Healthcare
·16 min read
The Future of Stroke Care: Digital Twins and AI
A Glimpse into How AI and Digital Twins Are Transforming Cerebrovascular Medicine
By Dr. Karim Godamunné MD MBA SFHM FACHE, CMO of LongevityPlan.AI

Introduction: A New Era in Cerebrovascular Medicine
Stroke remains one of the leading causes of death and long-term disability worldwide, affecting nearly 15 million people annually. Yet we stand at an inflection point in how we understand, predict, and treat cerebrovascular accidents. The convergence of artificial intelligence, multi-modal data fusion, and digital twin technology is fundamentally transforming stroke care from a reactive emergency response into a proactive, personalized medicine paradigm.
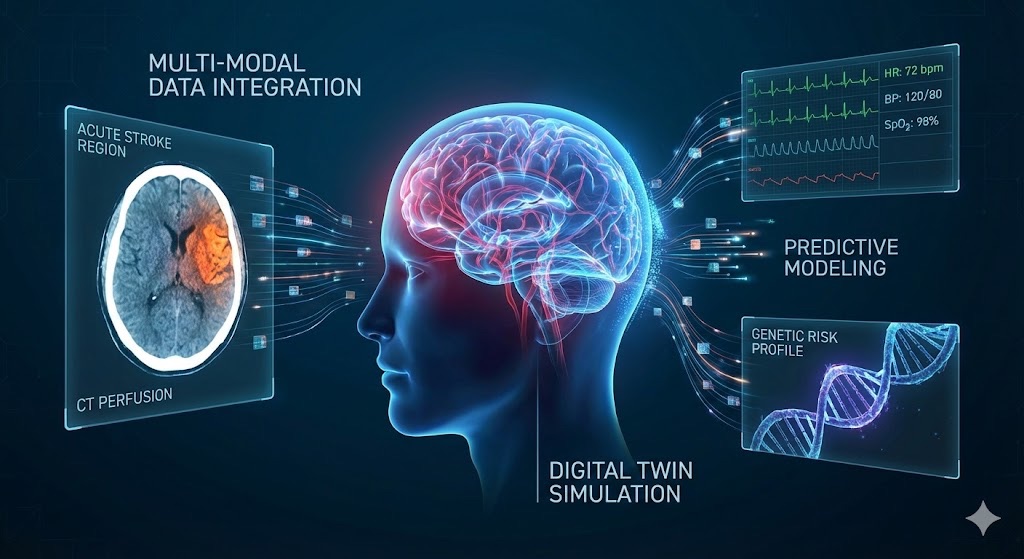
Multi-modal data fusion integrates imaging, physiological monitoring, genetic profiles, and real-time health data to create personalized digital twin models for stroke prediction and prevention. This convergence of heterogeneous data sources enables unprecedented precision in cerebrovascular risk assessment and treatment optimization.
Digital twins—virtual replicas of individual patients that continuously update with real-world data—represent perhaps the most ambitious application of AI in healthcare. When applied to stroke care, these dynamic models promise to predict individual risk, optimize treatment protocols in real-time, and personalize rehabilitation strategies with unprecedented precision. The key enabler? Multi-modal fusion: the sophisticated integration of diverse data streams including imaging, genomics, wearable sensors, electronic health records, and environmental factors into a single, coherent predictive model.
This article explores how leading researchers, innovative companies, and pioneering institutions are building the foundation for this transformation, and what it means for patients, clinicians, and the future of neurovascular medicine.
Understanding the Digital Twin: From Concept to Clinical Reality
A digital twin is not simply a static model or simulation. It is a living, breathing computational representation that mirrors a real-world entity—in this case, a patient's cerebrovascular system—and evolves continuously as new data becomes available. Think of it as a personalized avatar that captures not just your current health status, but predicts how your unique biology will respond to interventions, lifestyle changes, or disease progression.
The concept originated in aerospace and manufacturing, where companies like NASA and General Electric used virtual replicas of jet engines and spacecraft to predict failures before they occurred. The healthcare application is conceptually similar but orders of magnitude more complex. A human brain contains approximately 86 billion neurons and 100 trillion synapses, fed by a vascular network so intricate that if laid end-to-end, it would circle the Earth multiple times.
