, enabling accelerated regrowth when training resumes.
The Cellular Memory Revolution: More Than Just Motivation
For decades, conventional wisdom held that taking extended breaks from training meant starting from scratch. Athletes feared detraining periods, executives worried about business travel disrupting fitness routines, and aging individuals assumed that muscle loss was irreversible. The emerging science of muscle memory is rewriting this narrative entirely.
Research demonstrates that skeletal muscle tissue can be primed by earlier positive encounters with exercise training that can enhance adaptation to later retraining, even following significant periods of exercise cessation or detraining. This isn't merely about neurological adaptations or "remembering" how to perform movements—it's a fundamental biological process occurring at the cellular and epigenetic levels.
The implications extend far beyond athletic performance. Understanding muscle plasticity mechanisms is crucial for maintaining healthspan—the number of years lived in good health—as we age. While conventional longevity discussions focus on lifespan extension, the real game-changer is maintaining functional capacity, independence, and quality of life into our later decades.
The Tom Brady Phenomenon: Elite Athletic Longevity Through Recovery Science
Perhaps no athlete better exemplifies the practical application of muscle recovery science than Tom Brady, who competed at elite NFL levels until age 45—an achievement unprecedented in professional football. Brady's longevity wasn't accidental; it was the result of a meticulously designed system called the TB12 Method, developed with his longtime trainer Alex Guerrero.
At the core of Brady's approach is "muscle pliability"—a term that effectively describes maintaining muscles in a state optimized for rapid recovery and retraining. Instead of the typical "push until you break" training model, the TB12 Method is designed to balance stress with deliberate recovery, almost like a constant cycle of prehabilitation to slow the effects of age.
Brady's 2008 ACL injury became a pivotal moment. Rather than following conventional rehabilitation protocols emphasizing heavy strength training, Brady turned towards pliability work for recovery, which helped him regain function faster than conventional methods. This experience cemented his belief that maintaining recovery capacity was as important as building strength.
The TB12 philosophy aligns remarkably with cutting-edge muscle memory research. By avoiding the chronic muscle damage and inflammation that comes from excessive heavy lifting, Brady preserved his satellite cell pools and myonuclear reserves. His emphasis on recovery—including 9 hours of sleep nightly, deep-tissue massage, hydration (half his body weight in ounces of water daily), and anti-inflammatory nutrition—created the optimal environment for maintaining muscle plasticity into his mid-40s.
Staying injury-free is crucial for long-term success, and incorporating pliability contributes to an athlete's longevity and performance on the field, notes the TB12 Method documentation. Brady's ability to play 23 seasons—outlasting the typical NFL career by nearly 20 years—demonstrates that prioritizing recovery and maintaining cellular recovery capacity can extend peak performance far beyond normal expectations.
The lesson for non-elite athletes is clear: you don't need to train like you're 25 to maintain capacity at 45. Strategic recovery, inflammation management, and preserving cellular infrastructure matter more than maximum intensity training as we age.
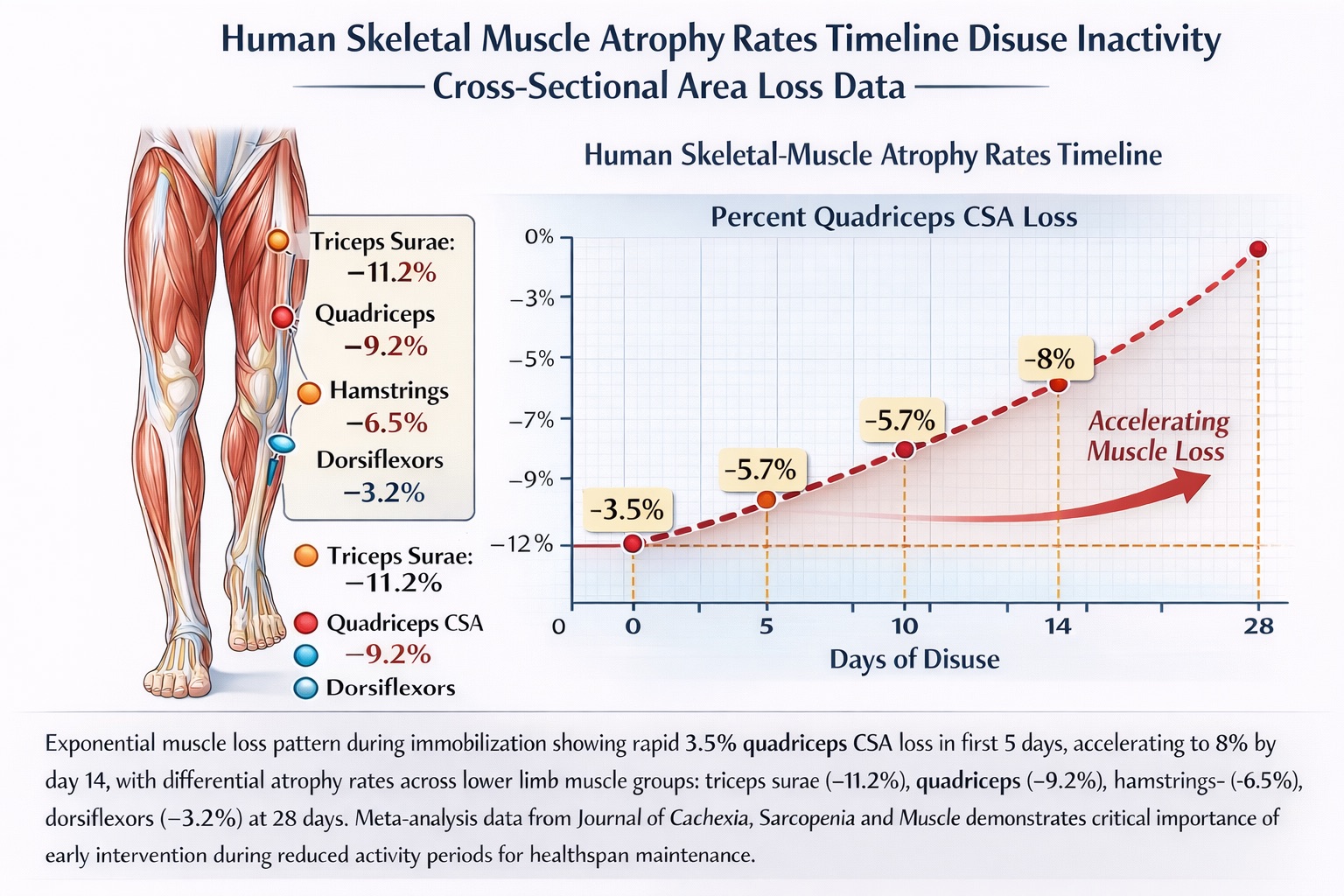
Exponential muscle loss pattern during immobilization showing rapid 3.5% quadriceps CSA loss in first 5 days, accelerating to 8% by day 14, with differential atrophy rates across lower limb muscle groups: triceps surae (-11.2%), quadriceps (-9.2%), hamstrings (-6.5%), dorsiflexors (-3.2%) at 28 days. Meta-analysis data from Journal of Cachexia, Sarcopenia and Muscle demonstrates critical importance of early intervention during reduced activity periods for healthspan maintenance.
