Women's Health
·28 min read
The Hormonal Blueprint
How Women's Endocrine Optimization, AI-Powered Longevity Planning, and Ovarian Science Are Rewriting the Rules of Youthful Healthspan
By Lina Ramos and Tony Medrano, Co-Founders of LongevityPlan.AI
Introduction: The $1.1 Billion Blind Spot
Approximately 1.1 billion people worldwide are postmenopausal women.¹ That is not a niche demographic — it is roughly the combined populations of the United States, Germany, France, the United Kingdom, and Japan. Yet until very recently, the biomedical establishment treated the hormonal transition that defines the second half of female life as little more than an inconvenience — a collection of hot flashes to be endured and a fertility question to be mourned.
That era is ending.
A convergence of longitudinal epidemiology, ovarian cell biology, wearable sensor technology, and artificial intelligence is reframing menopause not as a footnote in aging but as a central driver of it. Researchers at institutions ranging from the Buck Institute for Research on Aging to the University of Pittsburgh to Harvard's Brigham and Women's Hospital are producing data that would have seemed radical a decade ago: that the ovary functions as something close to a master clock for systemic health in females, that the timing window for hormonal intervention matters enormously, and that AI-powered personalization can transform a one-size-fits-all hormone conversation into the kind of precision protocol we already expect from elite sports medicine and oncology.
"Everyone is different. The promise of personalized preventive medicine is that we stop treating populations and start treating people," says Lina Ramos, Co-Founder of LongevityPlan.AI and 35-time Ironman Triathlon Finisher. That principle — the same one that drives the company's Cardiorespiratory Digital Twin™ technology — applies to female hormonal optimization with particular force, because the variability in how women experience the menopausal transition is staggering. The Study of Women's Health Across the Nation (SWAN), a landmark NIH-funded longitudinal study tracking over 3,300 women since 1996, has demonstrated that ethnicity, body composition, psychosocial stress, and genetic polymorphisms all modulate the timing, severity, and health consequences of reproductive aging in ways that no single prescription can address.²
This article is a science-driven guide — not a sales pitch — to understanding where the field stands today, who is doing the most important work, and how individuals and organizations can use emerging tools to plan for hormonal health across the lifespan.
Part I: The Ovary as Pacemaker — Why Reproductive Aging Drives Systemic Aging
The Organ That Ages First
Here is a number that should stop you cold: the human ovary begins to lose function a full decade or more before menopause, and ovarian aging is dramatically accelerated relative to the rest of the body. Women are born with approximately 7 million oocytes; they release only about 500 over a reproductive lifetime.³ By the time the average woman reaches her median age of natural menopause — 51.4 years — the ovarian follicle pool is effectively exhausted, and with it, the endocrine signaling architecture that coordinates bone health, cardiovascular function, metabolism, cognition, and immune regulation.
Jennifer Garrison, PhD, a neuroscientist at the Buck Institute for Research on Aging and co-founder of the Global Consortium for Reproductive Longevity and Equality (GCRLE), has become one of the most compelling voices articulating why this matters for the entire longevity field. In a 2026 interview with TIME, Garrison described ovaries as functioning like "conductors in an orchestra," coordinating health across nearly every tissue in the female body. When that coordination breaks down, she said, "it's kind of like losing the wi-fi signal to half of your devices."⁴
The science backs up the metaphor. Bérénice Benayoun, an ovarian-aging researcher at the University of Southern California's Leonard Davis School of Gerontology, has described menopause as "the worst thing that happens for women's health because it's literally the start of everything that's going to go wrong in an accelerated manner."⁵ Studies consistently show that earlier menopause is associated with higher all-cause mortality, while later menopause onset correlates with longer lifespan.⁶ Women who undergo surgical removal of both ovaries before natural menopause face chronic-disease risks that actually exceed those of naturally postmenopausal women — suggesting that even after the ovaries stop releasing eggs, they continue to provide protective endocrine signaling.⁷ However, research, technology and a new generation of health-aware women are reshaping conventional thinking.
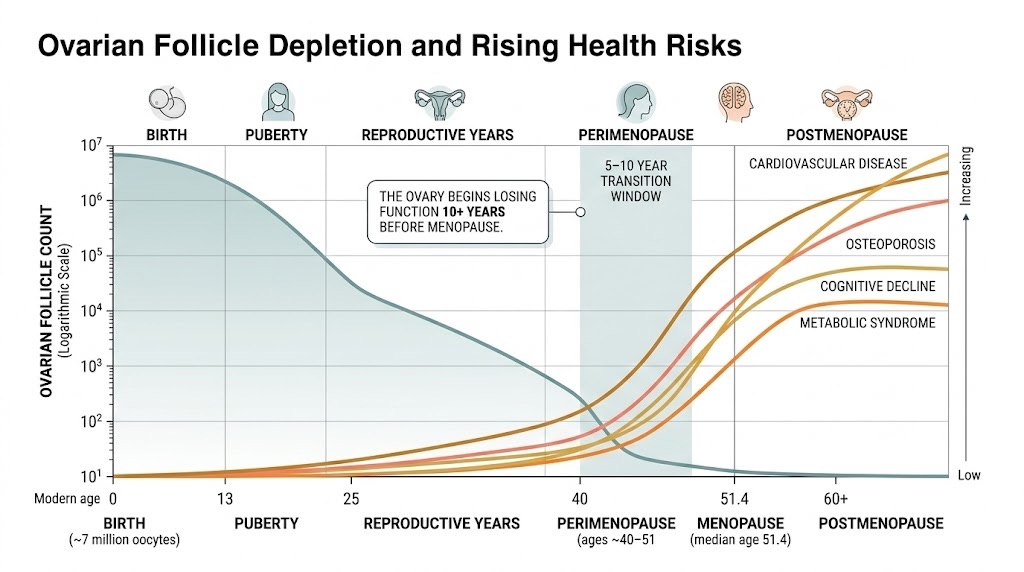
From 7 million to zero: The human ovary depletes its follicle reserve across the lifespan on a trajectory dramatically faster than any other organ system. As the SWAN study and USC's Benayoun lab have demonstrated, the perimenopausal acceleration window (highlighted) is where chronic disease risk curves begin their steepest climb — making it the most consequential period for longevity-oriented intervention.
