Longevity
·18 min read
The Longevity Divide
How Geography, Income, and Access to Data-Driven Medicine Are Creating Two Worlds of Human Healthspan
By Tony Medrano, Sarah Wang, Joël Christoph, Mary Mugambi, Maison Kipila & Reward Muzerengwa

Introduction: The Decade You Spend Dying
Consider a sobering reality: the average human being will spend nearly ten years of their life burdened by disease or disability before death. A landmark 2024 study published in JAMA Network Open by Mayo Clinic researchers Garmany and Terzic quantified what they call the 'healthspan-lifespan gap' across 183 World Health Organization member nations. Unfortunately, this gap has widened to 9.6 years—a 13 percent increase since 2000.
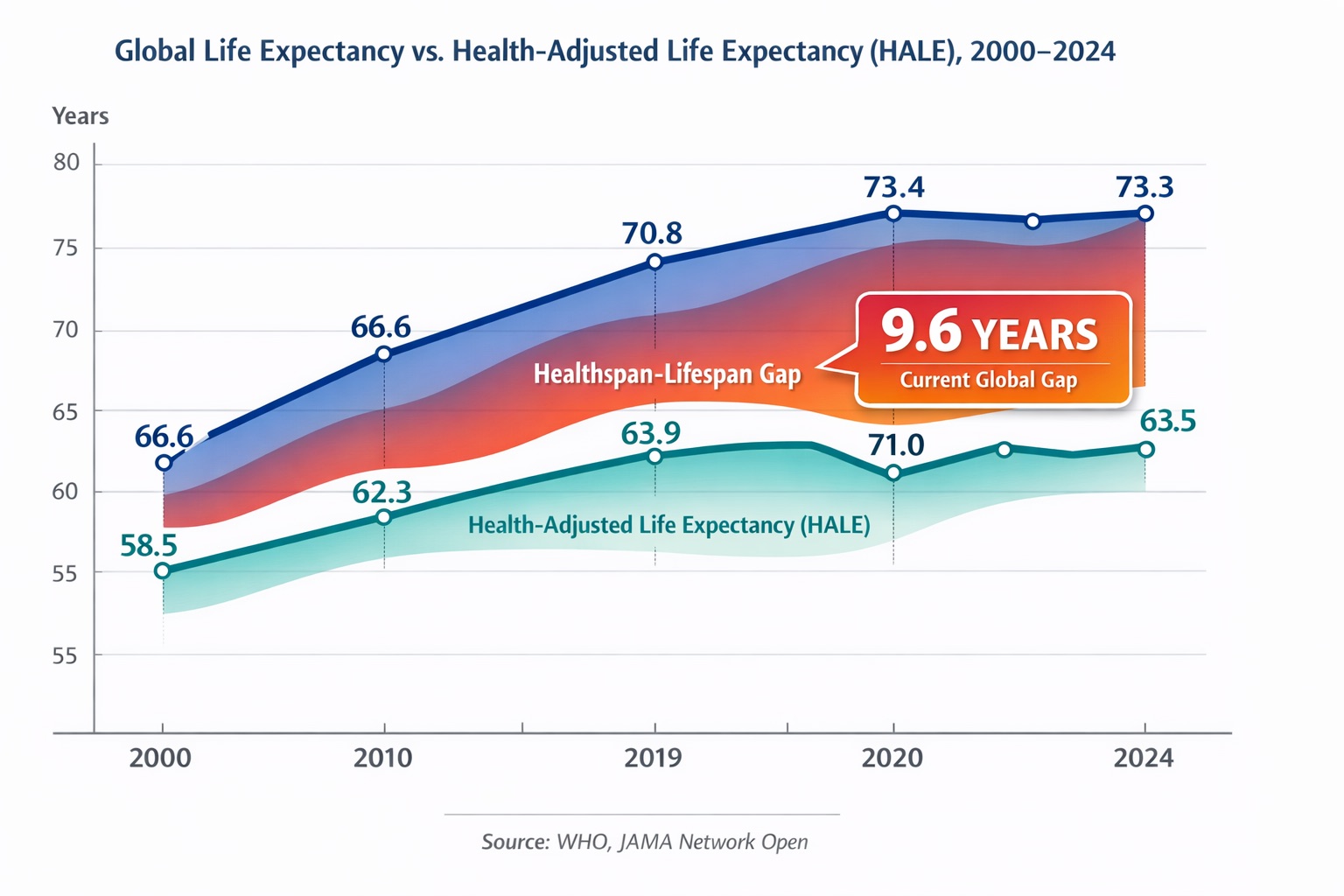
Figure 1: The global healthspan-lifespan gap has widened to 9.6 years as of 2024—meaning the average person will spend nearly a decade of life burdened by disease or disability. Data source: WHO Global Health Observatory; Garmany & Terzic, JAMA Network Open 2024.
If you are an American woman, your gap is significantly worse. Between 2000 and 2019, while U.S. female life expectancy inched up from 79.2 to 80.7 years, health-adjusted life expectancy remained virtually stagnant. The result? The final 12.4 years of the average American woman's life will be impacted by disease or disability, which is 29 percent higher than the global average.
This article examines why such disparities exist, what the science reveals about extending healthspan (not just lifespan), and how a new generation of precision technologies—from wearable biosensors to epigenetic clocks to AI-powered digital twins—is beginning to democratize what was once available only to elite athletes and billionaires.
Part I: The Geography of Dying
Life expectancy is not distributed evenly across the planet. According to the United Nations World Population Prospects 2024, a child born today in Western Europe can expect to live to 82.7 years. A child born in Western Africa can expect 57.7 years—a gap of 25 years, or roughly one-third of an entire human life.