The Alarming Speed of Muscle Loss: Understanding What We're Up Against
To fully appreciate the power of muscle memory, we must first confront the sobering reality of disuse atrophy. The data reveals just how quickly our bodies can lose hard-won gains.
The rate of muscle atrophy from disuse (10-42 days) is approximately 0.5-0.6% of total muscle mass per day, though considerable variation exists between individuals. This means that in just two weeks of complete inactivity, you could lose 7-8.4% of your muscle mass. The mathematics are unforgiving: a month of bedrest could cost you 15-18% of your muscle tissue.
But the losses aren't uniform across all muscles. Rates of atrophy vary significantly between muscle groups, with the greatest losses in triceps surae (-11.2% at day 28), followed by quadriceps (-9.2% at day 28), hamstrings (-6.5% at day 28), and foot dorsiflexors (-3.2% at day 28). This differential vulnerability suggests that some muscles are more atrophy-susceptible while others demonstrate greater resistance—knowledge that can inform targeted intervention strategies.
More concerning still, the greatest losses occur in the first 14 days, with rates following a pattern of exponential decay before slowing over time to reach an eventual nadir. This acute phase of rapid atrophy underscores why early intervention during periods of reduced activity is critical.
The Specific Case: Five Days That Change Everything
Consider the stark findings from van Loon's laboratory at Maastricht University. Five days of immobilization led to 3.5% reduction in quadriceps cross-sectional area (CSA) and 9% loss in muscle strength. By 14 days, these losses had progressed to 8% reduction in CSA and 23% reduction in quadriceps strength.
The disproportionate loss of strength relative to size reveals that muscle function deteriorates faster than muscle mass—a critical distinction for understanding recovery priorities. Strength depends not just on muscle size but on neural drive, motor unit recruitment, and muscle fiber architecture. All three systems begin deteriorating within days of reduced activity.
The Critical Care Crisis: When Muscle Loss Becomes Life-Threatening
The most extreme—and clinically significant—examples of disuse atrophy occur in intensive care unit (ICU) settings, where the convergence of illness, inflammation, immobilization, and metabolic stress creates a perfect storm for muscle wasting.
Critically ill patients experience a significant loss of nearly 2% of skeletal muscle per day during the first week of ICU admission—approximately 3-4 times faster than healthy individuals experiencing simple immobilization. Over just one week, this translates to a catastrophic 14% loss of muscle mass, with some patients losing up to 30% by day 14.
The consequences extend far beyond the ICU stay. At least 50% of ICU patients report inability to return to work due to fatigue, weakness, or overall impaired functional status one year after their critical care stay. Even more troubling, a predominant feature in ICU survivors is reduced muscle strength, mass, and physical function, leading to lower exercise capacity, long-lasting physical disability, higher mortality risk, and subsequent health costs.
The Six-Month Reality: When Recovery Plateaus
Groundbreaking longitudinal research published in the American Journal of Respiratory and Critical Care Medicine tracked ICU survivors over six months post-discharge. Persistent muscle weakness following resolution of critical illness is associated with markedly variable combinations of muscle atrophy and impaired voluntary contractile capacity.
The study revealed that patients who failed to recover muscle mass demonstrated lower quadriceps satellite cell content compared with those patients who recovered muscle mass, with the diminished satellite cell content potentially playing a causative role in poor muscle regrowth and sustained atrophy.
This finding illuminates a crucial mechanism: satellite cells—the muscle stem cells responsible for repair and regeneration—become depleted in some patients. Without adequate satellite cell reserves, muscles cannot recruit the myonuclei needed for regrowth, creating a vicious cycle where recovery becomes increasingly difficult over time.
The implications for longevity planning are profound. Maintaining satellite cell pools through consistent physical activity across the lifespan isn't just about immediate fitness—it's about preserving regenerative capacity for future recovery needs.
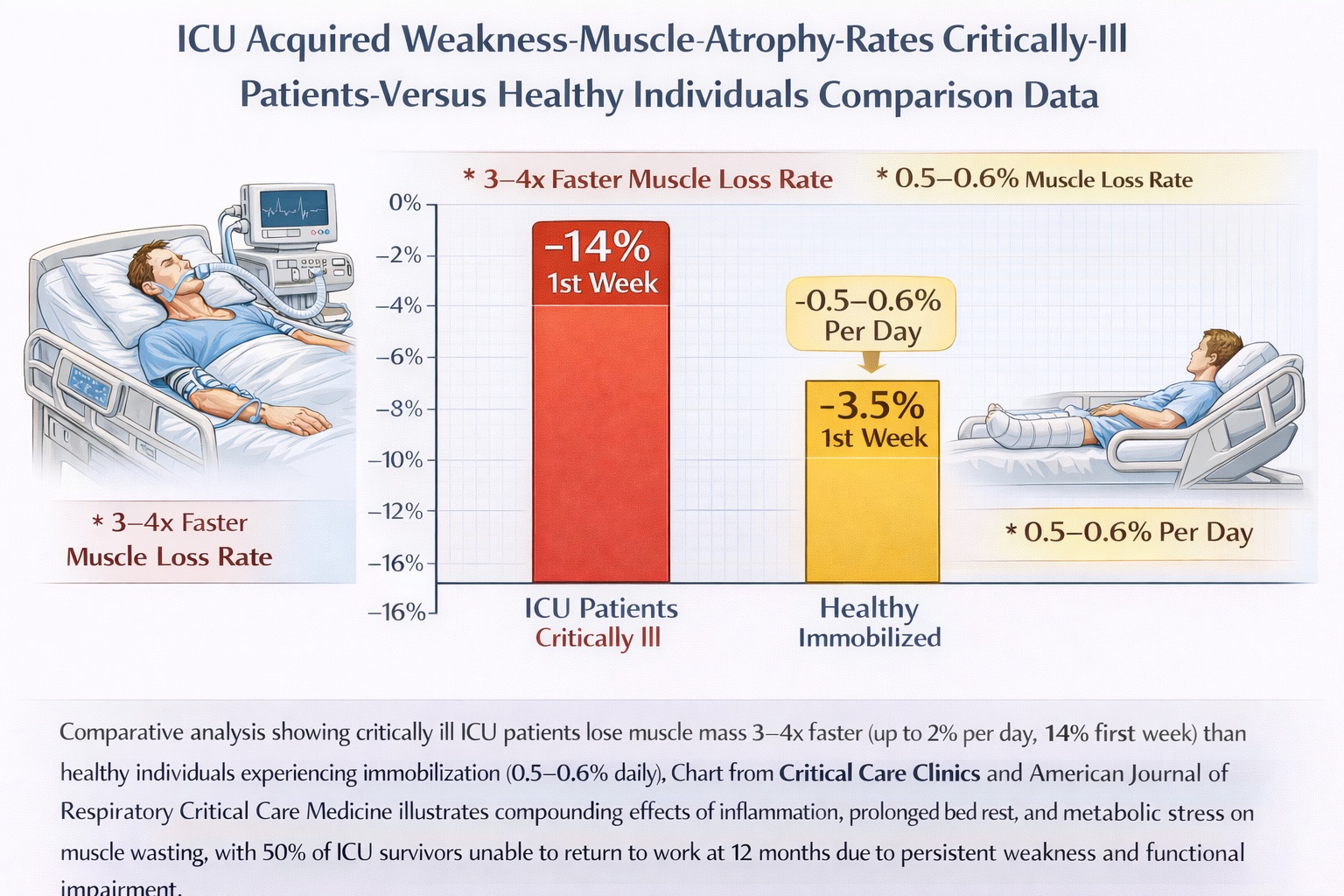
Comparative analysis showing critically ill ICU patients lose muscle mass 3-4x faster (up to 2% per day, 14% first week) than healthy individuals experiencing immobilization (0.5-0.6% daily). A chart from Critical Care Clinics and the American Journal of Respiratory Critical Care Medicine illustrates the compounding effects of inflammation, prolonged bed rest, and metabolic stress on muscle wasting, with 50% of ICU survivors unable to return to work at 12 months due to persistent weakness and functional impairment.