The SWAN Study: Three Decades of Longitudinal Evidence
If you want to understand what happens to women's bodies across the menopausal transition, the Study of Women's Health Across the Nation is the single most important dataset in the world. Launched in 1994 under funding from the National Institute on Aging and the National Institute of Nursing Research, SWAN has followed a multi-ethnic cohort of midlife American women — non-Hispanic Caucasian, African-American, Chinese, Japanese, and Hispanic — through premenopause, perimenopause, and postmenopause with an unprecedented level of biological and psychosocial detail.²
Nanette Santoro, MD, Professor of Obstetrics and Gynecology at the University of Colorado School of Medicine's Anschutz Division of Reproductive Sciences and a principal SWAN investigator since 2004, has been central to interpreting these findings. Dr. Santoro was recently elected as the 2026–2027 President of the Endocrine Society — a recognition of her influence in the field.⁸ Her work through SWAN has established several enduring themes. First, the most dynamic changes in symptoms and health markers begin before the final menstrual period, during the perimenopausal transition, a phase that can last five to ten years.⁹ Second, the relationship between hormones, body composition, ethnicity, and metabolic risk varies substantially as women traverse menopause. Higher BMI, for instance, is associated with worse vasomotor symptoms during the transition but may paradoxically reduce symptoms after menopause due to peripheral estrogen conversion in adipose tissue.¹⁰ Third, reproductive milestones serve as reflections of whole-body health — abnormalities in menstrual history and menopausal timing may be markers of aberrant aging.
SWAN has also produced some of the most striking data linking menopause to cardiovascular risk. Samar El Khoudary, PhD, a SWAN investigator at the University of Pittsburgh, has shared research showing that cardiovascular fat accumulation accelerates during the menopausal transition and correlates with memory decline.¹¹ These findings are particularly relevant to longevity planning: the window around menopause may represent a critical opportunity for intervention — or a point of no return.
Hot Flashes as a Cardiovascular Biomarker
For decades, hot flashes were treated as a nuisance symptom. Rebecca Thurston, PhD, Pittsburgh Foundation Professor of Women's Health and Dementia at the University of Pittsburgh, has fundamentally changed that view. Her research, conducted through the SWAN Heart Study, the MsHeart study, and the newly funded MenoBrain study (a $7.5 million NIH-supported longitudinal investigation following 224 women entering perimenopause), has demonstrated that vasomotor symptoms — hot flashes and night sweats — are not just uncomfortable but may be markers of underlying cardiovascular and cerebrovascular risk.¹²
Using novel wearable technologies to objectively measure hot flashes (rather than relying solely on self-reports), Thurston's lab has shown that women with more frequent and severe vasomotor symptoms have poorer vascular health, increased subclinical cardiovascular disease, and elevated risk of cardiovascular events. She has extended this work to demonstrate links between hot flashes and brain aging, including white matter hyperintensities — structural brain changes associated with dementia risk.¹³
The implications for longevity planning are profound. As Thurston has stated, hot flashes may "signify poor or degrading cardiovascular health among midlife women and indicate women who warrant focused CVD prevention efforts."¹⁴ This means that a wearable device tracking vasomotor symptoms is not merely logging comfort data — it is generating a cardiovascular risk signal that, when integrated into a digital twin or AI-powered health platform, could trigger early intervention.
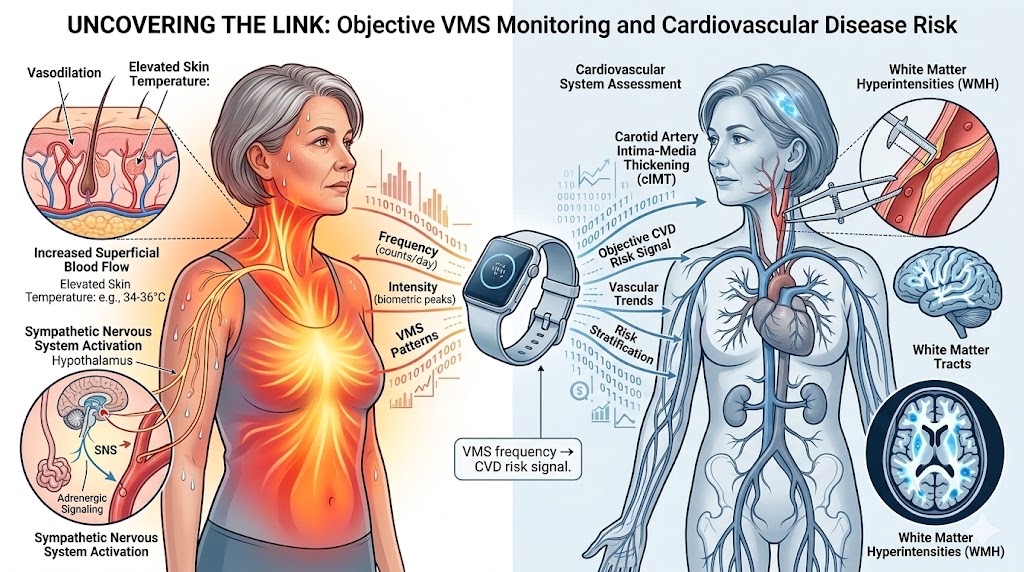
Beyond discomfort: University of Pittsburgh researcher Rebecca Thurston's work using wearable-based objective measurement of vasomotor symptoms has established hot flashes as a potential biomarker for subclinical cardiovascular disease and brain aging — transforming a "nuisance symptom" into a clinically actionable risk signal for longevity planning.
Part II: The Timing Hypothesis — When You Start Matters More Than Whether You Start
The Women's Health Initiative: From Panic to Precision
No discussion of women's hormonal health can avoid the Women's Health Initiative (WHI), the largest women's health study ever conducted in the United States, which enrolled 161,808 postmenopausal women beginning in 1993. When the estrogen-plus-progestin arm was halted early in 2002 due to findings of increased breast cancer, heart disease, and stroke risk, the shockwave was seismic: hormone therapy (HT) use plummeted by nearly 50% within six months, and an entire generation of women and their physicians developed a deep fear of hormones.¹⁵
The problem, as JoAnn E. Manson, MD, DrPH — Professor of Medicine at Harvard Medical School, Chief of Preventive Medicine at Brigham and Women's Hospital, and Principal Investigator of the WHI — has spent two decades explaining, is that the original findings were badly misinterpreted. The average age of WHI participants was 63. Most were more than a decade past menopause. Many had pre-existing cardiovascular disease. The study used a single oral formulation (conjugated equine estrogens plus medroxyprogesterone acetate) that has largely been replaced by modern preparations.¹⁶
In a landmark 2024 JAMA review paper, Manson and colleagues provided the most comprehensive synthesis to date of WHI findings across the intervention and extended follow-up phases. The conclusion was nuanced but clear: women in early menopause (under age 60 or within 10 years of menopause onset) had a lower absolute risk for adverse events from hormone therapy and generally had a more favorable benefit-to-risk profile than women in later menopause.¹⁷ As Manson has said: "It's so important for women to understand that the absolute risks of these hormones are much lower in early menopause than in later menopause."¹⁸