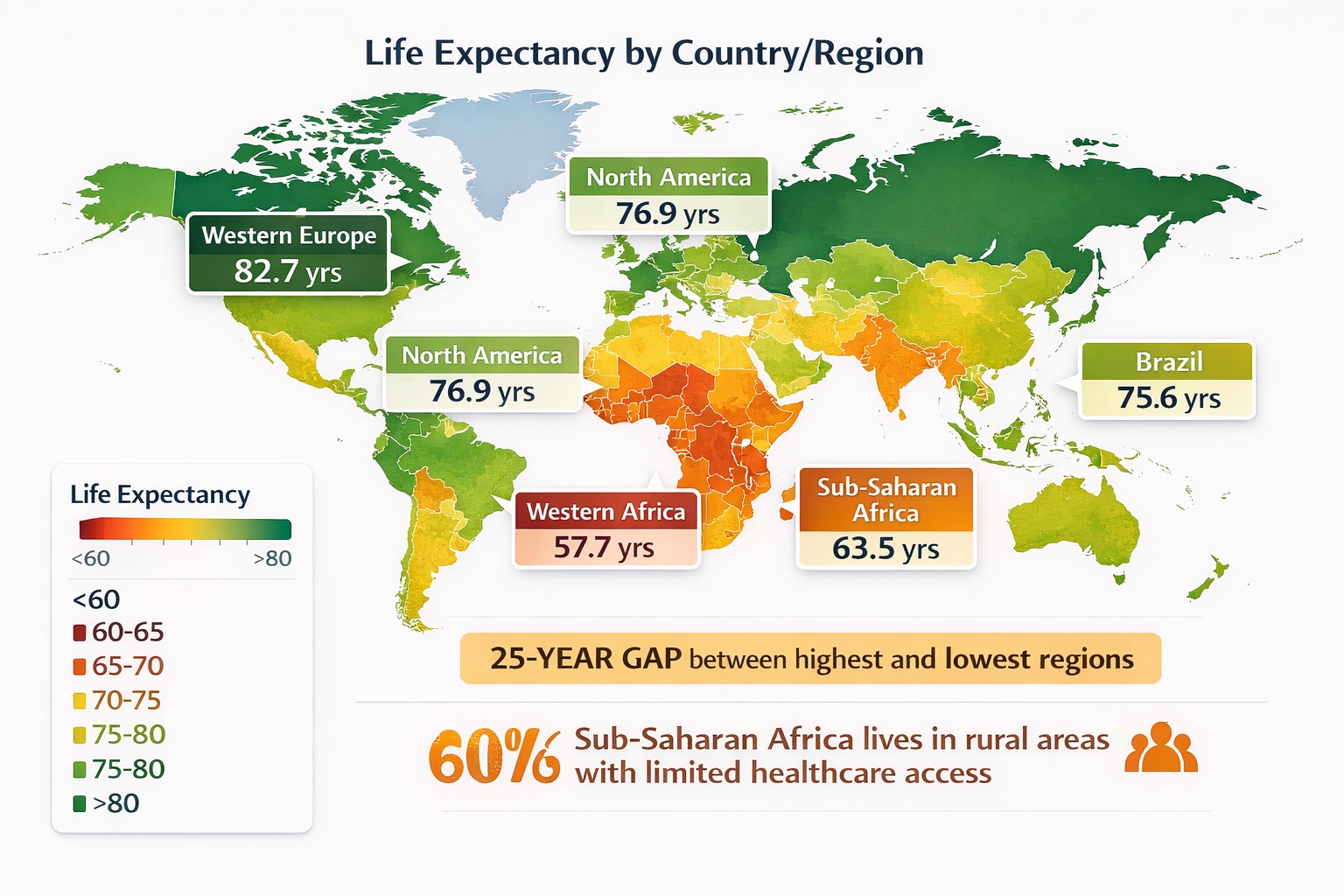
Figure 2: Life expectancy varies by up to 25 years between Western Europe (82.7 years) and Western Africa (57.7 years). This geographic lottery determines one-third of a human lifespan before a child draws their first breath. Data source: UN World Population Prospects 2024.
The reasons are structural and systemic. Sub-Saharan Africa carries 24-25 percent of the global disease burden while possessing only 3 percent of the world's healthcare workforce. More than 60 percent of the population lives in rural areas with limited access to basic medical infrastructure. Dr. Christopher Murray, Director of the Institute for Health Metrics and Evaluation at the University of Washington, said, "Health disparities are the norm, not the exception. What's remarkable is the size of these disparities, even on a global scale."
The US-Brazil Paradox
Perhaps more instructive than the US-Africa comparison is the US-Brazil comparison. The United States has a GDP per capita roughly five times that of Brazil. Yet life expectancy differs by only about one year (76.9 vs. 75.6-76 years). This data point demolishes the assumption that wealth automatically translates to longevity. Brazil's relative success stems from universal healthcare coverage, strong public health infrastructure, and lower rates of the chronic diseases that plague affluent Western nations of obesity, cardiovascular disease, and metabolic syndrome.
The 20-Year Gap Within America
Within the United States, life expectancy varies by up to 20 years depending on race and geography. According to Institute for Health Metrics and Evaluation data, Black Americans in the rural South and segregated urban centers had life expectancies as low as 70.5 years in 2000. Asian Americans in high-income coastal areas averaged 83.1 years—a gap equivalent to living in two different centuries of human development.
COVID-19 exposed and amplified these inequities. Between 2019 and 2020, Black Americans lost 4.0 years of life expectancy compared to 1.4 years for other groups. The pandemic didn't create these disparities; it revealed them with brutal clarity.
Part II: How Do We Actually Measure Healthspan?
Before we can close the healthspan gap, we must understand how it's measured. The gold standard is the World Health Organization's Health-Adjusted Life Expectancy (HALE), defined as "the average number of years that a person can expect to live in full health, taking into account years lived in less than full health due to disease and/or injury."
HALE uses Sullivan's method, which combines mortality data with disability weights from the Global Burden of Disease study. It's powerful but population-level—useful for comparing countries, possibly less useful for guiding individual health decisions. The WHO's 2024 data shows that prior to COVID-19, global HALE increased from 58.1 years in 2000 to 63.5 years in 2019, but this gain (5.3 years) lagged behind the life expectancy increase (6.4 years). We are adding years to life faster than we are adding life to years.