The Dual Mechanisms: Cellular and Epigenetic Memory
The science of muscle recovery points to two interconnected systems working in tandem to preserve muscle capacity even after significant atrophy.
Cellular Memory: The Myonuclear Domain Theory
Skeletal muscle cells, called myocytes, are unique among human cells in possessing hundreds of nuclei. As muscles expand, additional nuclei are incorporated into the pre-existing muscle fiber, which originate from activated satellite cells in the surrounding area.
The groundbreaking 2024 research by Kristoffer Toldnes Cumming and colleagues at Østfold University College provides the most definitive human evidence to date. Following 10 weeks of unilateral elbow-flexor strength training followed by 16 weeks of detraining, myonuclei increased in type 1 fibers by 13% and type 2 fibers by 33%, with the sustained higher number of myonuclei confirming myonuclear accretion and permanence in humans.
Professor Adam P. Sharples from the Norwegian School of Sport Sciences explains the significance: Having more of these control centers can basically cause more rapid adaptation the second time around when you resume training after a break.
The myonuclear domain theory posits that each nucleus governs a specific volume of cytoplasm within the muscle fiber. When you build muscle, you're not just making fibers bigger—you're fundamentally reorganizing the cellular architecture by adding control centers that persist even when the muscle shrinks. These retained nuclei can then rapidly upregulate protein synthesis when training resumes, bypassing the slow process of satellite cell recruitment and fusion that occurs during initial muscle building.
Epigenetic Memory: DNA Methylation Changes That Endure
The second mechanism operates at an even deeper level—in the regulatory switches that control gene expression. Human skeletal muscle possesses an epigenetic memory characterized by retained hypomethylation and increased gene expression after training into long-term detraining and retraining.
In groundbreaking 2024 research published in the American Journal of Physiology-Cell Physiology, Andrea M. Pilotto and colleagues from the University of Pavia examined high-intensity interval training effects. Twenty healthy subjects completed two training interventions lasting 2 months, separated by 3 months of detraining. Thousands of differentially methylated positions predominantly demonstrated a hypomethylated state after training, retained even after 3 months of exercise cessation.
Five specific genes—ADAM19, INPP5a, MTHFD1L, CAPN2, and SLC16A3—showed particularly robust memory profiles. These genes are involved in lactate transport, calcium signaling, and metabolic regulation. Retained hypomethylation was associated with enhanced expression of the same genes even after 3 months of detraining.
Think of DNA methylation as molecular Post-It notes on your genes. Training removes these notes from specific genes involved in muscle adaptation, leaving them primed for easier activation in the future. Even after months of inactivity, many of these notes stay removed, allowing the genes to respond more quickly when you resume training.
Professor Simone Porcelli from the University of Pavia notes that this epigenetic memory represents a form of molecular learning—the muscle literally learns how to adapt to exercise, and retains that knowledge at the chromosomal level.
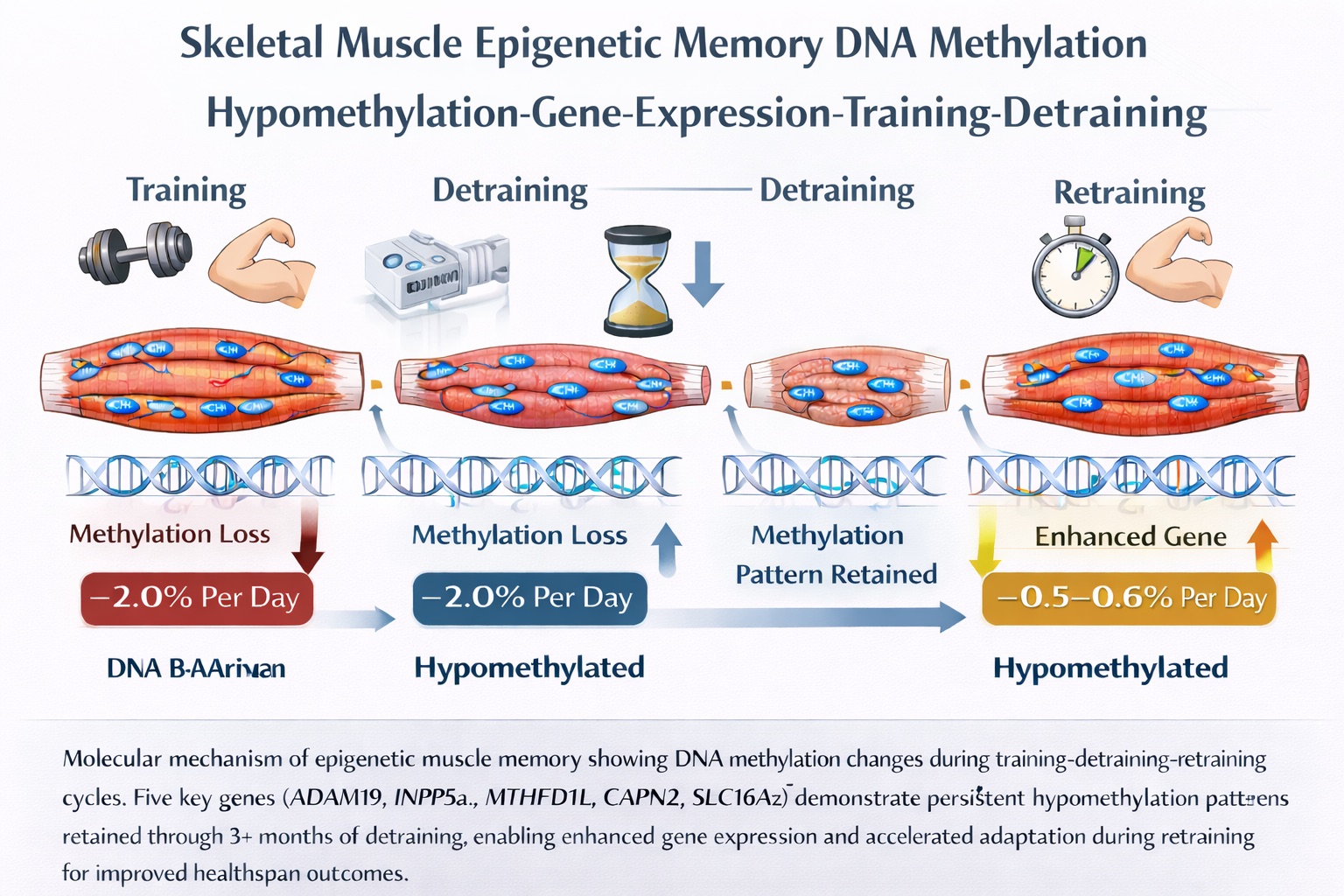
Molecular mechanism of epigenetic muscle memory showing DNA methylation changes during training-detraining-retraining cycles. Five key genes (ADAM19, INPP5a, MTHFD1L, CAPN2, SLC16A3) demonstrate persistent hypomethylation patterns retained through 3+ months of detraining, enabling enhanced gene expression and accelerated adaptation during retraining for improved healthspan outcomes.