This concept — known as the "timing hypothesis" — has been reinforced by multiple independent studies. A 2024 Medicare analysis of 10 million senior women found that use of estrogen monotherapy beyond age 65 was associated with a 19% reduction in all-cause mortality, a 16% reduction in breast cancer risk, and an 11% reduction in acute myocardial infarction.¹⁹ A 2025 presentation at The Menopause Society's annual meeting, based on more than 120 million patient records, showed that women who started estrogen therapy during perimenopause had approximately 60% lower odds of developing breast cancer, heart attack, and stroke compared to those who began after menopause or never used hormones.²⁰
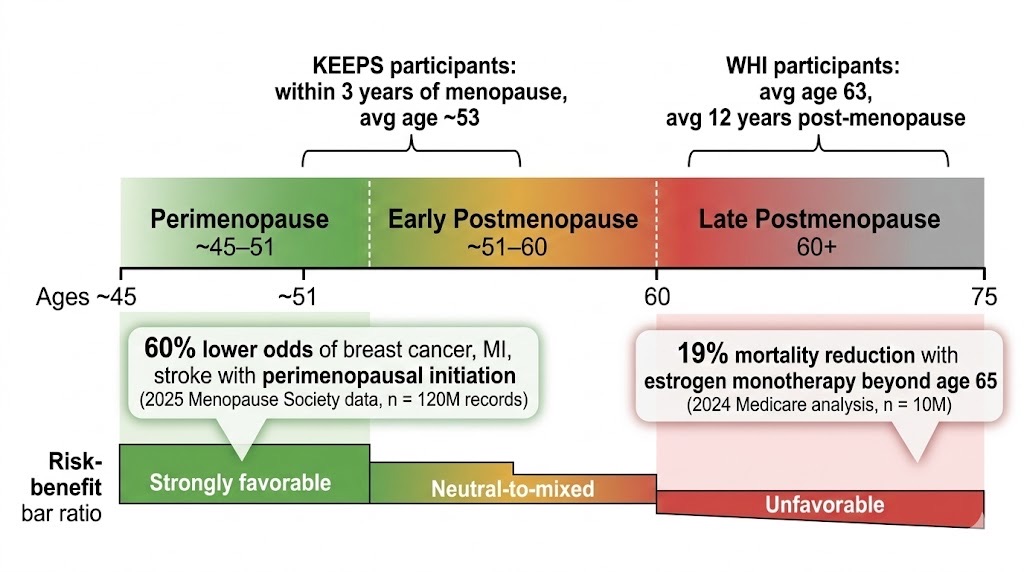
The timing hypothesis, visualized: Converging evidence from the Women's Health Initiative long-term follow-up (Manson et al., JAMA 2024), the Kronos Early Estrogen Prevention Study, and a 2025 analysis of 120 million patient records demonstrates that the benefit-to-risk profile of menopausal hormone therapy is dramatically influenced by when therapy begins relative to menopause onset — a finding with profound implications for personalized longevity planning.
The KEEPS Trial: Proof That Formulation and Timing Change Everything
The Kronos Early Estrogen Prevention Study (KEEPS), funded by the privately held Kronos Longevity Research Institute in Phoenix, Arizona, was specifically designed to address what the WHI could not: what happens when you give low-dose hormone therapy to recently menopausal women? KEEPS randomized 727 healthy women who were within three years of their final menstrual period to receive either oral conjugated equine estrogens, transdermal 17β-estradiol, or placebo — all with micronized progesterone — for four years.²¹
The results were reassuring on safety: no severe adverse events, including no venous thrombosis. Both hormone regimens reduced menopausal symptoms and maintained bone density. Importantly, the two hormone formulations differed in their effects on mood, anxiety, sleep, and sexual function — early pharmacogenomic evidence that which hormone you use, and how you deliver it, matters as much as whether you use it.²² The 14-year follow-up data, published in Menopause in January 2024, showed no long-term cardiometabolic differences between the treated and placebo groups, meaning early hormone therapy did not create lasting metabolic harm.²³
Cognitive Effects: The Lancet Weighs In
The relationship between hormone therapy and dementia has been one of the most anxiety-provoking questions in the field. In December 2025, The Lancet Healthy Longevity published a major systematic review and meta-analysis examining menopause hormone therapy and the risk of mild cognitive impairment or dementia. The conclusion: current evidence does not support the idea that hormone therapy either prevents or causes dementia.²⁴ As University College London PhD student Melissa Melville, lead author on the study, stated: "Across the globe, dementia disproportionately affects women, even after accounting for women's longer life spans, so there's a pressing need to understand what might be driving that risk."²⁵
The KEEPS Continuation Study, published in PLOS Medicine in November 2024, reached a complementary finding: cognitive performance approximately 10 years after randomization was not influenced by earlier exposure to either oral or transdermal hormone formulations.²⁶ Neither help nor harm. The implication is clear: hormone therapy should be prescribed for its demonstrated benefits — symptom management, bone preservation, quality of life — rather than marketed as cognitive insurance or feared as a dementia accelerant.
Part III: Beyond Replacement — The New Science of Ovarian Longevity
Gameto and the Cell-Engineering Frontier
If the timing hypothesis is about optimizing when to intervene, the next frontier is about what to intervene on. Dina Radenkovic Turner, MD, a physician-scientist trained at University College London and the Buck Institute, co-founded Gameto in 2020 with a mission that sounds audacious but is rooted in cell biology: to engineer solutions for accelerated ovarian aging.²⁷
Gameto's approach uses induced pluripotent stem cell technology — building on work from the laboratory of Harvard geneticist George Church — to create lab-made ovarian support cells ("ovaroids") that can mature eggs outside the body with minimal hormonal stimulation. The company's first product, Fertilo, has cut the IVF hormone injection regimen from two weeks to approximately two days. Fertilo has achieved regulatory clearance in Australia and multiple countries across Latin America and Asia; the first baby born using the technology turned one in December 2025.²⁸
But Gameto's ambitions extend well beyond fertility. The company's Ameno program, which received $10 million in ARPA-H funding in January 2025 as part of the White House Initiative on Women's Health Research, is targeting menopause itself.²⁹ Radenkovic Turner has been characteristically direct about the goal: "I do not compromise. I want to make menopause optional."³⁰
This is not mere entrepreneurial bravado. The underlying science is real: if ovarian support cells can be regenerated or replaced, the hormonal cascade that coordinates systemic health could theoretically be extended — not indefinitely, but meaningfully. The company has raised approximately $127 million to date and is in Phase 3 clinical trials for Fertilo.³¹
The $50 Million Double X Prize
In a dramatic move to accelerate the field, Jennifer Garrison co-led the creation of the "Double X Prize" — a $50 million XPrize competition announced in 2025 and set to launch in January 2026 — that challenges scientists to develop better ways to track ovarian health across a woman's entire lifespan.³² As Garrison told The Wall Street Journal, ovaries "are a proxy for what is driving aging in everyone." The prize is designed to fuel innovations that benefit not only women but the broader understanding of human aging.
AMH and the Molecular Pipeline
Anti-Müllerian hormone (AMH), produced by ovarian follicles, has emerged as a promising target for ovarian longevity interventions. Oviva Therapeutics — acquired by Granata Bio in 2025 — is developing an AMH drug aimed at preserving ovarian function. Meanwhile, Celmatix is experimenting with an AMH-mimicking molecule and plans primate trials before moving to human studies.³³ These are early-stage programs, but they represent a new therapeutic category: drugs designed not to treat disease after it occurs but to preserve the endocrine architecture that prevents disease in the first place.