The Rise of Biological Age Testing
For individuals seeking to optimize their own healthspan, population metrics are insufficient. What matters is biological age—how old your cells and systems are compared to your chronological age. This is where epigenetic clocks get into the picture.
The most validated of these clocks is DunedinPACE, developed through a collaboration between Duke University and the University of Otago, based on longitudinal data from the Dunedin Multidisciplinary Health and Development Study. It's a remarkable cohort that has tracked 1,037 individuals born in 1972-1973 from birth through middle age. Unlike earlier clocks that predict chronological age, DunedinPACE measures the pace of aging—how quickly or slowly your body is aging right now.
Published in eLife in 2022, DunedinPACE demonstrated high test-retest reliability and significant associations with morbidity, disability, and mortality independent of other epigenetic clocks like GrimAge. Companies like TruDiagnostic now offer DunedinPACE testing commercially, analyzing over 900,000 methylation markers to generate a single number: your pace of aging relative to one calendar year. A result of 0.8 means your body is aging 0.8 years for every chronological year that passes, a meaningful advantage compounding over decades.
Part III: VO2 Max—The Single Strongest Predictor of How Long You will Live
If you had to pick one metric to predict longevity, it wouldn't be cholesterol, blood pressure, or body mass index. It would be cardiorespiratory fitness, typically measured as VO2 max—the maximum amount of oxygen your body can utilize during intense exercise, expressed in milliliters per kilogram of body weight per minute.
The evidence is overwhelming. A 2018 study published in JAMA Network Open by researchers at the Cleveland Clinic followed 122,007 patients who underwent exercise stress testing between 1991 and 2014. Their conclusion was stark: individuals in the lowest fitness quintile had a mortality risk four times higher than those in the highest quintile. For comparison, being a current smoker increased mortality risk by only 1.4x, and having coronary artery disease by 1.3x.
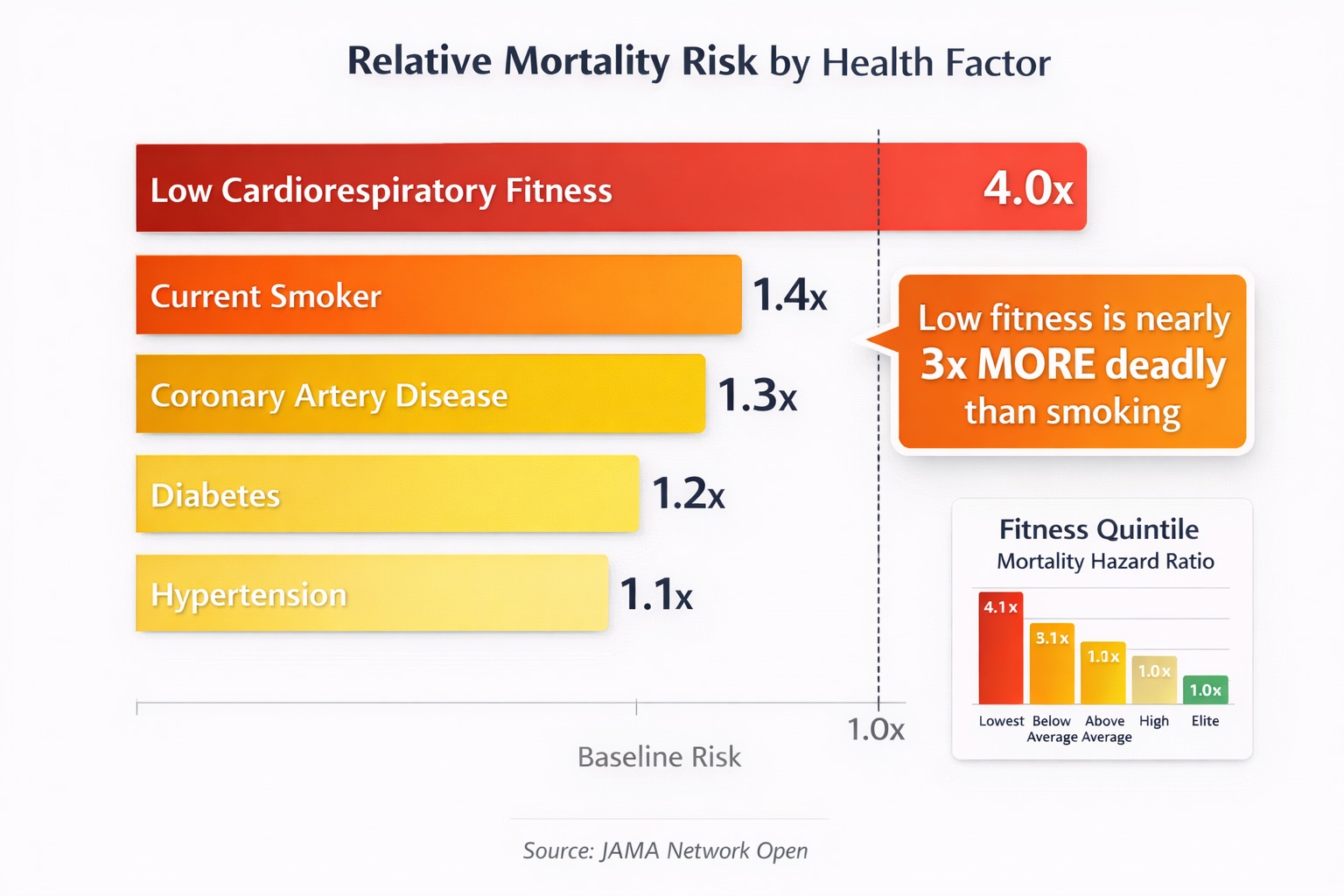
Figure 3: Cardiorespiratory fitness (VO2 max) is the single strongest predictor of longevity—low fitness increases mortality risk 4x, compared to 1.4x for smoking and 1.3x for coronary artery disease. Data source: Mandsager et al., JAMA Network Open 2018 (n=122,007).