Creating a meaningful digital twin of this system requires solving what researchers call the "multi-modal fusion problem." As noted in current research frameworks, multi-modal fusion serves as the engine while the digital twin represents the outcome. In practice, a digital twin only becomes clinically useful when it continuously integrates heterogeneous data into a coherent, predictive representation of a person or organ system.
The Multi-Modal Fusion Challenge
Traditional medical decision-making relies primarily on single data modalities: a CT scan here, blood pressure readings there, perhaps genetic markers in specialized cases. But stroke risk and outcomes depend on the complex interaction of dozens of factors spanning multiple biological scales and timeframes.
Multi-modal fusion addresses this by integrating:
Imaging Data: CT scans, MRI sequences, CT angiography, perfusion imaging, and even real-time ultrasound create detailed pictures of brain structure, blood flow, and tissue viability. Companies like RapidAI, Viz.ai, and Brainomix have pioneered AI algorithms that can analyze these images in minutes rather than hours, identifying stroke signatures and calculating tissue-at-risk scores that guide treatment decisions.
Physiological Monitoring: Continuous streams from wearable devices, implantable sensors, and hospital monitoring systems track heart rhythm, blood pressure, glucose levels, and other vital signs. Organizations like Cerebrotech Medical Systems and Neural Analytics are developing novel monitoring technologies that can detect early warning signs of cerebrovascular events.
Genetic and Molecular Data: Genomic profiles influence both stroke risk and treatment response. Research institutions including Stanford University, Johns Hopkins University, and the Icahn School of Medicine at Mount Sinai are mapping the genetic variants that predispose individuals to different stroke subtypes and influence recovery trajectories.
Electronic Health Records: Longitudinal patient histories contain crucial context—previous strokes, medication adherence, comorbidities, social determinants of health. Deep 6 AI and similar platforms are using natural language processing to extract meaningful patterns from unstructured clinical notes.
Environmental and Behavioral Data: Air quality, physical activity, diet, sleep patterns, and stress levels all modulate stroke risk. The integration of smartphone data, environmental sensors, and patient-reported outcomes adds critical real-world context.
The technical challenge lies not just in collecting this data, but in creating mathematical frameworks that can meaningfully combine information that exists at different temporal resolutions (genetic data is static, heart rate varies by the second), different spatial scales (from molecular to whole-organ), and different levels of certainty (lab values are precise, patient-reported symptoms are subjective).
The Technology Ecosystem: Who's Building the Future
The stroke digital twin revolution involves a complex ecosystem of technology companies, medical device manufacturers, academic medical centers, and AI research labs. Each contributes essential capabilities.
Imaging Intelligence and Rapid Diagnosis
When a stroke occurs, time is brain—every minute of delayed treatment results in the loss of approximately 1.9 million neurons. AI-powered imaging analysis has compressed what once took 10 (Stroke Center) to 45 (routine) minutes of expert radiologist time into automated assessments completed in under a minute.
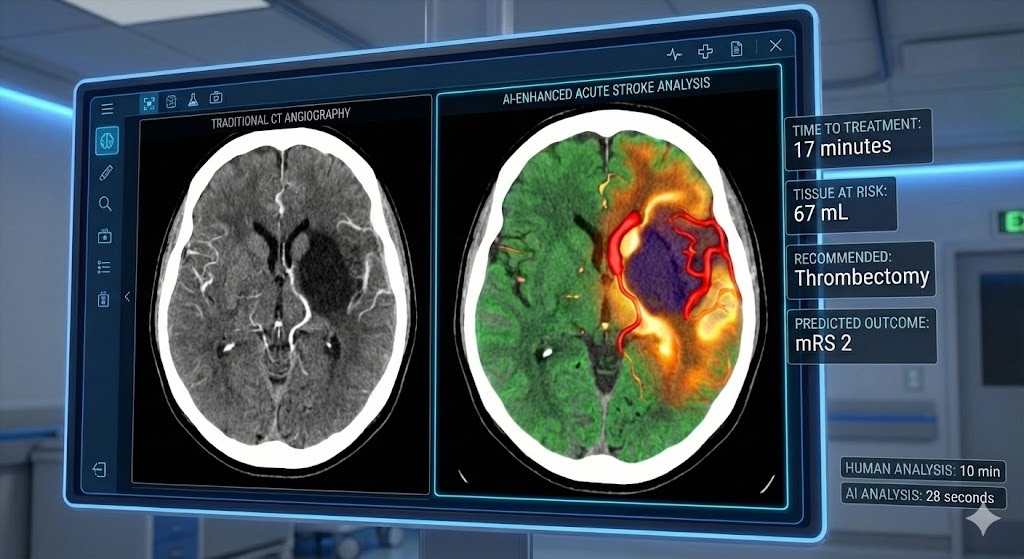
AI-powered imaging platforms analyze stroke CT scans in under 30 seconds, identifying large vessel occlusions, quantifying tissue at risk, and predicting treatment outcomes. This rapid analysis enables faster treatment decisions and improved patient outcomes in time-sensitive cerebrovascular emergencies.