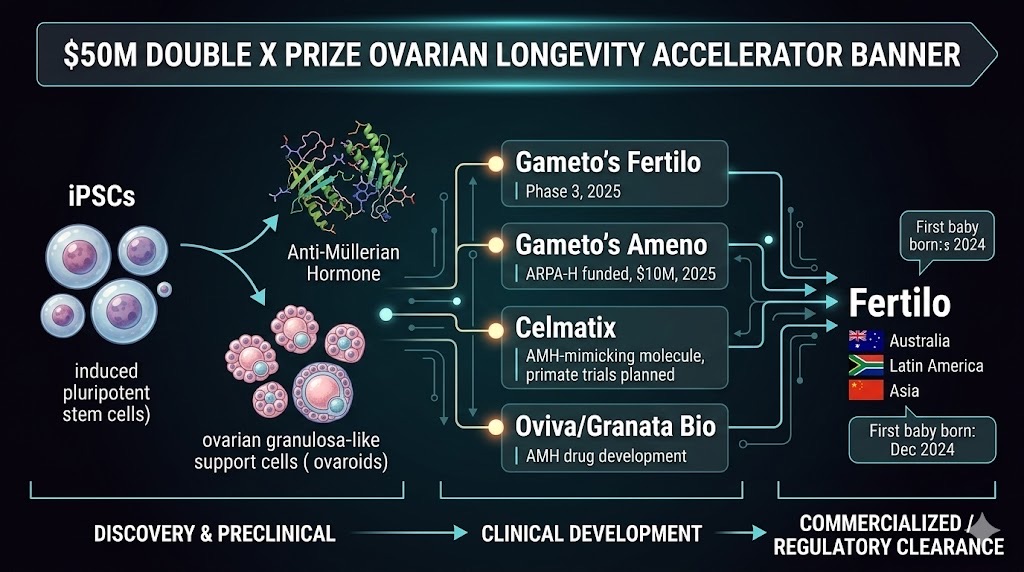
Beyond replacement: A new generation of biotechnology companies — led by Gameto (co-founded by Dina Radenkovic Turner, MD) with $127M raised and ARPA-H backing — is targeting the root cause of ovarian aging through cell engineering and molecular therapeutics, while the $50M Double X Prize aims to catalyze an entirely new field of ovarian health tracking across the female lifespan.
Part IV: The Exercise Prescription — What Changes When Hormones Do
Women Are Not Small Men
No discussion of hormonal optimization for longevity is complete without exercise physiology — and no one has done more to translate the science of female-specific training than Stacy Sims, PhD, an exercise physiologist who has directed research programs at Stanford University and the University of Waikato. Sims's famous TED talk, "Women Are Not Small Men," and her books ROAR (2016, revised 2024) and Next Level (2022), have established a new paradigm: female physiology requires fundamentally different training and nutrition strategies, and those strategies must adapt again during perimenopause and menopause.³⁴
The key insight is counterintuitive. As estrogen and progesterone decline, the adaptations that once came "for free" from the hormonal milieu — body composition maintenance, recovery efficiency, mitochondrial respiration advantages — must be deliberately trained. Sims advocates for sprint interval training (SIT) and heavy resistance training rather than the moderate-intensity, long-duration cardio that many midlife women default to. The reasoning is physiological: moderate exercise in a low-estrogen environment primarily increases cortisol and promotes visceral fat storage, while high-intensity, short-duration efforts stimulate the anabolic signaling pathways that hormones previously supported.³⁵
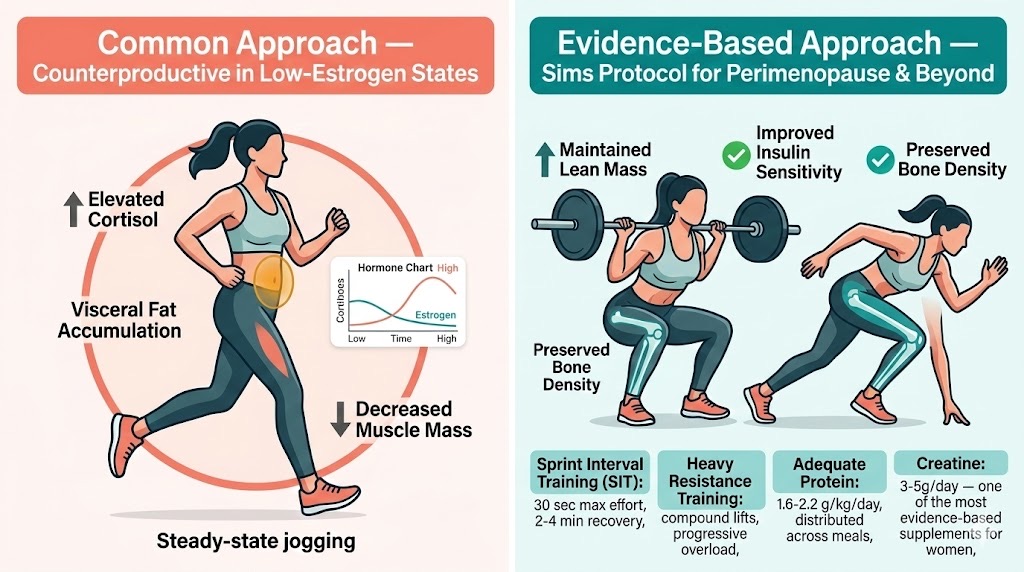
Women are not small men — especially after 40: Exercise physiologist Dr. Stacy Sims (Stanford, University of Waikato) has demonstrated that as estrogen and progesterone decline during perimenopause, the training stimulus must shift from moderate-intensity endurance to high-intensity interval and resistance protocols to maintain the anabolic adaptations that hormones previously provided. The common approach (left) can paradoxically accelerate body composition decline.
Sims also challenges the prevailing narrative that intermittent fasting is universally beneficial: in perimenopausal and menopausal women, caloric restriction can amplify the cortisol dysregulation that is already occurring. Her recommendation is to eat adequately, prioritize protein (especially around training), and supplement with creatine — which she considers one of the most evidence-based and female-relevant supplements available.³⁶
This is exactly the kind of individualized, data-driven protocol that platforms like LongevityPlan.AI are designed to support. When a coach or athlete can see real-time wearable data — heart rate variability, sleep architecture, training load — alongside hormonal biomarkers and metabolic panels, the training prescription stops being generic and starts being genuinely personalized.
Abbie Smith-Ryan and the Research on Female Athletes
At the University of North Carolina at Chapel Hill, Abbie Smith-Ryan, PhD, has been conducting some of the most rigorous research on exercise, body composition, and hormonal status in female athletes and active women. Her work demonstrates that the metabolic responses to exercise differ significantly between pre- and postmenopausal women, and that these differences have implications for everything from glycogen utilization to fat oxidation to recovery protocols. This is the kind of granular, sex-specific physiology data that needs to be incorporated into digital twin models to make them genuinely useful for half the population.