The Copenhagen Male Study, which followed 5,107 men for 46 years, found that each 1 ml/kg/min increase in VO2 max corresponded to an additional 45 days of life. Men in the highest cardiorespiratory fitness category lived approximately five years longer than those in the lowest. Dr. Peter Attia, author of Outlive: The Science and Art of Longevity, summarizes the clinical implications: "Going from below average to above average for your age and sex in terms of VO2 max is associated with roughly a 50% reduction in all-cause mortality. No drug has ever shown an effect size that large."
Part IV: Cristiano Ronaldo—The 40-Year-Old With the Body of a 28-Year-Old
In November 2025, football legend Cristiano Ronaldo shared data that stunned the sports world: according to WHOOP's comprehensive biometric analysis, his biological age was 28.9—despite being 40 years old chronologically. "The data doesn't lie," Ronaldo posted on social media. "That means I'm going to be playing football for another 10 years!"
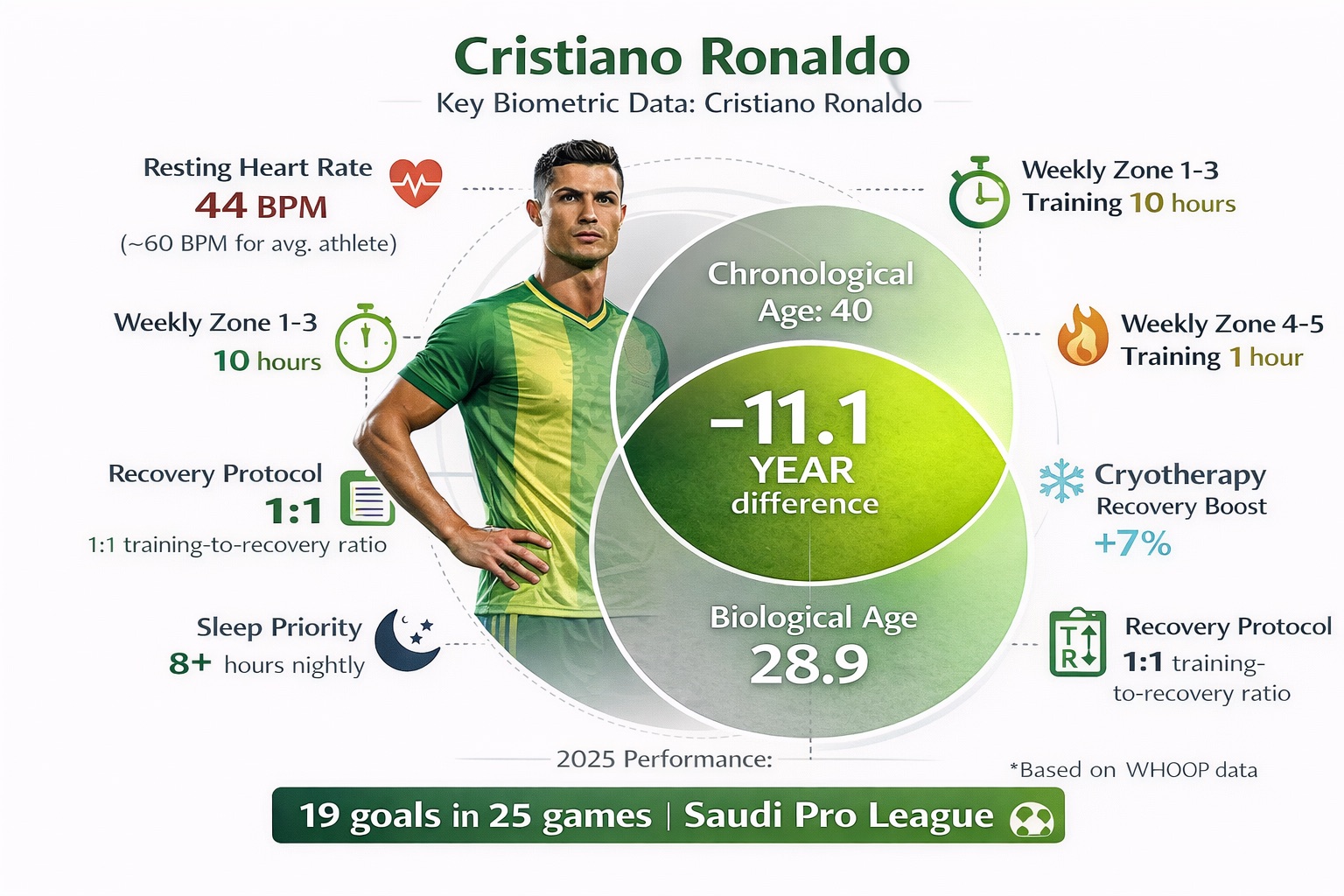
Figure 4: Cristiano Ronaldo's WHOOP data reveals a biological age of 28.9 at chronological age 40—an 11-year advantage achieved through systematic recovery protocols, a 44 BPM resting heart rate, and disciplined 80/20 polarized training. Data source: WHOOP November 2025.
This is not marketing hyperbole. WHOOP's analysis incorporated more than 140 different behaviours, with Ronaldo's resting heart rate of 44 beats per minute (BPM) alone contributing a two-year reduction in estimated biological age. His weekly training includes 10 hours in heart rate zones 1-3 (aerobic base building) plus an additional hour in zones 4-5 (high-intensity work)—a distribution that mirrors the 80/20 polarized training approach used by elite endurance athletes.
But what makes Ronaldo's protocol instructive is his emphasis on recovery. "If you're training 2 hours, you have to recover 2 hours," he explains. "You have to be smart, do things differently as you get older." His recovery arsenal includes cryotherapy (which WHOOP data shows gives him a 7% increase in recovery scores), strict sleep protocols, and real-time performance monitoring through wearable technology that tracks heart rate variability, sprint speed, power output, and workload ratios.