RapidAI has become particularly prominent in this space, with its algorithms now deployed in thousands of hospitals worldwide. The company's platform doesn't just identify strokes; it calculates the volume of threatened tissue, predicts which patients will benefit from mechanical thrombectomy, and estimates likely outcomes based on treatment timing. Viz.ai takes a complementary approach, using AI to automatically alert stroke teams the moment a suspected large vessel occlusion is detected, coordinating the complex logistics of emergency neurovascular care.
Companies including Brainomix, iSchemaView, Aidoc, and Avicenna.ai have developed competing and complementary platforms, each with slightly different algorithmic approaches and clinical workflows. Meanwhile, traditional medical imaging giants—GE HealthCare, Siemens Healthineers, Philips Healthcare, Canon Medical Systems—have integrated AI capabilities into their scanners and analysis software, making advanced stroke detection more accessible.
What makes these systems relevant to digital twins is their ability to not just diagnose, but to quantitatively characterize individual patient physiology in ways that feed predictive models. The same imaging biomarkers that guide acute treatment decisions can be tracked over time to validate and refine a patient's digital twin.
Novel Monitoring and Detection Technologies
Beyond imaging, several companies are pioneering entirely new ways to monitor cerebrovascular health. Ceribell has developed rapid EEG systems that can detect seizures and other neurological changes in minutes. Hyperfine and Butterfly Network are making portable, affordable imaging technologies that could enable more frequent monitoring. Samsung NeuroLogica produces mobile CT scanners that bring advanced imaging to patients rather than requiring patient transport.
Neural Analytics has developed a transcranial Doppler ultrasound system that can assess cerebral blood flow non-invasively, potentially enabling continuous monitoring in high-risk patients. This type of continuous data stream is exactly what digital twins need to remain accurate and current.
Intervention and Treatment Innovation
On the therapeutic side, companies like Penumbra, Stryker Neurovascular, and Medtronic Neurovascular are advancing mechanical thrombectomy devices and flow diversion technologies. BrainQ is exploring electromagnetic stimulation for stroke recovery. What unites these innovations is an increasing emphasis on personalization—matching specific devices and treatment parameters to individual patient characteristics, exactly the type of decision digital twins are designed to optimize.
The Research Intelligence Layer
Perhaps less visible but equally crucial are companies building the AI infrastructure that makes multi-modal fusion possible. Incepto Medical and Qure.ai are developing platforms specifically designed to train and validate medical AI models across diverse datasets. Their work addresses critical challenges around algorithmic bias, generalizability, and clinical validation that must be solved before digital twins can be safely deployed at scale.
The Scientific Leadership: Minds Shaping the Field
The technology would not exist without the foundational science being conducted at leading academic medical centers worldwide. A remarkable concentration of expertise has emerged across specific institutions and individuals who are defining the evidence base for AI-enhanced stroke care.