Part V: AI, Digital Twins, and the Future of Personalized Hormonal Health
The NSF-NIH Workshop on AI and Menopause
In a signal of how seriously the federal government is taking this convergence, the U.S. National Science Foundation hosted a landmark workshop in 2024–2025 titled "Using AI to Better Understand Menopause," co-convened with the NIH. The workshop brought together experts from biomedical and computational fields to explore how artificial intelligence can analyze genetic markers, hormone levels, and behavioral data to discover previously undetected variations in women's biological changes — and translate them into personalized treatment strategies.³⁷
NSF Chief Science Officer Karen Marrongelle opened the proceedings. Carolyn Mazure, chair of the White House Initiative on Women's Health Research, spoke about the important role AI is playing in improving women's health. The consensus was clear: the data exists, the computational tools exist, and the clinical need is massive — what has been missing is the integration layer.
Digital Twins and Biological Age Divergence
Research from multi-omics longitudinal studies has uncovered a striking finding: men tend to age biologically at a steady, linear pace, while women experience a sharp acceleration around the time of menopause. Bone density decline, for example, correlates more closely with time since menopause than with chronological age.³⁸ This means that a woman's "biological age" — as measured by epigenetic clocks, organ-specific biomarkers, and functional metrics — can diverge rapidly from her calendar age during the perimenopausal window.
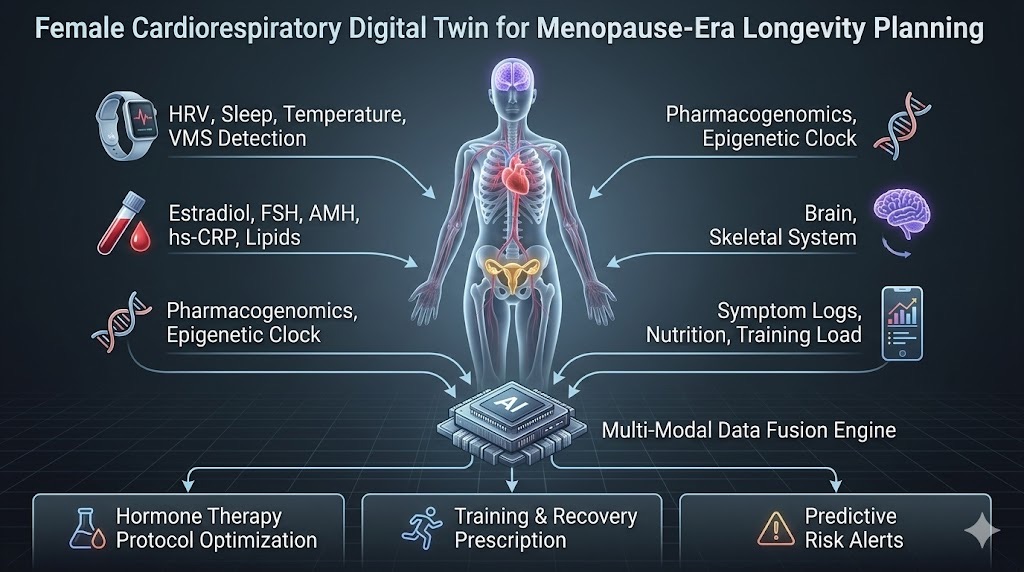
The integration layer that doesn't exist yet — but should: A properly constructed Cardiorespiratory Digital Twin™ for women navigating the menopausal transition would fuse wearable biometrics (HRV, sleep, temperature, objectively measured vasomotor symptoms), blood biomarkers (hormonal panels, inflammatory markers, metabolic panels), genomic data (pharmacogenomic variants affecting hormone metabolism), and lifestyle inputs into a unified AI model capable of recommending personalized hormone therapy formulations, training protocols, and predictive risk alerts. Platforms like LongevityPlan.AI are designed to build this integration layer.
This is precisely where digital twin technology becomes transformative. A 2025 paper in Frontiers in Digital Health described how digital twins are being developed for personalized medicine, integrating genetic, metabolic, behavioral, and environmental data into virtual models that can simulate health trajectories and test interventions in silico before applying them in vivo.³⁹ A 2025 paper in npj Digital Medicine from University College London described the integration of physics-based digital twins with AI — termed "Big AI" — as the pathway to truly individualized medicine.⁴⁰
For women navigating the menopausal transition, a properly constructed digital twin could integrate wearable data (sleep, HRV, vasomotor symptom frequency), blood biomarkers (estradiol, FSH, AMH, inflammatory markers, lipid panels), genomic data (pharmacogenomic variants affecting hormone metabolism — the kind KEEPS identified), and lifestyle inputs (exercise modality, nutrition, stress) into a unified predictive model. That model could then recommend not just whether to initiate hormone therapy, but which formulation, what delivery route, and when to adjust — turning a blunt clinical tool into precision medicine.
LongevityPlan.AI and the Integration Challenge
This is the challenge that LongevityPlan.AI was built to address. Co-Founder Lina Ramos (35-time Ironman finisher, three-time Kona World Championship qualifier including 2026, Stanford MBA) perspective on women’s hormonal performance optimization and health was born from the real-world experience trying to make sense of data fragmentation in endurance sports — and the recognition that the same problem plagues preventive medicine.
Athletes use different wearables (Oura, WHOOP, Garmin). They visit different biomarker providers (Function Health, InsideTracker, Viome). Their coaches spend 30–45 minutes per athlete per week compiling data before analysis can even begin. The same fragmentation affects women navigating the menopausal transition: hormone panels from one lab, wearable data from another device, symptom logs in a third app, and no unified intelligence layer connecting them.
LongevityPlan.AI's approach — building a Cardiorespiratory Digital Twin™ that integrates wearable data, lab results, biomarkers, medical records, and lifestyle activities into a personalized AI-powered replica — is designed to solve this integration problem. For a female endurance athlete entering perimenopause, this could mean correlating declining estradiol levels with changes in HRV recovery patterns, sleep architecture disruptions, and training response degradation — then recommending specific protocol adjustments before performance collapses or injury risk spikes.
Midday and Mayo Clinic: AI Meets Menopause Management
Lisa Health's Midday platform, developed in collaboration with Mayo Clinic, represents another node in this emerging ecosystem. Midday uses advanced algorithms and sensor technology to evaluate menopause progression and deliver personalized insights. Users can connect wearable devices to the app and receive menopause-specific health insights, and the platform includes a Mayo Clinic–powered algorithm that helps women determine whether hormone therapy may be appropriate for them.⁴¹ The premium version incorporates patent-pending algorithms for advanced symptom tracking, including the ability to detect and measure hot flashes using commercial wearable technology — precisely the kind of objective vasomotor symptom data that Rebecca Thurston's research has shown to be clinically meaningful.