The Finnish Study: Definitive Proof of Muscle Memory in Action
The most comprehensive examination of muscle memory in humans comes from the University of Jyväskylä in Finland, where Juha P. Ahtiainen and Eeli J. Halonen led a 30-week investigation comparing continuous versus periodic resistance training.
Fifty-five healthy untrained participants were randomized to either periodic resistance training (PRT)—completing 10 weeks of training, 10 weeks of detraining, then 10 more weeks of retraining—or continuous resistance training (CRT) for 20 weeks straight.
The results were striking: After 10 weeks of RT followed by detraining, the PRT group experienced greater gains during the first 5 weeks of the second 10-week RT period than the CRT group during its second RT period immediately after 10 weeks of RT.
Even more remarkably, muscle strength and size were regained faster during retraining than they were initially gained during the first training period. The PRT group, despite their 10-week break, ultimately achieved identical outcomes to the continuous training group by the end of 30 weeks.
The Five-Week Window: Accelerated Retraining Phenomenon
The most dramatic differences appeared in the first five weeks of retraining. During retraining, the PRT group exhibited faster gains in strength and muscle size than the CRT group during the same stage of continuous training.
Specifically, during the second 10-week period, changes in the PRT group were significantly greater than the CRT group: leg press 1RM increased 12.2% vs. 5.9%, vastus lateralis CSA increased 15.1% vs. 3.3%, and biceps brachii CSA increased 15.1% vs. 6.8%. The PRT group was experiencing muscle growth at more than double the rate of continuous trainers who had no break.
Dr. Kevin Murach from the University of Arkansas explains the implications: People tend to overestimate how much they need to do to maintain their muscle mass, and a little bit of exercise can go a pretty long way in maintaining function and size.
This finding fundamentally challenges the "never miss a workout" mentality that pervades fitness culture. Strategic breaks may not just be acceptable—they might actually optimize long-term progress by preventing chronic training stress and potentially resensitizing muscle fibers to anabolic stimuli.
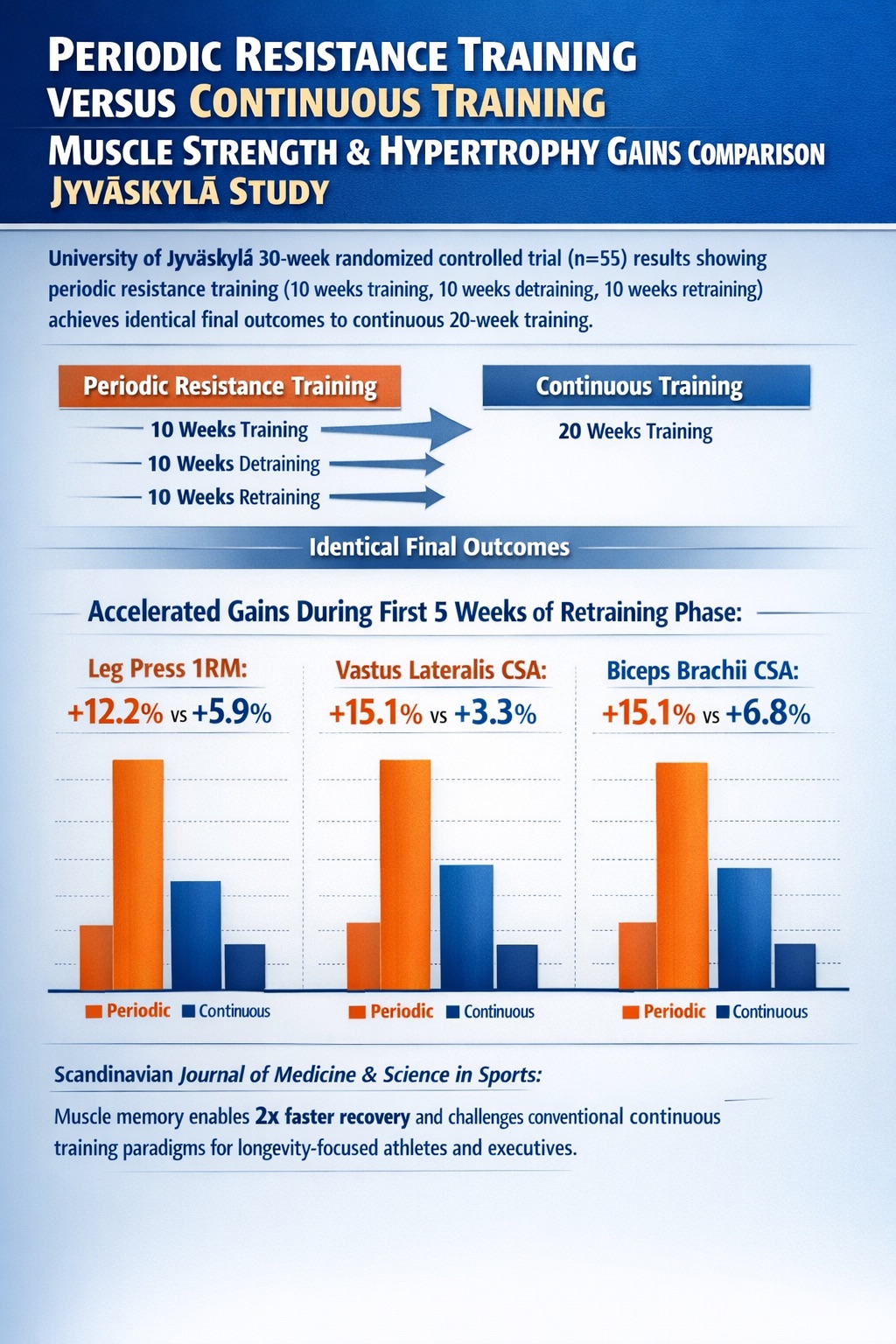
University of Jyväskylä 30-week randomized controlled trial (n=55) results showing periodic resistance training (10 weeks training, 10 weeks detraining, 10 weeks retraining) achieves identical final outcomes to continuous 20-week training*, with significantly accelerated gains during first 5 weeks of retraining phase: leg press 1RM (+12.2% vs +5.9%), vastus lateralis CSA (+15.1% vs +3.3%), biceps brachii CSA (+15.1% vs +6.8%). Scandinavian Journal of Medicine & Science in Sports data demonstrates muscle memory enables 2x faster recovery and challenges conventional continuous training paradigms for longevity-focused athletes and executives.*
Age-Related Impairment: When Recovery Becomes Harder
Perhaps the most clinically important finding in muscle memory research is the differential recovery capacity between young and older adults. Research by Charlotte Suetta and colleagues revealed a troubling pattern: Following 2 weeks of unilateral leg casting and subsequent intensive resistance training, older adults were not able to fully recover losses of skeletal muscle in comparison to young adults who demonstrated full recovery of quadriceps cross-sectional area.