Pioneers of Acute Stroke Treatment
The modern era of stroke treatment owes much to researchers who demonstrated that rapid intervention could reverse what was once considered permanent brain damage. James C. Grotta at the University of Texas Health Science Center at Houston helped establish the therapeutic time window for thrombolytic therapy. Jeffrey L. Saver at UCLA has been instrumental in proving the benefit of mechanical thrombectomy, fundamentally changing acute stroke treatment. Gregory W. Albers at Stanford University pioneered imaging-based patient selection, showing that the right patients can benefit from treatment even many hours after symptom onset—a finding that required sophisticated imaging analysis to implement.
These foundational insights created the clinical imperative for AI and digital twins: if treatment decisions depend on rapidly assessing complex imaging data and predicting individual patient trajectories, automation and predictive modeling become clinical necessities rather than futuristic luxuries.
The Imaging Science Innovators
David Liebeskind at UCLA has advanced understanding of collateral circulation—the brain's natural backup blood supply that can sustain tissue during a stroke. His work on quantifying collateral flow using imaging has direct applications to digital twin models, which must capture individual variations in cerebrovascular anatomy. Mayank Goyal at the University of Calgary has been central to establishing evidence for endovascular treatment and refining patient selection criteria.
Tudor G. Jovin, now at Cooper University Hospital, has pushed the boundaries of treatment time windows and explored novel therapeutic approaches. His work exemplifies the iterative process between clinical innovation and technological development that characterizes modern stroke research.
Next-Generation Clinical Researchers
A new generation of researchers is explicitly working at the intersection of data science and clinical stroke care. Adam D. de Havenon at Yale University is using machine learning to predict stroke outcomes and identify patients at risk for recurrent events. Rishi Gupta and others are exploring how real-world data from electronic health records can improve risk prediction and treatment personalization.
Lee Schwamm at Yale has been a leader in telemedicine stroke care, demonstrating how distributed expertise and rapid data sharing can improve outcomes. His work foreshadows the networked, data-intensive future that digital twins will require.
International Perspectives
The global nature of stroke research is reflected in contributions from institutions worldwide. Werner Hacke and Christoph Diener in Germany have shaped European stroke care standards. Peter Rothwell at Oxford has made fundamental contributions to understanding stroke risk stratification. Researchers at the Karolinska Institutet, Imperial College London, King's College London, and University College London are advancing complementary approaches to personalization and precision medicine in cerebrovascular disease.
Academic Powerhouses Driving Innovation
While individual researchers make crucial contributions, the infrastructure and collaborative ecosystems at major universities provide the foundation for translating digital twin concepts into clinical reality.
Harvard University, through Massachusetts General Hospital and affiliated institutions, maintains one of the world's largest concentrations of stroke research expertise. Their work spans from basic neuroscience to health services research, creating the multidisciplinary foundation essential for complex digital twin development.
Stanford University has emerged as a leader in imaging-based treatment selection and AI applications in stroke care. The institution's proximity to Silicon Valley facilitates unusual collaborations between clinicians and technology companies. Johns Hopkins University brings unparalleled expertise in neurology, neurosurgery, and biomedical engineering, with particular strength in developing novel monitoring technologies and surgical interventions.
The Mayo Clinic Alix School of Medicine exemplifies the integrated academic medical center model, where patient care, research, and education occur in tight feedback loops. This integration is crucial for digital twins, which require continuous validation against real clinical outcomes.
Other institutions are also making their mark. The Icahn School of Medicine at Mount Sinai has built a reputation for AI and data science applications in medicine. The University of California system—particularly UCLA and UC San Diego—combines clinical excellence with technological innovation and access to diverse patient populations essential for developing generalizable models.
Canadian institutions including McGill University and the University of Toronto have been particularly influential in establishing evidence for endovascular stroke treatment and developing risk prediction algorithms. Their work has shaped international treatment guidelines.
European institutions bring complementary strengths. Charité – Universitätsmedizin Berlin is one of Europe's largest university hospitals, with extensive experience in clinical trials and health technology assessment. The Karolinska Institutet in Sweden has made fundamental contributions to understanding stroke pathophysiology and recovery mechanisms.
From Data to Decisions: How Digital Twins Work in Practice
Understanding the concept of digital twins is one thing; seeing how they would function in clinical practice is another. Consider a hypothetical but realistic scenario based on current technological capabilities.

