Clinical Research
·19 min read
How Digital Twins Could Redefine Clinical Trials
Exploring the Shift from Reactive Trials to Predictive Modeling
By Tony Medrano & Taylor Barkdoll, LongevityPlan.AI
1. The $2.6 Billion Coin Flip: Why Clinical Trials Are Broken
Here is a number that should keep every pharmaceutical executive, health-conscious investor, and aspiring centenarian awake at night: 90 percent of drug candidates that enter clinical trials never reach patients. The average cost of shepherding a single molecule from laboratory bench to pharmacy shelf now exceeds $2.6 billion, a figure that has tripled in inflation-adjusted dollars since the early 2000s. The timeline stretches 10 to 15 years. And the human toll—hundreds of thousands of volunteers enrolled in trials that ultimately fail—is incalculable.
The arithmetic gets worse the deeper you look. A typical Phase III oncology trial requires 500 to 3,000 patients. Recruitment alone can take two to four years. The cost per enrolled patient averages $42,000, but in complex therapeutic areas like respiratory disease, total per-study costs can exceed $115 million. And after all of that investment, approximately 50 percent of Phase III trials still fail.
Analyses of clinical trial data from 2010 to 2017 identified four primary reasons for this carnage: lack of clinical efficacy (40–50 percent of failures), unmanageable toxicity (30 percent), poor drug-like properties (10–15 percent), and inadequate strategic planning (10 percent). Notice that not one of these failure modes is insurmountable with better predictive modeling.
The Alzheimer's disease space illustrates the stakes with particular clarity. Between 2002 and 2012, the failure rate for Alzheimer's drugs was 99.6 percent. Every failed trial represents not only billions in sunk costs but years of lost hope for patients and families. If digital twins can even modestly improve the probability of success—say, from 10 percent to 15 percent—the downstream economic and human impact is staggering.
For decades, clinical trials have operated on fundamentally the same model: recruit patients, randomize them into treatment and control arms, administer therapies, wait, measure, and hope. It is a process that the late statistician George Box might have described with his famous aphorism: "All models are wrong, but some are useful." The trouble is that the current model is not merely wrong—it is ruinously expensive and heartbreakingly slow.
Enter the digital twin.
Originally engineered by NASA to monitor spacecraft in orbit—creating virtual replicas of physical systems that could be stress-tested without risking hardware—digital twin technology is now migrating from aerospace hangars into hospital wards, pharmaceutical boardrooms, and, increasingly, into your personal health planning toolkit. A digital twin in medicine is a computational model of all or part of a patient, continuously calibrated with real-world data, that can simulate responses to interventions before those interventions are ever administered. Think of it as a flight simulator for your biology.
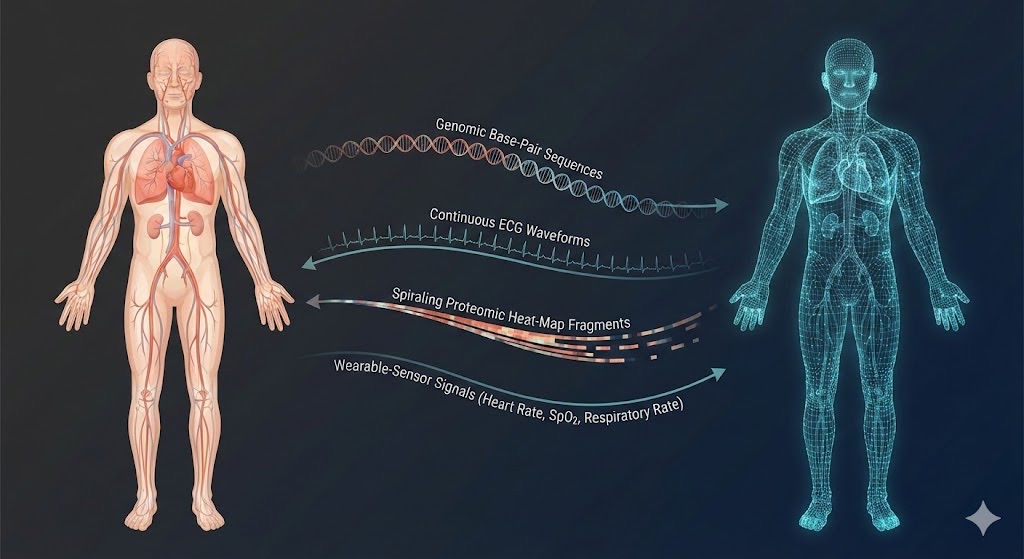
The digital twin paradigm in medicine: a continuously calibrated computational model receives multi-modal patient data and returns predictive simulations of disease progression and therapeutic response.