This age-related impairment in recovery capacity isn't just about slower progress—it represents incomplete recovery even with optimal rehabilitation. Some older adults never fully regain what they've lost, creating a downward spiral where each period of inactivity results in permanent net loss.
The mechanisms underlying this age-related decline are multifactorial. Older adults demonstrate:
- Reduced satellite cell reserves and proliferative capacity
- Anabolic resistance (diminished response to protein intake and exercise)
- Chronic low-grade inflammation that promotes catabolism
- Mitochondrial dysfunction affects energy availability for protein synthesis
- Hormonal changes reduce growth signaling
This underscores why maintaining muscle mass becomes exponentially more important with age. Every decade of consistent training builds not just current capacity but future recovery potential. The myonuclei you accumulate in your 30s and 40s may determine whether you can recover from illness or injury in your 70s and 80s.
The Negative Memory Problem: Repeated Wasting and Permanent Loss
There's a darker side to muscle plasticity. Repeated muscle wasting is a clinically relevant issue, especially in elderly populations, where, after an injury and consequent disuse, individuals lose muscle and become weaker and are more likely to suffer a repeated fall injury that may result in further muscle loss in the future.
This concept of "negative muscle memory"—where repeated periods of atrophy may lead to permanent loss of myonuclei and diminished recovery capacity—explains why prevention strategies are paramount. It's not enough to recover once; we must prevent the accumulation of negative adaptations over time.
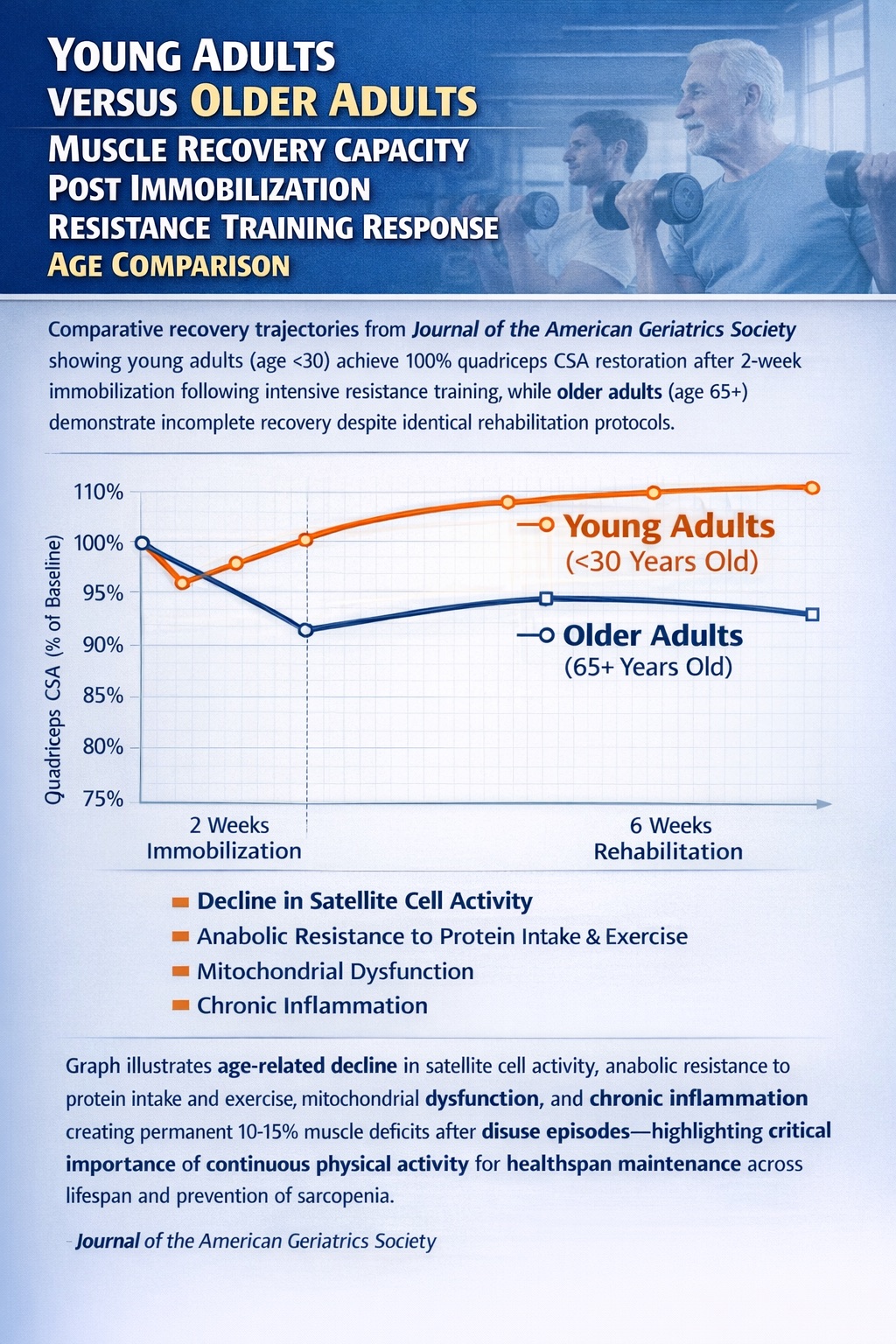
Comparative recovery trajectories from Journal of the American Geriatrics Society showing young adults (age <30) achieve 100% quadriceps CSA restoration after 2-week immobilization following intensive resistance training, while older adults (age 65+) demonstrate incomplete recovery despite identical rehabilitation protocols. Graph illustrates age-related decline in satellite cell activity, anabolic resistance to protein intake and exercise, mitochondrial dysfunction, and chronic inflammation, creating permanent 10-15% muscle deficits after disuse episodes—highlighting the critical importance of continuous physical activity for healthspan maintenance across lifespan and prevention of sarcopenia.