Personalized digital twin dashboards integrate genetic profiles, continuous physiological monitoring, imaging data, and environmental factors to provide individualized stroke risk predictions and simulate the impact of preventive interventions before implementation. This patient-specific modeling enables proactive, precision-based cerebrovascular care.
Prevention and Risk Prediction
Sarah is a 58-year-old woman with hypertension, prediabetes, and a family history of stroke. Her digital twin begins with a baseline created from her genetic profile, medical history, and comprehensive imaging of her cerebrovascular anatomy. Continuous data from her smartwatch tracks heart rhythm, physical activity, and sleep patterns. Periodic blood tests monitor inflammatory markers and lipid profiles.
The digital twin doesn't just store this data—it integrates information using machine learning models trained on thousands of similar patients. When Sarah's irregular heart rhythm patterns subtly change in a way that historical data suggests precedes atrial fibrillation, the system alerts her physician. When environmental sensors detect prolonged periods of poor air quality in her neighborhood correlating with elevated inflammatory markers, the model adjusts her risk assessment upward and recommends enhanced monitoring.
Crucially, the digital twin can simulate interventions before they're implemented. What happens to Sarah's five-year stroke risk if she starts anticoagulation? What if she increases exercise by 30 minutes daily? The model provides quantitative predictions personalized to her unique biology, helping Sarah and her physician make informed decisions.
Acute Stroke Response
When Sarah experiences sudden weakness and speech difficulty, the digital twin proves its value in a different way. Emergency responders transmit her vitals to the hospital, where her digital twin immediately contextualizes the data. The system knows her baseline blood pressure, cerebrovascular anatomy, medication list, and bleeding risk factors.
Upon arrival, rapid CT imaging is automatically analyzed by AI algorithms from companies like RapidAI or Viz.ai. But unlike standard protocols, Sarah's digital twin combines the imaging findings with her individual characteristics to generate personalized treatment recommendations. The system calculates that based on her collateral circulation pattern, tissue viability, and clot characteristics, she has an unusually long therapeutic time window and would benefit from thrombectomy even though six hours have elapsed since symptom onset.
During the procedure, real-time monitoring data continuously updates the digital twin, which predicts complications before they occur and suggests optimal device selection and technique parameters based on her unique vascular anatomy.
Recovery and Rehabilitation
Post-stroke, Sarah's digital twin shifts focus to rehabilitation and secondary prevention. The system integrates data from wearable sensors monitoring her movement patterns, cognitive assessment tools tracking recovery, and imaging showing structural brain changes. Machine learning models predict which rehabilitation approaches are most likely to benefit her based on patterns observed in similar patients.
When subtle changes in her gait pattern suggest developing spasticity, the digital twin alerts her rehabilitation team early enough for preventive intervention. When her medication adherence begins to slip—detected through a combination of pharmacy data and physiological monitoring—the system triggers supportive interventions.
Six months post-stroke, comprehensive reassessment updates Sarah's digital twin with new information about her recovery trajectory, adjusting long-term predictions and care recommendations. The model now estimates her risk of recurrent stroke, cognitive decline, and functional limitations years into the future, enabling proactive management.
The Technical Challenges Ahead
Despite remarkable progress, significant obstacles remain before digital twins become standard stroke care tools.