As Hossein Akbarialiabad and colleagues from Harvard Medical School, Oregon Health & Science University, and Yale School of Medicine argued in their 2025 paper in npj Systems Biology and Applications: "Digital twins can transform randomized clinical trials by improving ethical standards, including safety, informed consent, equity, and data privacy. They also enhance trial efficiency by enabling early detection of adverse events and streamlined design."
This article examines how digital twins are poised to redefine clinical trials—and, by extension, the entire trajectory of personalized and preventive medicine. We will explore the science, spotlight the companies and scientists leading this revolution, present verified data and peer-reviewed research, and consider what this means for anyone planning a longer, healthier, more data-driven life.
2. Digital Twins 101: From Rocket Science to Your Bloodstream
The term "digital twin" was formalized by Michael Grieves at the University of Michigan in 2002, though NASA had been using the concept since the Apollo program. In its industrial incarnation, a digital twin has two defining features: it is built on a mechanistic model of the physical system, and it is dynamically calibrated to that system through a continuous, bidirectional flow of data.
Medicine adopted the paradigm more recently but with explosive momentum. A PubMed search for "digital twin" now returns over 1,400 citations, with an exponential increase since 2020. Reinhard Laubenbacher of the University of Florida and colleagues published a landmark 2024 Perspective in Nature Computational Science outlining how medical digital twins are "most advanced in oncology and cardiology" and offer "substantial improvements in patient-specific treatments and diagnostics."
The comprehensive report Foundational Research Gaps and Future Directions for Digital Twins by the U.S. National Academies of Sciences defines a medical digital twin as a "computational model of the system to be twinned—in our case, all or part of a human patient—that is connected to [the] system in a bidirectional fashion over time, periodically recalibrated with patient data, and providing patient predictions over time." This is not just a static electronic health record. It is a living, learning model—one that evolves as you do.
For the longevity-minded, this distinction matters enormously. A static snapshot of your blood panel is a photograph. A digital twin is a motion picture, complete with the ability to fast-forward and ask: What happens to my cardiovascular system if I add Zone 2 training three days per week? What if I start metformin at age 52 versus 58?
Three Layers of Medical Digital Twins
The 2025 Lancet Digital Health review by Christoph Sadée, Olivier Gevaert, and colleagues at Stanford University—alongside co-authors from Harvard, the Institute for Systems Biology, and George M. Church's laboratory—proposes a useful framework. Medical digital twins can operate at three scales:
Molecular-level twins model cellular processes: gene expression, protein folding, metabolic flux. These are the engines behind AI-driven drug discovery at companies like Insilico Medicine and Roche.
Organ-level twins replicate the physics of specific organs—the beating heart, the ventilating lung, the filtering kidney. Dassault Systèmes' Living Heart Project, for instance, creates patient-specific cardiac simulations used by the FDA to evaluate medical devices.
Whole-patient twins integrate multi-modal data—genomics, wearables, imaging, electronic health records—into a holistic avatar. This is the frontier where clinical trials and personal longevity planning converge, and where the concept of a Cardiorespiratory Digital Twin™ begins to show its transformative potential.