Flo Health: AI at Scale
Flo Health, the leading femtech app for menstrual cycle tracking, achieved unicorn status in mid-2024 with a valuation exceeding $1 billion. With nearly 240 million downloads and close to 70 million monthly active users, Flo uses AI-powered machine learning algorithms to provide personalized insights based on cycle data.⁴² While Flo's primary focus has been reproductive-age women, its massive dataset and AI infrastructure position it to become a significant player in perimenopause and menopause tracking — if it chooses to invest in that direction.
Part VI: The Advocates — Changing the Conversation from Silence to Science
Mary Claire Haver: From Galveston to Global Influence
Mary Claire Haver, MD, a board-certified OB/GYN, Menopause Society Certified Practitioner, and adjunct associate professor at the University of Texas Medical Branch, has arguably done more than any single clinician to bring menopause science into the mainstream conversation. Her New York Times #1 bestselling book The New Menopause (2024) and her Galveston Diet program — the first nutrition protocol specifically designed by a female OB/GYN for women in menopause — have reached hundreds of thousands of women who were previously told to "eat less and exercise more" by physicians with no menopause-specific training.⁴³
Haver's work is important not because it breaks new scientific ground (she would be the first to credit the researchers whose work she synthesizes) but because it bridges the enormous gap between what the science shows and what patients actually experience in clinical encounters. A 2019 cross-sectional survey found that obstetrics and gynecology residents, family medicine residents, and internal medicine residents all had significant knowledge gaps in menopause management.⁴⁴ Haver's platform fills that void at scale.
Louise Newson: The UK's Menopause Revolution
Across the Atlantic, Louise Newson, FRCGP — a GP, hormone specialist, and member of the UK Government's Menopause Taskforce — has been described as "the medic who kickstarted the menopause revolution." She founded the Newson Health Menopause and Wellbeing Centre in Stratford-upon-Avon, created the free Balance menopause app (used by thousands of women to track symptoms and access evidence-based information), and hosts the UK's No. 1 medical podcast.⁴⁵ A Visiting Fellow at Murray Edwards College, Cambridge, and a Sunday Times bestselling author, Newson has been relentless in advocating for improved GP training and expanded access to hormone therapy.
Her influence has been both clinical and political. The UK's National Health Service has expanded menopause services and education in part because of the public pressure generated by Newson and the community she has built. Her work represents a model for how a single clinician, amplified by digital platforms and media, can shift public health policy.
Stephanie Faubion and The Menopause Society
Stephanie S. Faubion, MD, MBA, serves as medical director of The Menopause Society (formerly the North American Menopause Society), the leading professional organization in the field since 1989. Dr. Faubion, who also directs the Mayo Clinic Center for Women's Health and the Mayo Clinic Menopause and Women's Sexual Health Clinic, has been a critical voice for evidence-based, individualized care. In response to the 2025 Menopause Society findings on early estrogen therapy initiation, Faubion stated: "For most women, it's not necessary to discontinue hormone therapy simply because they've reached a predetermined age. Consideration must be given to their specific risk factors and health status."⁴⁶
The FDA Label Change Debate
In late 2025, Nature reported that the U.S. FDA was removing serious health warnings from hormone replacement therapies — a move that reflects the evolution in scientific understanding since the WHI but that some researchers worry may swing the pendulum too far in the other direction.⁴⁷ The concern is not that hormone therapy is dangerous — the data increasingly show it is safe when initiated appropriately — but that the message needs to be nuanced, individualized, and grounded in the kind of personalized risk assessment that AI platforms are uniquely suited to provide.
Part VII: The Corporate Landscape — Who Is Building What
Established Players
Fountain Life, the longevity-focused health platform co-founded by Peter Diamandis, offers comprehensive diagnostic packages that include hormonal panels alongside full-body MRI, coronary CT, and DEXA scans. Their model — catch disease before it catches you — is particularly relevant for women in the perimenopausal window, where early detection of cardiovascular risk and bone density changes can guide hormone therapy decisions.
InsideTracker, the biomarker analytics platform, has expanded its offerings to include sex-specific analysis and recommendations — a recognition that the same blood panel produces very different clinical implications depending on hormonal status. For a 45-year-old woman with declining estradiol, an elevated LDL reading may indicate an emerging menopausal cardiovascular risk trajectory rather than a simple dietary issue.
WHOOP continues to invest in female physiology research through its scientific advisory council, which includes Stacy Sims. The WHOOP platform already tracks menstrual cycle phases and adjusts recovery recommendations accordingly — an infrastructure that could be extended to perimenopause and menopause tracking with additional biomarker integration.
Oura provides similar menstrual cycle insights via its temperature-sensing ring. As ovarian function declines and temperature regulation becomes more variable (a hallmark of vasomotor instability), Oura's continuous temperature data could become a real-time proxy for menopausal status — though this application has not yet been clinically validated.
Innovative Startups
Twin Health uses AI-driven "whole body digital twins" to reverse metabolic disease. While their primary focus has been Type 2 diabetes, the platform's ability to model metabolic function makes it a natural candidate for menopause-related metabolic dysfunction — particularly the increased risk of metabolic syndrome that University of Pennsylvania researchers recently documented in women who reach menopause before age 45.⁴⁸
Tally Health, co-founded by Columbia University aging researcher David Sinclair's collaborator and Harvard genetics researcher, offers epigenetic age testing and personalized longevity recommendations. For women, the sharp acceleration in biological aging around menopause makes epigenetic clock measurements particularly informative — and actionable.
Deep Longevity, a subsidiary of Endurance Longevity, uses AI-based biomarkers to estimate biological age from blood tests, photographs, and other data. Their aging clocks could be calibrated to capture the sex-specific aging acceleration that occurs during the menopausal transition.
GlycanAge measures biological age through immunoglobulin G glycan analysis — a biomarker panel that is particularly sensitive to inflammatory changes. Given that systemic inflammation increases markedly during the menopausal transition (a finding confirmed by SWAN research published in March 2025⁴⁹), glycan-based aging metrics may be especially informative for women navigating midlife.
Part VIII: What This Means for You — A Practical Framework
Whether you are a female executive, an endurance athlete, a coach, or a parent planning a child's long-term health trajectory, the science points toward a set of actionable principles:
1. Know Your Timeline. The perimenopausal window — which can begin in the early 40s and last 5–10 years — is the most dynamic and consequential period for hormonal health intervention. If you are a woman over 40, or if you coach, manage, or care for women over 40, this transition deserves the same strategic attention you would give to a major career milestone or athletic training cycle.
2. Get Baseline Data Early. Hormonal panels (estradiol, FSH, AMH, testosterone, SHBG), inflammatory markers (hs-CRP, IL-6), metabolic panels (fasting glucose, insulin, lipid fractions), and bone density measurements should be obtained during the late reproductive years — not after symptoms become severe. As the WHI, KEEPS, and SWAN data collectively demonstrate, the window of opportunity for intervention is narrow, and late starts yield diminished returns.