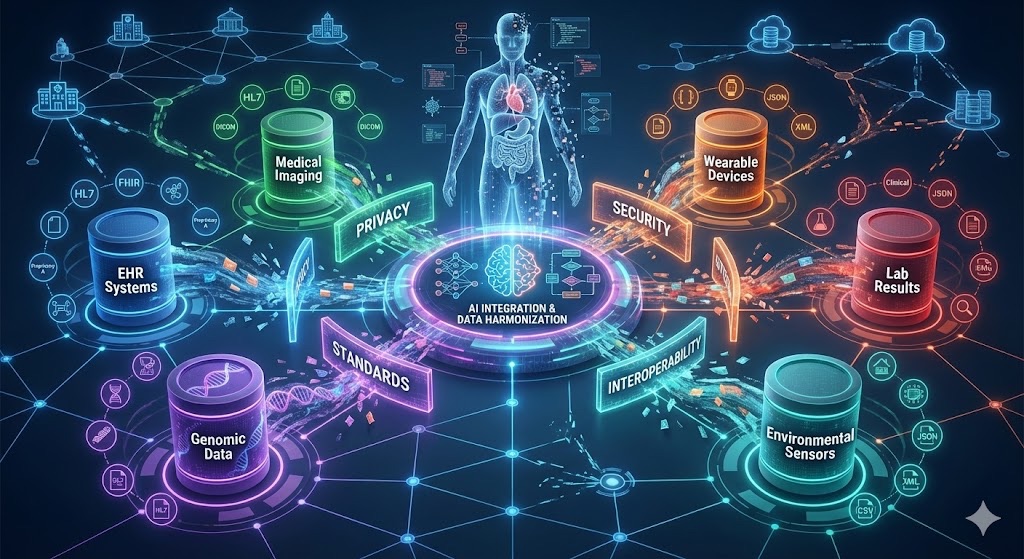
Data integration remains a critical challenge for digital twin implementation, requiring harmonization of electronic health records, medical imaging, genomic databases, wearable device data, and environmental sensors across incompatible systems and formats. Federated learning approaches and standardization efforts are working to overcome these interoperability barriers.
Data Integration and Interoperability
Healthcare data exists in countless incompatible formats across separate systems. Electronic health records from different vendors don't communicate seamlessly. Imaging data uses different protocols and resolutions. Wearable devices each have proprietary data formats. Creating truly integrated digital twins requires solving massive data engineering challenges.
Industry efforts through organizations like the American Heart Association are working to establish common data standards, but progress is incremental. Companies like Deep 6 AI are building middleware solutions that can extract and harmonize data from diverse sources, but no universal solution yet exists.
Model Validation and Generalizability
Machine learning models are only as good as the data they're trained on. Most stroke research has historically focused on populations served by large academic medical centers, potentially missing crucial variations in stroke patterns across different demographics, geographies, and socioeconomic groups.
Ensuring that digital twins work equally well for a rural patient in Mississippi and an urban patient in New York, for elderly patients and younger ones, for different ethnic backgrounds with different genetic risk profiles, requires training and validation on extraordinarily diverse datasets. Organizations like the American Heart Association are coordinating multicenter studies to address this challenge, but building truly representative datasets takes time.
Privacy and Security
Digital twins require continuous access to intimate personal data. The computational models themselves become valuable intellectual property. Balancing the clinical benefits of data sharing with privacy protection and cybersecurity concerns remains an active challenge.
Federated learning approaches—where models are trained across distributed datasets without centrally pooling sensitive information—offer one solution. Blockchain-based systems for secure data sharing represent another. Companies throughout the ecosystem are experimenting with different approaches, but no consensus has emerged.
Clinical Validation and Regulatory Pathways
Before digital twins can guide high-stakes treatment decisions, they must undergo rigorous validation demonstrating they improve outcomes compared to current standards. This requires large-scale randomized trials that are expensive and time-consuming.
Regulatory agencies including the FDA are developing frameworks for evaluating AI-based medical devices, but the continuously learning nature of digital twins—where models update as new data arrives—challenges traditional approval processes designed for static technologies. How do you validate a system that evolves over time?
Cost and Implementation
Developing and maintaining digital twins requires significant computational infrastructure, specialized expertise, and ongoing data collection. Who pays for this? How do healthcare systems justify the upfront investment when benefits may accrue over years or decades?
These economic questions will ultimately determine adoption rates. Early implementations will likely focus on high-risk patients where the value proposition is clearest, gradually expanding as costs decrease and evidence accumulates.
The Road Ahead: Next Five Years
Despite challenges, the trajectory is clear. Several developments seem likely within the next five years based on current research and development efforts.