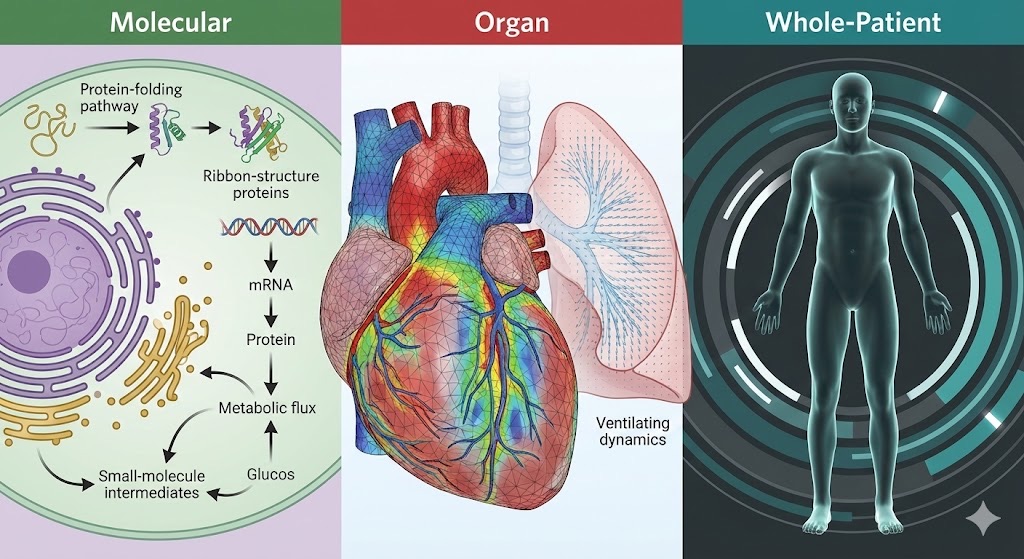
Medical digital twins operate at three complementary scales—molecular, organ, and whole-patient—each offering distinct predictive power for drug discovery, device evaluation, and personalized treatment planning (framework adapted from Sadée et al., Lancet Digital Health, 2025).
3. Unlearn.AI and the Art of the Virtual Placebo
Perhaps no company has done more to operationalize digital twins in clinical trials than San Francisco-based Unlearn.AI. Founded by Charles K. Fisher, a physicist turned machine-learning scientist, Unlearn has built a platform called TwinRCTs that creates individual-level digital twins of clinical trial participants—specifically, AI-generated predictions of how each participant would have progressed if they had received a placebo.
The statistical methodology underpinning this approach is called PROCOVA™ (Prognostic Covariate Adjustment), which Unlearn describes as a special case of the widely used ANCOVA method. The core insight is elegant: by using a pre-trained machine-learning model—built on large, longitudinal historical clinical datasets—to predict each participant's expected placebo trajectory, you generate a prognostic covariate that dramatically reduces variance in treatment-effect estimates.
The regulatory milestones are significant. In September 2022, the European Medicines Agency (EMA) formally qualified PROCOVA for use as the primary analysis methodology in Phase 2 and Phase 3 clinical trials with continuous outcomes. The U.S. Food and Drug Administration (FDA) subsequently confirmed that PROCOVA aligns with its current guidance on covariate adjustment. These are not pilot endorsements. They are regulatory green lights for real trials with real patients.
"This variance reduction [with digital twins] could have had a significant impact on the number of subjects we needed…and still preserved the same power…we would have had faster enrollment, encouraged greater patient participation. And ultimately, that would have been cost saving and time saving."
— Ole Graff, Executive Medical Director of Neuroscience, AbbVie (AD/PD 2025 Conference)
Steve Herne, Unlearn's CEO, who brings over 25 years of clinical research experience from roles at WCG, Bioclinica, and Covance, emphasizes the practical integration: "These models are powered by a proprietary neural network architecture purpose-built for clinical prediction. Integration is straightforward—sponsors can use our technology without changing endpoints, treatment arms, or randomization schemes."