Beyond Recovery: Novel Therapeutic Approaches
Emerging research is exploring unconventional approaches to accelerate muscle recovery after injury or periods of inactivity.
Hypoxia and Cold: Unexpected Recovery Accelerators
A fascinating 2024 study from the University of Barcelona's Department of Cell Biology, Physiology and Immunology investigated intermittent exposure to hypobaric hypoxia (simulated altitude) combined with cold as a strategy to improve and accelerate recovery from muscle injuries.
Lead researcher Garoa Santocildes and colleagues discovered that hypobaric chambers, long used to improve physical fitness in high-performance sports, create conditions where the body is exposed to low atmospheric pressure and cells take up less oxygen, generating a physiological response that accelerates injured skeletal muscle recovery.
The mechanism involves triggering the hypoxia-inducible factor (HIF) pathway, which upregulates angiogenesis (new blood vessel formation), stem cell mobilization, and tissue remodeling. When combined with cold exposure, which reduces inflammation and may preserve myonuclear content, the dual stimulus creates an enhanced recovery environment.
AI-Powered Longevity Planning: From Theory to Personalized Practice
The convergence of muscle plasticity science with AI-driven diagnostics is creating unprecedented opportunities for personalized longevity optimization.
TruDiagnostic: Epigenetic Insights Meet Recovery Science
TruDiagnostic, a Kentucky-based epigenetics company, is pioneering the translation of muscle memory science into actionable health insights. In June 2024, TruDiagnostic launched the first-ever epigenetic aging analysis of individual organ systems using validated and system-specific trained clocks called SYMPHONYAge.
Developed by scientists at Yale University, SYMPHONYAge provides a new way of looking at aging by examining how different parts of the body decline independently and synchronously over time, with organ systems aging differently in a single body based on lifestyle and dietary choices.
Dr. Albert Higgins Chen from Yale explains: Arthritis is the result of both musculoskeletal wear and inflammation, whereas stroke can happen due to problems in the cardiovascular system, metabolism, inflammation, and brain function, with interconnected patterns leading to different aging types and making some people more prone to certain age-related diseases.
In October 2024, TruDiagnostic and Yale released landmark research analyzing the impact of 51 different longevity interventions spanning diet, exercise, pharmacological, and therapeutic modifications on 110 biomarkers. The findings validated that their GenX clocks, including OMICmAge (developed with Harvard) and SymphonyAge, are the most responsive aging clocks available.
TruDiagnostic's partnership with Weill Cornell Medicine has uncovered even deeper mechanisms. Researchers uncovered DNA markers associated with retroelements—remnants of ancient viral genetic material—that may be involved in aging and act as highly accurate epigenetic clocks predicting chronological age.
Dr. Lishomwa Ndhlovu and Dr. Michael Corley found that the reactivation of specific retroelements increases with age, potentially leading to biological hallmarks of aging such as inflammation, cellular senescence and genomic instability.
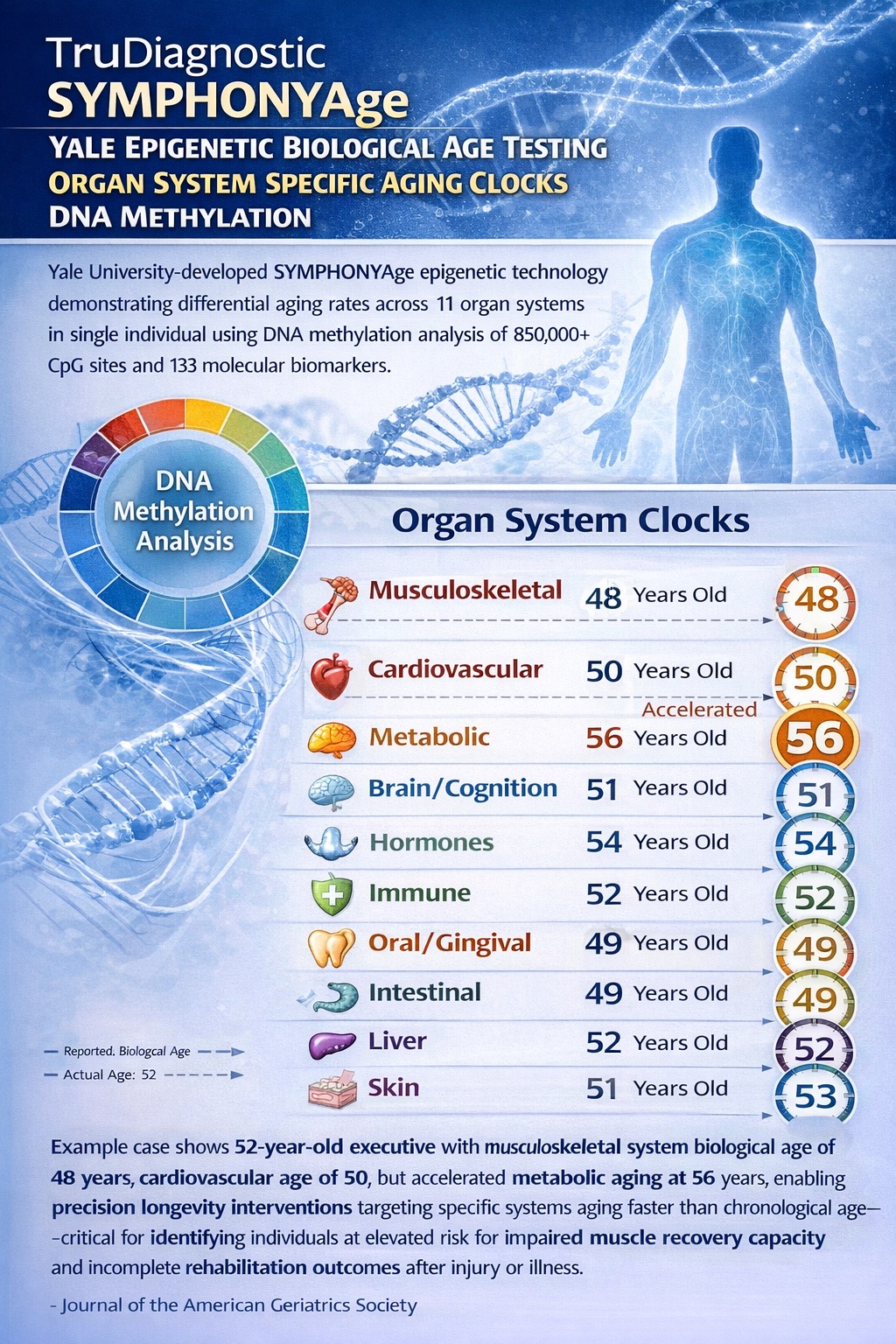
Yale University-developed SYMPHONYAge epigenetic technology demonstrating differential aging rates across 11 organ systems in single individual using DNA methylation analysis of 850,000+ CpG sites and 133 molecular biomarkers. Example case shows 52-year-old executive with musculoskeletal system biological age of 48 years, cardiovascular age of 50, but accelerated metabolic aging at 56 years, enabling precision longevity interventions targeting specific systems aging faster than chronological age—critical for identifying individuals at elevated risk for impaired muscle recovery capacity and incomplete rehabilitation outcomes after injury or illness.