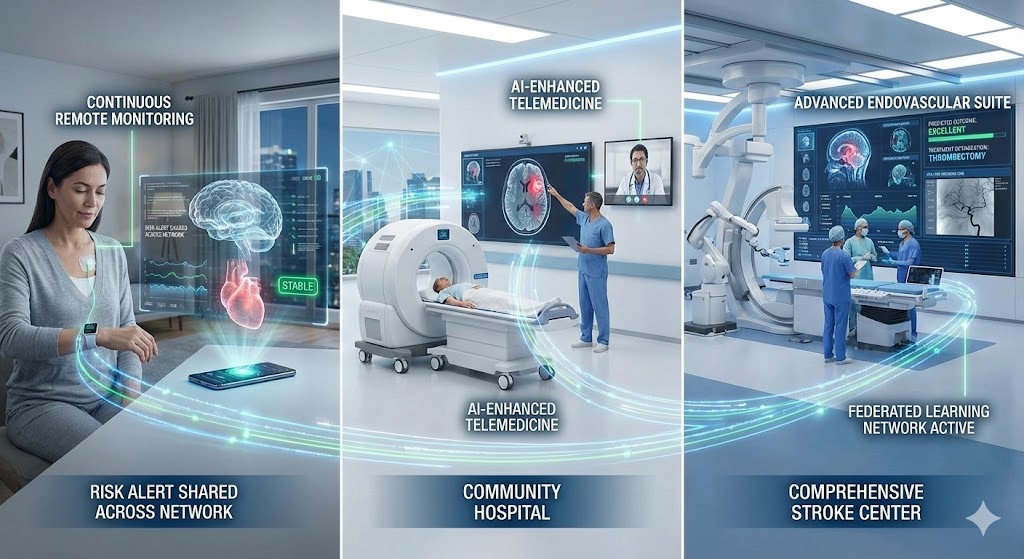
The future stroke care ecosystem will integrate continuous home monitoring, AI-powered portable diagnostics at community hospitals, telemedicine specialist access, and comprehensive stroke centers—all connected through federated digital twin networks that enable preventive care and democratize access to expertise regardless of geographic location.
Integration into Clinical Guidelines
Major stroke organizations including the American Heart Association are beginning to incorporate AI-based risk prediction and imaging analysis into treatment guidelines. This regulatory and professional acceptance creates pathways for digital twin adoption. We'll likely see initial guidelines for using predictive models in specific clinical scenarios—patient selection for extended time window treatment, personalized rehabilitation protocol selection—before broader implementation.
Expanded Data Sources
The proliferation of consumer health devices, continuous glucose monitors, and other wearable technologies will provide richer data streams for digital twins. Companies like Brainlab and established device manufacturers are developing next-generation monitoring technologies specifically designed for integration into predictive models. The challenge will shift from data scarcity to data overload, requiring sophisticated algorithms to separate signal from noise.
Federated Learning Networks
Rather than individual institutions developing isolated digital twins, we'll likely see emergence of federated networks where models trained at one institution can be improved by data from others without compromising privacy. Research collaborations between universities—Case Western Reserve, Duke, Emory, Northwestern, Ohio State, the University of Michigan, University of Pennsylvania, University of Pittsburgh, University of Washington, University of Wisconsin-Madison, and others—are laying groundwork for such networks.
Preventive Care Focus
While acute stroke treatment has driven much innovation, the greatest population health impact will come from prevention. Digital twins that identify high-risk individuals years before events occur, enabling aggressive preventive interventions, could dramatically reduce stroke incidence. This preventive focus aligns with broader healthcare trends toward value-based care and population health management.
Democratization of Expertise
One powerful promise of digital twins is making specialized expertise available everywhere. A community hospital in a rural area could leverage AI-powered decision support approaching the sophistication of treatment available at Stanford or Harvard. Companies like Butterfly Network and Hyperfine, making imaging more portable and affordable, enable data collection in settings previously lacking access to advanced diagnostics. This democratization could reduce disparities in stroke care quality.
Ethical Considerations and Equity
As with any transformative technology, digital twins raise important ethical questions that must be addressed proactively.
Algorithmic Bias and Health Equity
If digital twins are trained primarily on data from well-resourced populations, they risk perpetuating or even amplifying existing healthcare disparities. A model that works beautifully for patients similar to those in training data might perform poorly—or even generate harmful recommendations—for underrepresented populations.