A concrete demonstration of the technology's power emerged in late 2025, when AbbVie and Unlearn published results in Alzheimer's & Dementia: Translational Research & Clinical Interventions showing that digital twins, applied retroactively to the 453-patient AWARE trial (NCT02880956), reduced treatment-effect variance and offered the potential for meaningful sample-size reductions—without inflating Type I error rates.
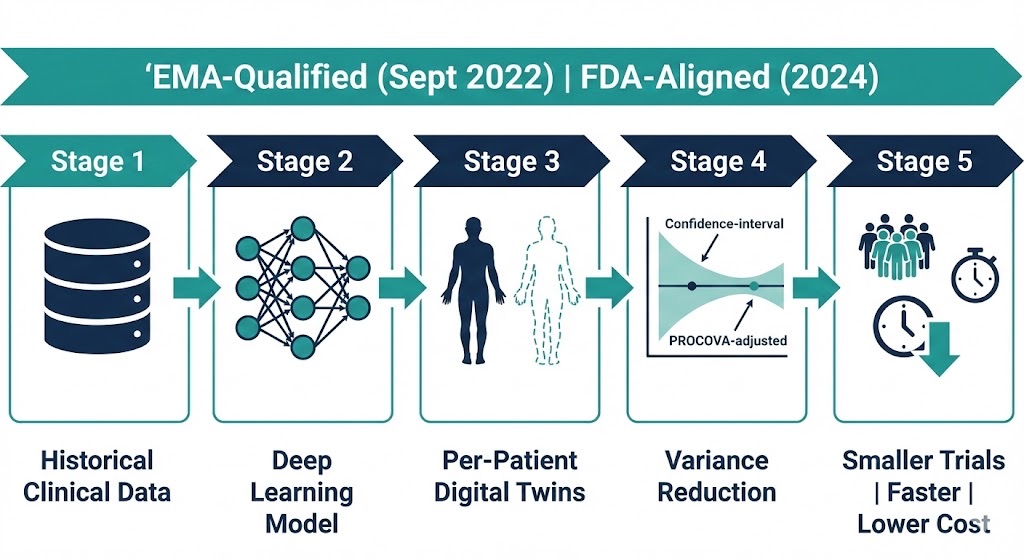
Unlearn.AI's TwinRCTs pipeline: historical clinical data trains a deep learning model that generates individual-level digital twins, producing prognostic covariates that reduce treatment-effect variance in EMA-qualified and FDA-aligned trial analyses.
4. The In Silico Trial: Running the Experiment Before You Run the Experiment
While Unlearn.AI focuses on augmenting real-world randomized controlled trials, another class of companies is pursuing something even more ambitious: fully simulated clinical trials run entirely in silico.
Nova In Silico: Predicting Trial Outcomes Before Enrollment
Lyon-based Nova In Silico (formerly Novadiscovery), co-founded by Jean-Pierre Boissel—an Emeritus Professor of Clinical Pharmacology at Claude Bernard University Lyon 1, former Scientific Director at INSERM, and one of the recognized founding fathers of systems medicine—has built a platform called Jinkō that constructs mechanistic, quantitative systems pharmacology (QSP) models to simulate clinical trials before they happen.
The proof of concept was dramatic. In a three-year collaboration with Janssen-Cilag France and thoracic oncologist Professor Michaël Duruisseaux, Nova In Silico used Jinkō to predict the results of the Phase III MARIPOSA trial in EGFR-mutant non-small cell lung cancer—a week before the actual results were unveiled at the 2023 ESMO conference. Their predictions, built on a QSP model of 5,900 digital patients, produced hazard ratios and median time-to-progression estimates whose confidence intervals overlapped with the actual trial results.
François-Henri Boissel, former CEO and co-founder, noted: "In one recent use case, we helped a biotech go directly from Phase I to Phase III as well as reducing the size of the Phase III trial by focusing on optimal responder profiles. This saved one year of time to market and a few million dollars."