Ronaldo's results aren't just personal—they're statistically elite. He has scored in 19 of 25 games in the current Saudi Pro League season, outperforming younger imported stars like Karim Benzema, Sadio Mané, and Aleksandar Mitrović. His fitness tests continue to produce metrics in sprint speed, VO2 max, and body composition comparable to those of athletes a decade younger. Luis Castro, his former Al-Nassr coach, attributes this to discipline: "Cristiano has deeply ingrained routines, a strong training culture, and immense respect for the game. He's extremely disciplined with his nutrition, sleep, and body preparation. In my view, that's the key to his longevity."
Part V: LeBron James and the $1.5 Million Question
In his 22nd National Basketball Association (NBA) season, LeBron James continues to defy the actuarial tables of professional basketball. At 40 years old, he's averaging 24.9 points, 8.1 rebounds, and 8.4 assists per game while shooting 51.6% from the field—numbers that would represent career years for most players. The legendary figure of $1.5 million annually spent on body maintenance has become sports lore, though James himself remains coy about the exact figure. "That is a number that I will not disclose," he told Netflix's Starting 5 docuseries, "but more importantly, I think it's just the time."
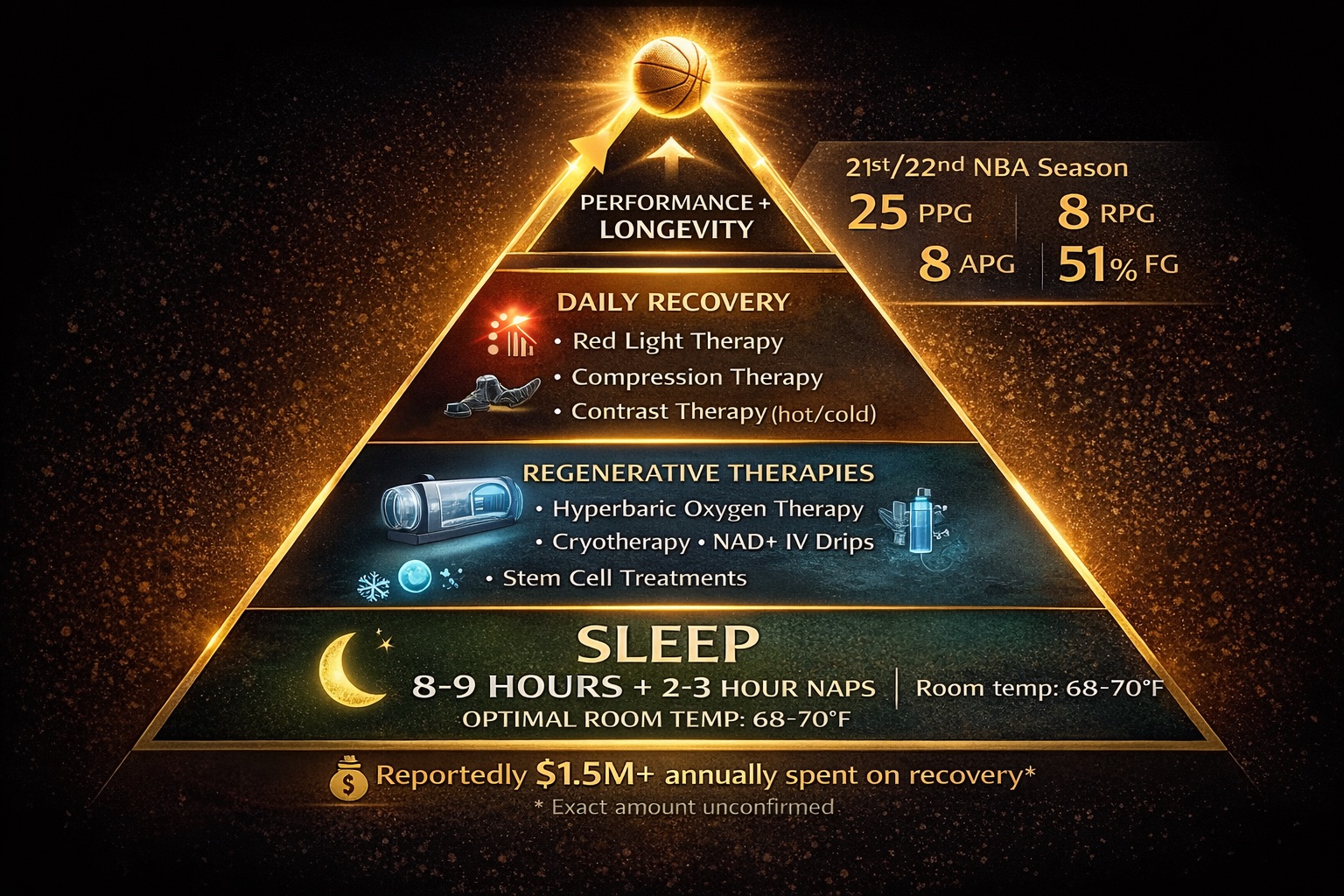
Figure 5: LeBron James's multi-layered recovery stack—from hyperbaric oxygen therapy to cryotherapy to 11+ hours of daily sleep—represents the high-investment frontier of athletic longevity that enabled his unprecedented 22nd NBA season at age 40.
James's protocol represents the high-investment end of the longevity spectrum. His routine reportedly includes hyperbaric oxygen therapy (90-minute sessions that increase stem cell production and reduce inflammation), cryotherapy chambers reaching -238°F, red light therapy for cellular repair, NAD+ IV drips to support mitochondrial function, and stem cell treatments for tissue regeneration. He prioritizes 8-9 hours of sleep nightly plus 2-3 hour daytime naps, in a sleep environment precisely controlled at 68-70 degrees with complete darkness and natural sound therapy.
The question for the rest of us: how much of this is actually necessary? Prof. Mike Chan, founder of European Wellness Biomedical Group, offers a perspective: "LeBron's approach may seem extreme, but it embodies the future of personalized regenerative care. His protocol is essentially a high-budget, high-frequency application of therapies we've been refining for over two decades in clinical settings. Longevity isn't reserved for the rich—it's about early access to emerging science."