Addressing this requires intentional effort to include diverse populations in research and development. Organizations like Boston University, Brown University, Columbia University, and Emory University with strong health equity research programs are documenting disparities and developing methods to ensure AI tools benefit all patients.
Autonomy and Shared Decision-Making
As predictive models become more sophisticated, there's risk they could supplant rather than support human judgment. A digital twin that recommends against aggressive treatment based on poor predicted outcomes might become a self-fulfilling prophecy if it discourages efforts that could prove the prediction wrong.
Maintaining appropriate human oversight, ensuring patients understand how recommendations are generated, and preserving space for hope and individual agency alongside data-driven predictions will require thoughtful implementation.
Data Ownership and Control
Who owns the digital twin—the patient, the healthcare institution, the technology company whose algorithms power it? What rights do patients have to access, modify, or delete their digital twin data? These questions lack clear answers and will require new frameworks balancing individual autonomy with collective benefit.
Conclusion: The Promise and the Path Forward
The convergence of multi-modal data fusion, artificial intelligence, and digital twin technology represents the most significant paradigm shift in stroke care since the advent of thrombolytic therapy and mechanical thrombectomy. We are transitioning from a model where stroke is an unpredictable catastrophe requiring emergency heroics to one where individual risk is continuously assessed, prevention is personalized, treatment is optimized in real-time, and recovery is guided by predictive models.
The ecosystem bringing this vision to reality is remarkably diverse. Technology companies like RapidAI, Viz.ai, and Brainomix are proving that AI can enhance clinical decision-making in time-critical situations. Researchers including Gregory Albers, Jeffrey Saver, David Liebeskind, and dozens of others are establishing the evidence base demonstrating when and how these tools improve outcomes. Academic medical centers from Harvard to Stanford to the University of Toronto are creating the collaborative infrastructure needed to develop and validate complex predictive models.
Yet significant work remains. Technical challenges around data integration, model validation, and computational infrastructure must be solved. Economic models that align incentives and ensure equitable access require development. Ethical frameworks protecting patient autonomy while enabling beneficial data sharing need construction. Regulatory pathways accommodating continuously learning systems must be established.
The path forward requires unprecedented collaboration among clinicians, data scientists, engineers, ethicists, regulators, and patients themselves. It demands sustained investment in both technological infrastructure and the human expertise to develop and deploy it responsibly. It necessitates commitment to ensuring that powerful new tools reduce rather than exacerbate healthcare disparities.
But the potential rewards justify the effort. Stroke remains a devastating disease that changes lives in an instant. If digital twins can predict events before they occur, optimize treatment when they do, and personalize recovery to maximize each individual's potential, the impact on human suffering would be profound.
We stand at the beginning of this journey, not its end. The companies, researchers, and institutions profiled here are building the foundation. The next decade will determine whether digital twins fulfill their promise or remain an unrealized vision. Based on the pace of innovation and the caliber of minds engaged in the challenge, there is reason for substantial optimism.
The future of stroke care is being written now—in research labs and hospital wards, in Silicon Valley startups and established medical device companies, in the algorithms being trained on millions of patient records and the clinical trials testing their real-world impact. It is a future where medicine becomes truly personalized, where prevention takes precedence over reaction, and where every patient benefits from the accumulated wisdom embedded in vast datasets transformed into actionable insight.
That future—powered by multi-modal fusion and embodied in digital twins—is closer than many realize. And for the millions who will face stroke in the coming decades, it cannot arrive soon enough.
About the Author
Dr. Karim Godamunné is the Chief Medical Officer at LongevityPlan.AI, a Board Certified Internist, Hospitalist, and a physician executive with more than two decades of experience driving clinical transformation, operational excellence, and technology-enabled care delivery. Prior to joining LongevityPlan.AI, he served as a Hospital Chief Medical Officer and was responsible for a Joint Commission Certified Comprehensive Stroke Center. He also founded a Primary Stroke Center, served as the Center's Medical Director, and was recognized for his pioneering work leveraging telemedicine for stroke systems of care.
This article presents current research and development in stroke care technology. While based on established science and ongoing research, digital twin applications in clinical stroke care remain largely investigative. Patients should consult healthcare providers for medical advice and current treatment options.