3. Integrate Your Data. Wearable metrics (sleep, HRV, temperature, activity), biomarkers, symptom logs, and medical history should flow into a unified platform — not sit in separate silos. This is the core value proposition of digital twin technology and platforms like LongevityPlan.AI: turning fragmented data streams into coherent, personalized intelligence.
4. Match Your Training to Your Physiology. Following the evidence from Stacy Sims and others, perimenopausal and postmenopausal women should shift toward high-intensity interval training, heavy resistance training, and adequate protein intake — and away from chronic moderate-intensity cardio and caloric restriction. This is not intuition; it is endocrinology.
5. Have the Hormone Conversation — With Data. The timing hypothesis is no longer a hypothesis; it is supported by converging evidence from the WHI long-term follow-up, the KEEPS trial, The Menopause Society's 2025 findings, and the 2024 Medicare analysis. If you are within 10 years of menopause onset (or under 60), and you have bothersome symptoms, the risk-benefit calculus for hormone therapy — particularly transdermal estradiol with micronized progesterone — is more favorable than at any point since before 2002. But the decision should be individualized, ideally with a Menopause Society Certified Practitioner.
6. Think Like an Organization. For corporations, sports teams, and military organizations, female hormonal health is not a personal matter — it is a performance and readiness variable. The NFL spends $213 million annually on injury prevention. NASA monitors astronaut physiology to the minute. The same organizational seriousness should apply to supporting female employees, athletes, and service members through the menopausal transition — because the performance, cognitive, and health implications are as significant as any musculoskeletal injury or sleep deficit.
Conclusion: The Next Decade
The science of women's hormonal longevity is entering a period of exponential progress. Jennifer Garrison's Double X Prize will catalyze ovarian health tracking innovations. Gameto's cell-engineering platform may redefine what menopause means. The MenoBrain study at Pittsburgh will provide the first longitudinal neuroimaging data on how the menopausal transition affects the brain in real time. AI platforms are beginning to integrate the kind of multi-modal data — wearable, genomic, proteomic, behavioral — that can turn population-level insights into individual-level protocols.
But technology alone is insufficient. The cultural shift matters too. As Dr. Faubion of The Menopause Society has noted, the conversation is changing: patients are now initiating discussions about hormone therapy before their physicians even raise it. Mary Claire Haver, Louise Newson, and Stacy Sims have each, in different ways, demonstrated that when you give women evidence-based information, they make excellent decisions about their own health.
The question for the longevity field — and for every organization, team, and individual invested in healthspan — is whether we will match that demand with the infrastructure to deliver genuinely personalized care. The data platforms exist. The science is converging. The talent is in place. What remains is execution.
"We democratize elite sports science, performance optimization, and healthspan maximization by integrating wearable data, lab results, biomarkers, medical records, and lifestyle activities into a personalized Digital Twin — an AI-powered software replica that mirrors the human body to predict, optimize, and personalize health, recovery, and performance in real-time," says Lina Ramos. “We built Longevityplan.AI to bring the predictive power of AI to traditional health science so, among other things, women could remain physically strong, mentally sharp, and energetically engaged in life, even as they advance in age," she adds. For the 1.1 billion postmenopausal women worldwide — and the hundreds of millions more approaching that transition — that vision has never been more urgent or more achievable.

From bench to bedside to boardroom: The researchers, clinicians, and entrepreneurs profiled in this article — Jennifer Garrison (Buck Institute), JoAnn Manson (Harvard), Nanette Santoro (Colorado), Rebecca Thurston (Pittsburgh), Dina Radenkovic Turner (Gameto), Stacy Sims (Stanford), Mary Claire Haver (UTMB), Louise Newson (Newson Health), and Stephanie Faubion (Mayo Clinic/Menopause Society) — represent a new generation of leaders placing women's hormonal health at the center of the longevity conversation. The question for the field is whether institutions, corporations, and individuals will match their science with the infrastructure for personalized care.
About the Authors
Lina Ramos is a serial endurance athlete, strategic leader, and longevity visionary dedicated to transforming how humans optimize performance, healthspan, and life outcomes through data-driven science and artificial intelligence. As a co-founder of LongevityPlan.ai, Lina brings decades of experience in performance endurance, business leadership, and innovation to the mission of democratizing elite health insights for everyday people.
Lina's journey to co-founding LongevityPlan.AI is rooted in her lifelong commitment to high performance and human potential. She is a 35x Ironman finisher and a three-time Ironman World Championship qualifier — achievements that reflect not just physical endurance but a deep understanding of the mental fortitude, resilience, and adaptability required to perform at the highest levels over time. Her personal experience competing at elite distance races informs the core mission of LongevityPlan.AI: to bridge the data gaps between wearables, biomarkers, lifestyle, and outcomes so individuals and coaches can unlock their peak potential in health, performance, and longevity.
Lina holds an MBA from Stanford University and a BS from the Haas School of Business at UC, Berkeley, where she refined her expertise in strategy, business systems, and scalable impact. This academic foundation, paired with hands-on problem-solving as a founder, empowers her to lead cross-disciplinary teams that integrate cutting-edge AI, digital twin modeling, and holistic human performance data.
At LongevityPlan.AI, Lina drives the company's strategic vision with a focus on real-world outcomes: helping athletes, coaches, clinicians, and everyday people cut through fragmented health data to uncover personalized insights that meaningfully extend healthspan and performance longevity. Her leadership ensures that the company's technology meets rigorous scientific standards while staying deeply accessible and actionable for users at every level.
Lina's impact extends beyond the finish line and boardroom alike. She embodies a belief that longevity isn't measured by years alone, but by the quality of life lived — a principle that informs every aspect of LongevityPlan.AI's mission to make elite performance and proactive health universally attainable.
Tony Medrano is the co-founder and CEO of LongevityPlan.AI. He is a three-time Ironman finisher and three-time tech CEO with successful exits from a $1B molecular diagnostics company and a mobile app platform company. He holds degrees from Harvard University, Columbia University, and Stanford University.
Footnotes
-
Manson JE, Crandall CJ, Rossouw JE, et al. "The Women's Health Initiative Randomized Trials and Clinical Practice: A Review." JAMA. 2024;331(20):1748-1760. doi:10.1001/jama.2024.6542
-
Santoro N. "Understanding the Menopause Journey." Climacteric. 2025;28(4):384-388. Published online February 4, 2025. doi:10.1080/13697137.2024.2445303
-
Review of hormonal replacement therapy options for the treatments of menopausal symptoms. PMC. 2025. PMC12463494.
-
Garrison J. Quoted in "Ovaries Could Unlock Secrets of Longevity." TIME. January 13, 2026.
-
Benayoun B. Quoted in "Ovaries Could Unlock Secrets of Longevity." TIME. January 13, 2026.