Part VI: Do These Wearables Actually Work? The Validation Data
Elite athletes like Ronaldo and James have access to medical-grade monitoring. But consumer wearables from companies like WHOOP, Oura, Garmin, and Apple are now bringing similar capabilities to the mass market—at least in theory. The critical question is accuracy.

Figure 6: Not all wearables are created equal—Oura Ring Gen 4 achieved 99% concordance with gold-standard HRV measurements, while some devices showed only 82% agreement. Accuracy matters when health decisions depend on the data. Data sources: Dial et al., Physiological Reports 2025; Miller et al., Sensors 2022.
An independent study funded by the Australian Institute of Sport and conducted by Central Queensland University, published in Sensors, examined six popular wearable devices against gold-standard measurements. WHOOP demonstrated 99.7% accuracy in measuring heart rate and 99% accuracy in heart rate variability (HRV). Other wearables ranged from 41-96% for heart rate and 24-69% for HRV.
A 2025 study in Physiological Reports compared five consumer devices against gold-standard Polar H10 chest straps during sleep. Oura Ring (Gen 4) achieved a concordance correlation coefficient of 0.99 for HRV with a mean absolute percentage error of just 5.96%. WHOOP showed moderate accuracy (CCC = 0.94, MAPE = 8.17%), while Garmin and Polar watch devices demonstrated lower concordance.
Perhaps more importantly, does wearing these devices actually change behaviour and health outcomes? A 2025 study published in Sensors analyzed nearly one million days of longitudinal data from 12,000 WHOOP subscribers. The findings were striking: individuals who wore WHOOP daily had baseline resting heart rates nearly 4 BPM lower than those with lower wear times—a difference with potential clinical significance given evidence linking each 1 BPM increase to 3% higher all-cause mortality and 2% higher coronary heart disease risk.
Part VII: Epigenetic Clocks—Reading the Biological Script
While wearables capture physiological signals in real time, epigenetic clocks reveal something deeper: the cumulative biological record written into your DNA through methylation patterns. Think of DNA methylation as software running on your genetic hardware—chemical tags that turn genes on or off in response to aging, environment, and lifestyle.
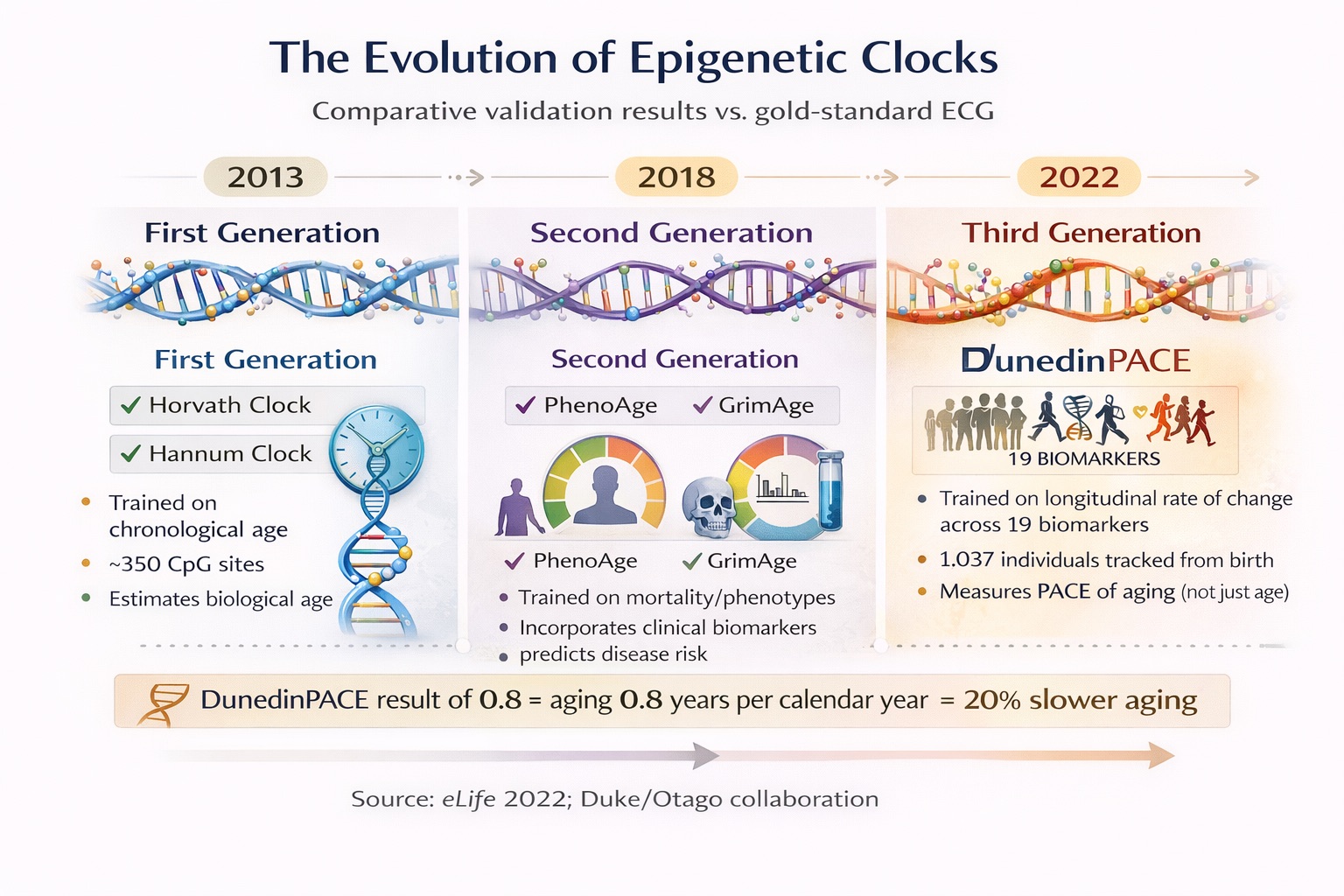
Figure 7: Epigenetic clocks have evolved from estimating biological age to measuring the real-time pace of aging. Third-generation clocks like DunedinPACE can detect whether your interventions are actually slowing cellular aging. Data source: Belsky et al., eLife 2022.