Fountain Life: Comprehensive Diagnostics Meet Precision Recovery Planning
Fountain Life—co-founded by Peter Diamandis, Tony Robbins, and Dr. Bill Kapp—is integrating advanced AI with comprehensive diagnostics to detect disease before symptoms appear and optimize recovery capacity.
The APEX diagnostic program gathers more than 150GB of data to determine whether you currently have or are at risk for developing any of the leading causes of shortened health and lifespan, specifically cardiovascular disease, cancer, aneurysms, metabolic disease, and neurocognitive dysfunction.
Peter Diamandis emphasizes the hidden nature of disease progression: 70% of all heart attacks have no precedent, 70% of all fatal cancers result from cancers not routinely tested for, and individuals with Parkinson's don't develop tremors until nearly 70% of the substantia nigra neurons are gone.
In August 2024, Fountain Life raised an $18 million Series B round to expand its network of longevity centers. CEO Dr. Bill Kapp notes that by definition, if you're asymptomatic, the current health system tells you you're healthy, but the data shows that's not true.
Peter Diamandis is also the founder and executive chairman of the XPRIZE Foundation, which launched the $101 million XPRIZE Healthspan in 2023. Competitors are tasked with finding a therapeutic that can reverse the loss of function in three key bodily systems—muscle, immune system and cognition—with the ultimate goal of adding an extra 10-20 healthy years to a person's life.

Fountain Life's AI-integrated APEX diagnostic platform combines full-body MRI imaging, coronary CT angiography, advanced blood biomarker panels (150+ markers), whole genome sequencing, microbiome analysis, and metabolomics, generating 150+ gigabytes of individualized health data per member. Visual representation of multi-modal data integration pipeline using artificial intelligence and machine learning for early disease detection before symptom manifestation, enabling identification of subclinical muscle loss, metabolic dysfunction, cardiovascular disease, cancer, and neurodegenerative conditions—supporting proactive longevity planning and muscle memory preservation strategies for high-performing executives and athletes.
Practical Applications: Evidence-Based Strategies
Based on a comprehensive review of current research, here are evidence-based strategies for leveraging muscle plasticity mechanisms:
1. Build Myonuclear Reserves Early
For individuals under 50, the primary goal should be maximizing myonuclear accretion through progressive resistance training. Implementation: 3-4 sessions weekly, emphasizing mechanical tension (heavy loads, 6-12 reps) and metabolic stress (higher reps with shorter rest).
2. Embrace Strategic Periodization
The Finnish research demonstrates that periodic breaks don't compromise long-term adaptations. Consider 8-week intensive training blocks followed by 1-2 week recovery phases, especially during demanding life periods.
3. Prioritize Recovery With Age
As recovery capacity declines, shift focus from maximum intensity to optimal recovery. Follow Tom Brady's example: prioritize sleep (8-9 hours), hydration, anti-inflammatory nutrition, and active recovery over maximum training volume.
4. Monitor Biological Age
Use epigenetic testing from companies like TruDiagnostic to track musculoskeletal aging specifically. Early detection of accelerated aging enables intervention before permanent capacity loss.
5. Prevent Negative Cycles
For older adults, preventing disuse is more important than optimizing training. Even modest activity (2 resistance sessions weekly) can maintain myonuclear pools and prevent the downward spiral of repeated atrophy.
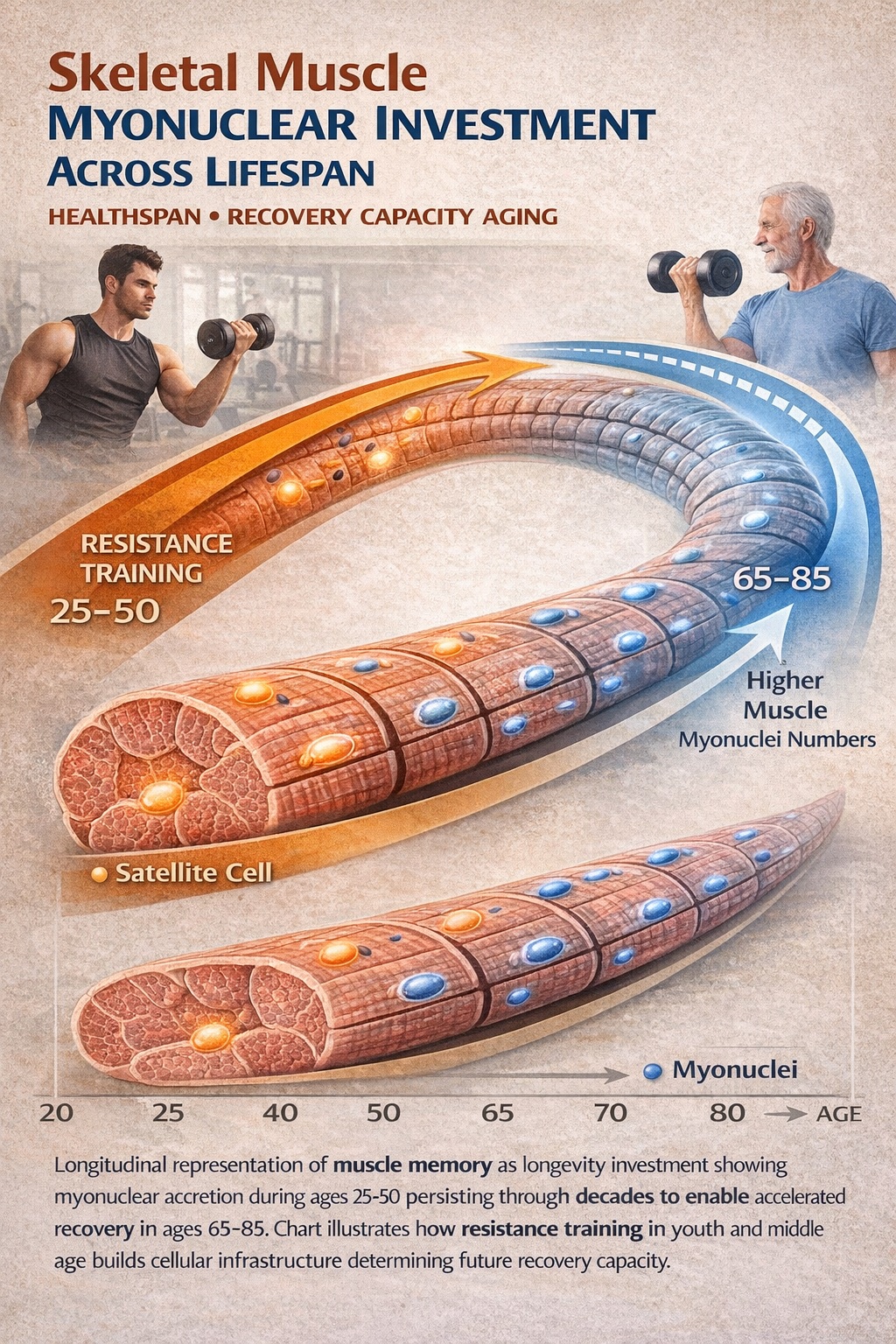
Longitudinal representation of muscle memory as longevity investment showing myonuclear accretion during ages 25-50, persisting through decades to enable accelerated recovery in ages 65-85. The chart illustrates how resistance training in youth and middle age builds cellular infrastructure, determining future recovery capacity.