What makes Nova In Silico's approach distinctive is its hybrid design: unlike purely data-driven AI models that require enormous training datasets, Jinkō blends mechanistic disease models rooted in published pathobiology with real-world data from clinical trials and preclinical work, meaning it can operate effectively even with limited sample sizes—a critical advantage in rare diseases and pediatric populations.
Duke University's Center for Virtual Imaging Trials
At Duke University, Ehsan Samei, the Reed and Martha Rice Distinguished Professor of Radiology and Director of the Center for Virtual Imaging Trials (CVIT), is building something complementary: virtual patients and virtual scanners that enable entirely simulated imaging trials.
In a landmark 2025 paper in PNAS Nexus, Samei convened a roundtable of leading scientists, regulators (including FDA officials), and industry representatives to define the future of in silico trials and digital twins in medicine. His conclusion was unequivocal: these technologies "offer a new way to efficiently qualify, quantify, and personalize healthcare innovations in advance or in conjunction with clinical application."
"In medicine, there's a significant limitation to our science. We often do not know the exact ground truth of patients. In virtual imaging trials, we know those details, because they are precise and realistic models in the computational space."
— Ehsan Samei, PhD, Duke University Center for Virtual Imaging Trials
CVIT's technology creates bio-physically accurate digital humans—complete with realistic anatomy, disease progression models, and imaging system simulations—that can be used to test how new imaging technologies or AI diagnostic tools would perform across thousands of virtual patients. The implications for drug development are significant: imaging endpoints (like tumor shrinkage measured on CT) are critical in oncology trials, and virtual imaging trials allow researchers to optimize imaging protocols and AI evaluation tools before committing to real-patient studies.
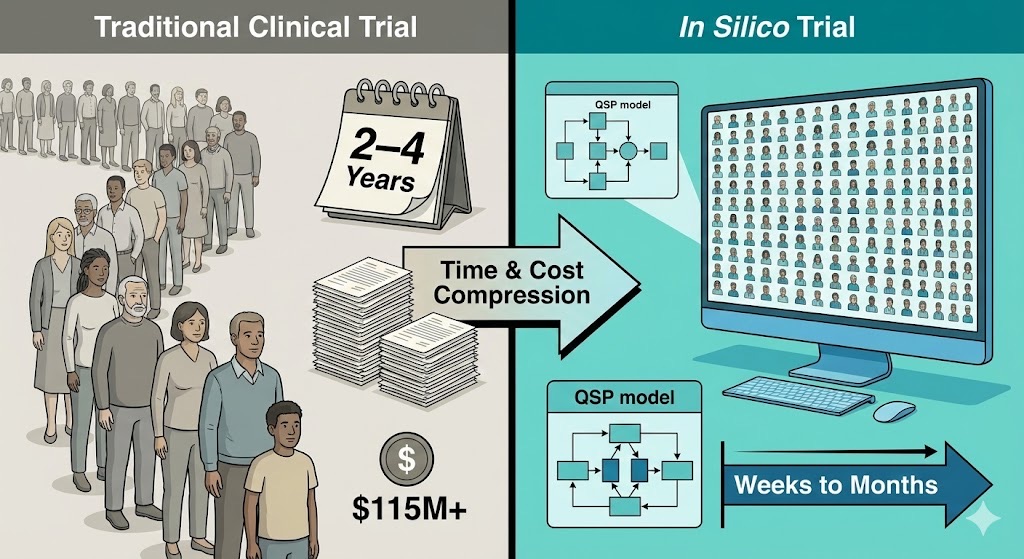
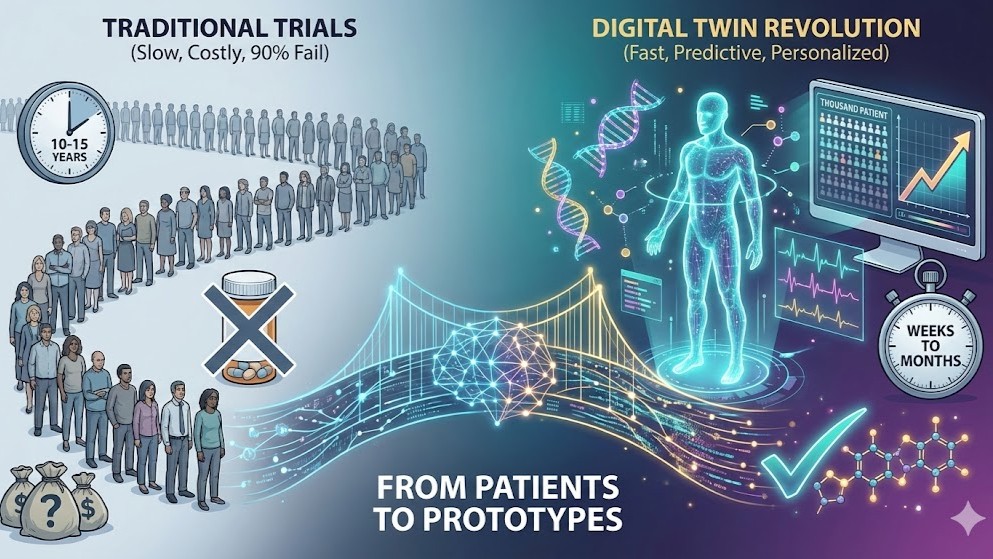
Traditional randomized controlled trials require years of enrollment and can exceed $115 million per study; in silico approaches using quantitative systems pharmacology and virtual patient populations can compress timelines from years to weeks while dramatically reducing costs.
5. Roche, AstraZeneca, and the Big Pharma Digital Twin Race
Large pharmaceutical companies are not spectators in this revolution—they are among its most active participants.