TruDiagnostic, a Kentucky-based company founded in 2020, has emerged as a leader in commercial epigenetic testing. Their TruAge test analyzes over 900,000 methylation markers to generate biological age estimates for 11 organ systems (brain, heart, liver, kidney, immune system, and more) plus an overall pace-of-aging score using the licensed DunedinPACE algorithm.
In October 2024, TruDiagnostic and Yale University published a landmark meta-analysis comparing 51 different longevity interventions across multiple biological clocks—the first study of its kind. The analysis validated that specific interventions actually slow biological aging, not just correlate with it. This matters enormously: it means we can now test whether a diet, exercise protocol, or therapeutic intervention is working at the cellular level, rather than waiting for decades to see mortality outcomes.
The DunedinPACE clock has shown robust associations with cognitive decline in the Framingham Heart Study Offspring Cohort. A faster pace of aging predicted both worse baseline cognitive performance and steeper decline over time—even after adjusting for education. In the InCHIANTI cohort study (699 adults followed up to 24 years), faster longitudinal changes in DunedinPACE were significantly associated with higher mortality, independent of baseline epigenetic age.
Part VIII: The Digital Twin Revolution—From NASA to Your Living Room
The concept of the 'digital twin' originated at National Aeronautics and Space Administration (NASA) in the 1960s, where engineers created virtual replicas of spacecraft to simulate scenarios and predict failures. Today, this technology is being applied to human physiology. According to industry surveys, 66% of healthcare executives plan to invest in digital twin technology within the next three years, with 86% viewing it as core to their digital innovation strategy.
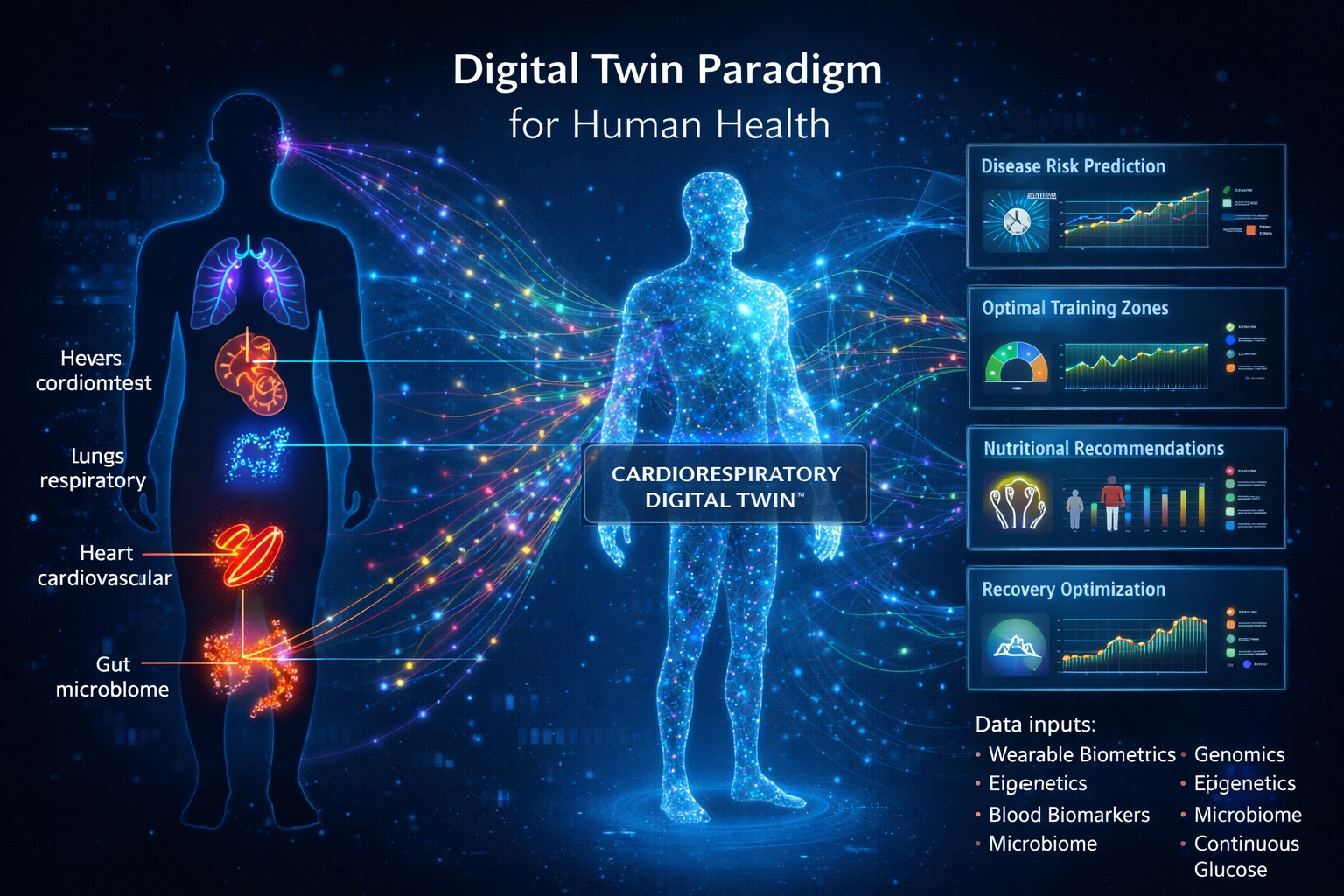
Figure 8: The Cardiorespiratory Digital Twin™ integrates real-time biometrics, genomics, epigenetics, and AI modeling to create a virtual replica of your physiology—enabling predictive health optimization that was once available only to elite athletes and astronauts.
In July 2025, researchers at Israel's Weizmann Institute of Science, led by Dr. Eran Segal, published groundbreaking research in Nature Medicine demonstrating AI-based digital twins that can predict individual disease risk and enable truly preventive treatment. The system integrates genomics, continuous glucose monitoring, microbiome data, and clinical biomarkers to create personalized health models.