Conclusion: Memory as a Longevity Strategy
The science of muscle memory reveals something profound about human biology: we are designed for resilience. The cellular machinery we build through training doesn't disappear the moment we stop—it persists, waiting to be reactivated.
As Professor Adam Sharples and his colleagues have shown, skeletal muscle memory represents an important consideration for optimizing exercise interventions and training programs as well as the development of therapeutic strategies for counteracting muscle-wasting conditions and age-related muscle loss.
For those serious about longevity—whether elite athletes like Tom Brady, successful executives, or simply individuals committed to living well in their later decades—understanding and leveraging muscle plasticity isn't optional. It's a foundational principle of healthspan extension.
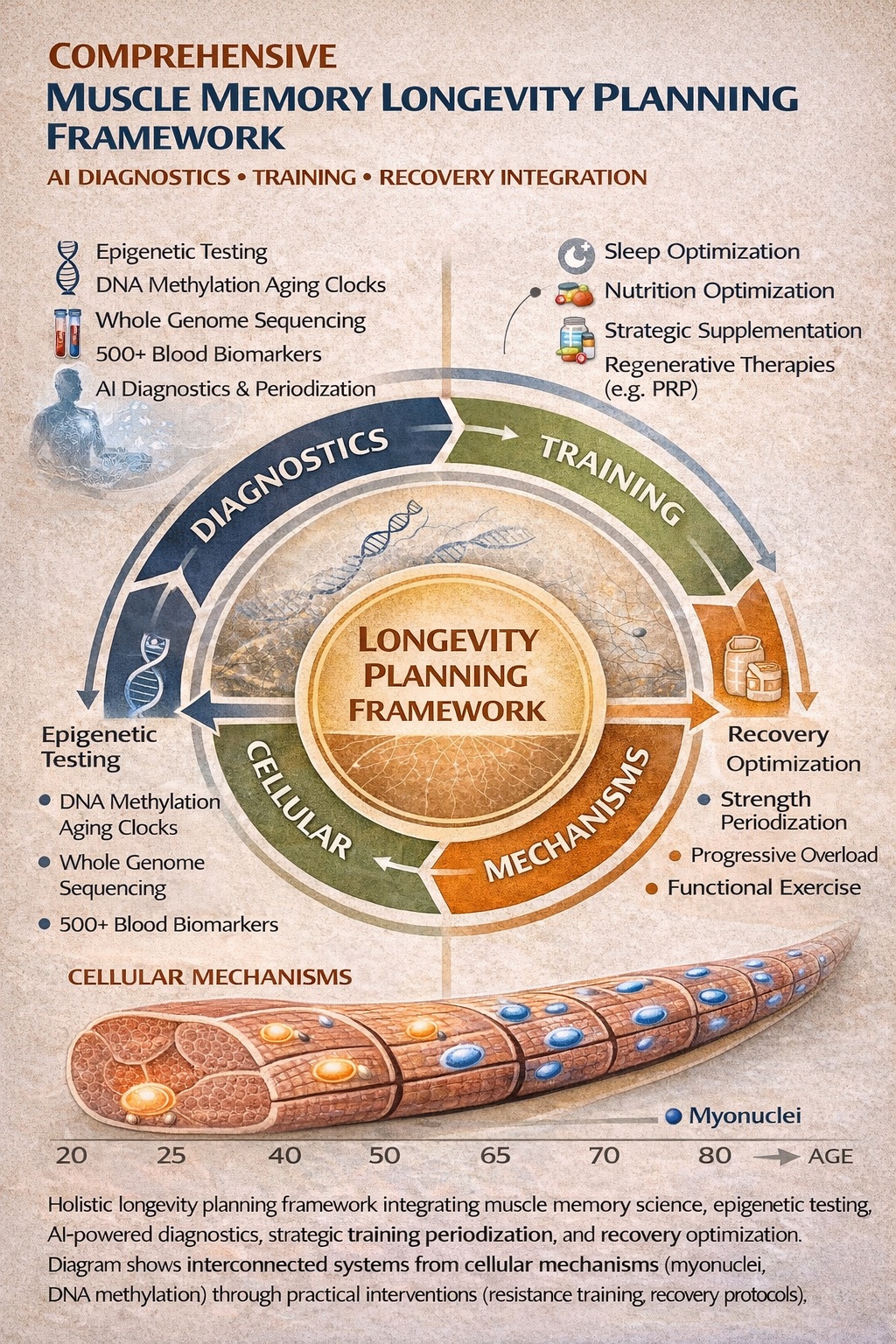
Holistic longevity planning framework integrating muscle memory science, epigenetic testing, AI-powered diagnostics, strategic training periodization, and recovery optimization. The diagram shows interconnected systems from cellular mechanisms (myonuclei, DNA methylation) through practical interventions (resistance training, recovery protocols) to long-term healthspan outcomes.
About the Authors
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a 3x IRONMAN Triathlon (140.6 mi) Finisher, and 3x tech CEO with 2 successful exits. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University.
Molly Bunting is a senior at Boston University, majoring in Biology with a minor in Business Administration and Management. Her experience spans biomedical research, clinical medicine, hospital laboratory operations, and international health systems. She will graduate in Spring 2026 and is interested in careers spanning biodefense, pharmaceutical R&D, and medicine.