-
Benayoun BA, Kochersberger A, Garrison JL. "Studying Ovarian Aging and Its Health Impacts: Modern Tools and Approaches." Genes & Development. 2025;39(15-16):975-990. doi:10.1101/gad.352732.125
-
Garrison J. Quoted in "Ovaries Could Unlock Secrets of Longevity." TIME. January 13, 2026. (Regarding post-oophorectomy health risks exceeding natural menopause.)
-
SWAN Study website. "Endocrine Society members elected Nanette Santoro, M.D., of the University of Colorado School of Medicine as its 2026-2027 President." swanstudy.org. Accessed 2025.
-
Santoro N. "Understanding the Menopause Journey." Climacteric. 2025.
-
Al-Safi ZA, Santoro N. "SWAN: Key Findings to Date and More to Come." Women's Health. 2013;9(2). doi:10.2217/WHE.13.15
-
SWAN Study news releases, 2024. swanstudy.org/news.
-
Thurston RC. Research profile, University of Pittsburgh Department of Psychiatry. "Menopause and cardiovascular disease; Menopause and neurocognitive health." psychiatry.pitt.edu.
-
Thurston RC, Wu M, Chang YF, et al. "Menopausal Vasomotor Symptoms and White Matter Hyperintensities in Midlife Women." Neurology. 2023;100(2):e133-e141. PMID: 36224031.
-
Thurston RC. Research description, ScienceDirect author page. "VMS may signify poor or degrading cardiovascular health among midlife women."
-
Yale School of Medicine. "After Decades of Misunderstanding, Menopause Is Finally Having Its Moment." April 14, 2025. medicine.yale.edu.
-
Manson JE. "The Women's Health Initiative Trials: Clinical Messages." Medscape. May 6, 2024.
-
Manson JE, Crandall CJ, Rossouw JE, et al. JAMA. 2024;331(20):1748-1760.
-
Manson JE. Quoted in Peter Attia podcast episode #253, December 9, 2024. peterattiamd.com/joannmanson.
-
Use of menopausal hormone therapy beyond age 65 years and its health implications. Menopause. 2024;31(5):363-371. doi:10.1097/GME.0000000000002335
-
The Menopause Society. "When Women Initiate Estrogen Therapy Matters." Press release, October 21, 2025. menopause.org.
-
Miller VM, Taylor HS, Naftolin F, et al. "Lessons from KEEPS: The Kronos Early Estrogen Prevention Study." Climacteric. 2021;24(2):139-145. doi:10.1080/13697137.2020.1804545
-
Miller VM, et al. Climacteric. 2021. (KEEPS pharmacogenomic findings.)
-
Cardiometabolic outcomes in Kronos Early Estrogen Prevention Study. Menopause. 2024;31(1):10-17. doi:10.1097/GME.0000000000002278
-
Melville M, He L, Desai R. "Menopause Hormone Therapy and Risk of Mild Cognitive Impairment or Dementia: A Systematic Review and Meta-Analysis." The Lancet Healthy Longevity. 2025;6(12):100803. doi:10.1016/j.lanhl.2025.100803
-
Melville M. Quoted in "No Evidence Links Menopause Hormone Therapy to Dementia Risk." Contemporary OB/GYN. January 2026.
-
Gleason CE, Dowling NM, et al. "Long-term Cognitive Effects of Menopausal Hormone Therapy: Findings from the KEEPS Continuation Study." PLOS Medicine. 2024;21(11):e1004435. doi:10.1371/journal.pmed.1004435
-
Radenkovic Turner D. Company profile and founder story. Insight Partners. "How Gameto Is Reshaping Women's Healthcare." February 2026. insightpartners.com.
-
Insight Partners. "Fertilo has undergone rapid clinical and commercial progress, moving from initial concept in 2023 to Phase 3 clinical trials in 2025." insightpartners.com.
-
Insight Partners. "In January 2025, Ameno was awarded $10M in funding from ARPA-H as part of the White House Initiative on Women's Health Research." insightpartners.com.
-
Radenkovic D. Quoted in "Dina Radenkovic MD: I Want To Make Menopause Optional." The Pavlovic Today. September 29, 2021.
-
Insight Partners. "To date, Gameto has raised approximately $127M." insightpartners.com.
-
"10 Women Longevity Experts Spearheading the Science of Aging Well." The Flow Space. January 16, 2026. theflowspace.com.
-
"Ovaries Could Unlock Secrets of Longevity." TIME. January 13, 2026.
-
Sims ST. Next Level: Your Guide to Kicking Ass, Feeling Great, and Crushing Goals Through Menopause and Beyond. Rodale Books, 2022. drstacysims.com.
-
Sims ST. Interview with MetPro. "Dr. Stacy Sims Unlocks the Mystery Around Weight Loss After Menopause." September 10, 2025. metpro.co.
-
Sims ST. "Strength, Science, and Support Through Menopause." Newsletter, 2025. drstacysims.com.
-
U.S. National Science Foundation. "Harnessing AI to Bridge Gaps in Women's Health Care." August 20, 2025. nsf.gov.
-
"Your AI-Powered Digital Twin Will Predict Your Future Health." ICT&Health. September 15, 2025. icthealth.org.
-
Saratkar SY, et al. "Digital Twin for Personalized Medicine Development." Frontiers in Digital Health. 2025;7. doi:10.3389/fdgth.2025.1583466
-
Coveney P, Highfield R, Stahlberg E, Vázquez M. "Digital Twins and Big AI: The Future of Truly Individualised Healthcare." npj Digital Medicine. 2025;8:494. doi:10.1038/s41746-025-01874-x
-
Mayo Clinic News Network. "Lisa Health Launches Midday, an App Leveraging AI to Personalize the Menopause Journey, in Collaboration with Mayo Clinic." February 9, 2023. newsnetwork.mayoclinic.org.
-
Binariks. "FemTech: Opportunities for Digital Health Companies." February 12, 2025. binariks.com.
-
Haver MC. The New Menopause: Navigating Your Path Through Hormonal Change with Purpose, Power, and Facts. Rodale Books, 2024. thepauselife.com.
-
Kling JM, MacLaughlin KL, Schnatz PF, et al. "Menopause Management Knowledge in Postgraduate Family Medicine, Internal Medicine, and Obstetrics and Gynecology Residents: A Cross-Sectional Survey." 2019.
-
Newson L. About page. drlouisenewson.co.uk/about. "Sunday Times bestselling author and host of the UK's No. 1 medical podcast."
-
The Menopause Society. "Ongoing Individualized Hormone Therapy Appears to Have No Age Limit." Press release, September 10, 2024. menopause.org.
-
"Is HRT in Menopause Healthy? US Label Change Triggers Debate." Nature. November 12, 2025. doi:10.1038/d41586-025-03687-0
-
Hone Health. "Menopause Society Meeting 2025: Longevity and Hormone Insights." October 27, 2025. honehealth.com.
-
SWAN Study. "The Relation Between Systemic Inflammation and the Menopause Transition." Published March 24, 2025. swanstudy.org.
Disclaimer: This article is for informational and educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before making decisions about hormone therapy or any medical treatment.