For cardiorespiratory fitness specifically, the emergence of Cardiorespiratory Digital Twin™ technology represents a paradigm shift. Companies like Insilico Medicine are developing AI platforms like Precious3GPT—a multimodal transformer trained on multi-omic aging data that has identified 145 dual-purpose therapeutic targets (addressing both disease and aging processes simultaneously). Their lead compound, ISM001-0055, is now in clinical trials.
Part IX: Bridging the Divide—What Actually Works
Dr. Peter Attia's 'Medicine 3.0' framework distills the evidence into four interconnected pillars: exercise, nutrition, sleep, and emotional health. But the devil is in the details.
Exercise: The 80/20 Principle
Elite endurance athletes—from Kenyan marathoners to Norwegian cross-country skiers—consistently train with an 80/20 distribution: roughly 80% of training volume at low intensity (Zone 2, below the first lactate threshold) and 20% at high intensity. Zone 2 training builds mitochondrial density and metabolic flexibility; high-intensity intervals (like the Norwegian 4x4 protocol: 4 minutes at 90-95% max heart rate, 4 minutes recovery, repeated 4 times) push VO2 max upward.
The research supports this approach. Each 1 MET increase in cardiorespiratory fitness (equivalent to about 3.5 ml/kg/min of VO2 max) is associated with a 12-15% reduction in mortality risk. For most adults, the goal should be simple: get above average for your age and sex, then aim for 'elite' (top 2.5%). The payoff in reduced mortality is enormous.
Recovery: The Non-Negotiable
Both Ronaldo and James emphasize what most amateur athletes neglect: recovery isn't laziness—it's adaptation. Sleep, in particular, emerges as the single most impactful recovery tool. WHOOP's June 2025 research, published in the Journal of Medical Internet Research, analyzed over 300,000 monthly mental health surveys paired with 7.9 million days of biometric data. The finding: sleep consistency (regular bedtime and wake times) predicted better mental health outcomes even more strongly than total sleep duration.
Part X: The Future—Convergence and Democratization
According to the Global Burden of Disease Study 2021 forecasts, life expectancy is projected to increase by 4.9 years for males and 4.2 years for females by 2050, with the largest gains anticipated in sub-Saharan Africa and other currently low-life-expectancy regions. Dr. Christopher Murray notes: "The gaps are shrinking. The biggest increases in healthy life expectancy are anticipated in the places that currently have the least."
But technology alone will not close the healthspan-lifespan gap. The Global Burden of Disease study identifies priority conditions accounting for more than 80% of life expectancy disparities: neonatal disorders, respiratory infections, diarrheal diseases, HIV/AIDS, tuberculosis, malaria, cardiovascular disease, stroke, diabetes, road injury, and suicide. Many of these require systemic interventions—healthcare access, clean water, road safety, mental health services—rather than individual optimization.
For those with access to the emerging longevity ecosystem—wearable biosensors, epigenetic testing, AI-driven insights—the opportunity is unprecedented. The data that once required a $1.5 million annual investment (or a professional sports contract) is becoming accessible through consumer devices costing hundreds rather than millions of dollars. Companies like WHOOP, Oura, TruDiagnostic, Fountain Life, and Viome are building the infrastructure of personalized longevity planning.
Conclusion: The New Frontier
The longevity divide is real and widening. Between nations, within nations, between those with access to precision medicine and those without. But for the first time in human history, we have the tools to measure biological aging at the individual level, to track the impact of interventions in real time, and to optimize the trajectory of our own healthspan.
Cristiano Ronaldo didn't achieve a biological age 11 years younger than his chronological age by accident. LeBron James didn't play elite basketball into his 22nd season through luck. They applied systematic, data-driven approaches to the most fundamental question: how do we add life to our years, not just years to our life?
The science is clear. The technology exists. The question is no longer whether healthspan optimization is possible—it's whether we'll choose to pursue it, and whether we'll build systems that make it accessible to everyone, not just elite athletes and billionaires.
That's the mission at LongevityPlan.AI: to democratize access to the precision longevity tools that can close the healthspan-lifespan gap, one individual at a time.
About the Authors
Sarah J.M. Wang is a public health researcher and governance practitioner whose work focuses on integrating ethical artificial intelligence into health systems to advance equity, accountability, and patient-centered care. As Assistant Director of the Harvard–MIT Health Systems & AI Governance Initiative, she coordinates multidisciplinary experts across academia, theology, health administration, and industry to translate emerging AI research into operational clinical policy and governance frameworks. She holds a Master of Public Health from the Harvard T.H. Chan School of Public Health and graduated summa cum laude with a B.A. in Public Health Policy from the University of California, Irvine. Fluent in Mandarin and English, Sarah also holds training in applied data science and AI.
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data from athletes and leverages proprietary Cardiorespiratory Digital Twin™ technology, wearable data, and biomarker data to deliver personalized performance optimization and longevity recommendations to athletes, coaches, organizations, businesses, government, and the military. A 3x technology/AI company CEO with 2 successful exits, Tony has also finished 3 Full Ironman Triathlons (140.6 mi) since 2019. He holds degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University, and has worked with the US Olympic Team, the NBA, NFL, MLB, NASA, Google, Microsoft, Netflix, and Bridgewater Associates, among others. He also served as a US Navy Officer commanding an emergency response team aboard a destroyer.
Reward Muzerengwa is a PhD Candidate in Microbial Genomics and Scientific Lead of the Microbiome Mapping L19 Grant Project at the African Genome Centre (AGC), University Mohammed VI Polytechnic (UM6P) in Morocco. He has over twelve years of experience as a Senior Research Scientist and Biosafety Supervisor in biotechnology research, medical microbiology, and biosecurity with the National Biotechnology Authority of Zimbabwe. His research spans microbial genomics, vaccine development, biosecurity, and synthetic communities. He is a UN 2025 Youth for Biosecurity Fellow and an Affiliate of the Zimbabwe Young Academy of Sciences.