Roche has been at the forefront, with researchers at its Innovation Centers in Munich and Basel publishing foundational work on generative AI-powered digital twins. The 2024 paper by Maria Bordukova, Nikita Makarov, Fabian Schmich, and Michael P. Menden in Expert Opinion on Drug Discovery laid out the theoretical framework for how generative AI—including variational autoencoders, generative adversarial networks, and large language models—can create virtual representations of biological systems ranging from individual cells to entire patients. Their follow-up work, published in npj Digital Medicine in 2025, introduced the Digital Twin-Generative Pretrained Transformer (DT-GPT), a large language model adapted for clinical trajectory forecasting. Benchmarked on non-small cell lung cancer, ICU, and Alzheimer's disease datasets, DT-GPT outperformed state-of-the-art machine learning models, reducing scaled mean absolute error by 1.3–3.4 percent across different clinical settings.
AstraZeneca has invested in both internal digital twin capabilities and partnerships with AI companies. Michael P. Menden, a former AstraZeneca employee and collaborator on the Roche digital twin research, bridges the two organizations, underscoring the extent to which talent and ideas flow across pharmaceutical boundaries in this space.
GSK and Sanofi have also embedded digital twin methodologies into their R&D pipelines, partnering with specialized platforms like Certara and Simulations Plus for pharmacokinetic and pharmacodynamic modeling that feeds into broader patient-level simulations. Bayer and Teva have explored digital twin applications in cardiovascular and neurological disease areas, respectively.
At the 2025 Outsourcing in Clinical Trials DACH conference in Zurich, Dimitris Christodoulou, global business lead for digital health at Roche, observed that while the ultimate aim of fully simulating a patient's entire physiology remains "on the horizon," the immediate value lies in "operational and behavioral twins" that can optimize trial design, patient recruitment, and real-time monitoring.
6. Insilico Medicine: When AI Builds the Twin from the Molecule Up
The digital twin companies profiled so far operate primarily at the patient level—modeling how individuals progress through disease and respond to treatment. But recall the three-scale framework from Section 2: digital twins can also operate at the molecular level, simulating cellular processes to discover new drug targets and design molecules against them. No company has pushed this molecular-scale twinning further into clinical reality than Insilico Medicine, whose end-to-end generative AI platform treats the entire drug-target-patient system as a hierarchy of interconnected computational models.
Founded by Alex Zhavoronkov, PhD, Insilico is a clinical-stage biotech that uses generative AI not merely to assist drug discovery but to drive it end-to-end—from target identification to molecular design to clinical testing. Their flagship molecule, rentosertib (formerly ISM001-055), is a first-in-class inhibitor of TNIK (Traf2- and NCK-interacting kinase), a novel target in idiopathic pulmonary fibrosis (IPF) that was itself discovered using generative AI.
The numbers are remarkable. The entire preclinical program—from target discovery to developmental candidate nomination—took under 18 months and cost approximately $2.6 million. Contrast that with the industry average of 3 to 6 years and an out-of-pocket cost estimated at $430 million. From project initiation to Phase I dosing, the total timeline was under 30 months.
In June 2025, Nature Medicine published the Phase IIa results of the GENESIS-IPF trial (NCT05938920)—a 71-patient, double-blind, placebo-controlled study across 21 sites in China. Patients receiving 60 mg of rentosertib daily experienced a mean improvement in forced vital capacity (FVC) of +98.4 mL, compared to a decline of -20.3 mL in the placebo group—a dose-dependent response suggesting not merely slowed disease progression but potential reversal.
"These results not only suggest that Rentosertib has a manageable safety and tolerability profile, but also warrants further investigation in larger-scale clinical trials of longer duration, demonstrating the transformative potential of AI in drug discovery and development."
— Dr. Zuojun Xu, Professor, Peking Union Medical College, Principal Investigator of the Phase IIa trial
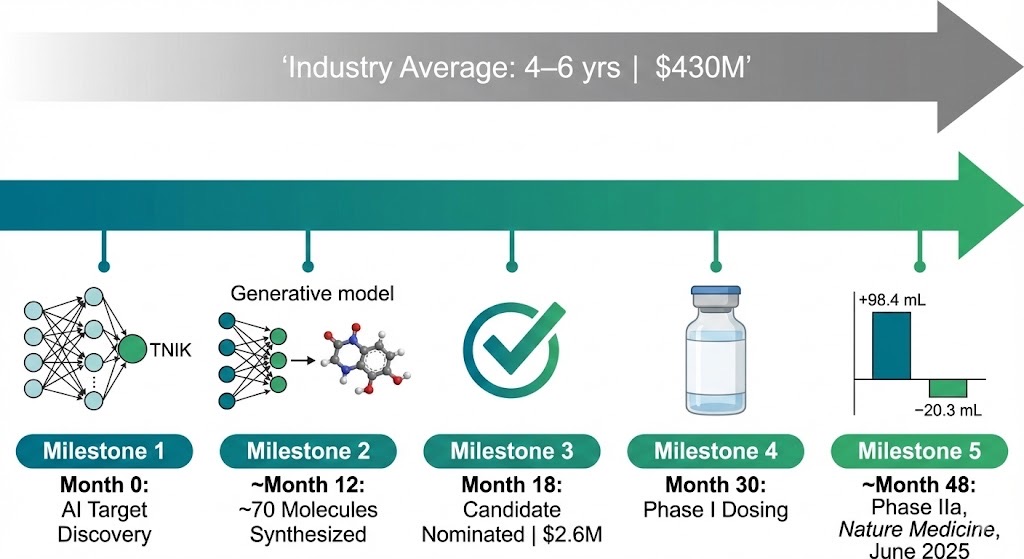
Insilico Medicine's generative AI platform compressed the traditional drug discovery timeline from years to months: rentosertib advanced from AI-identified target to positive Phase IIa results in Nature Medicine in under four years at a fraction of industry-average cost.
From 2021 to 2024, Insilico nominated 22 preclinical developmental candidates across its platform, with an average time to nomination of approximately 13 months and roughly 70 molecules synthesized per program. Ten programs have reached the clinical stage. This is not theoretical efficiency—it is measurable, published, peer-reviewed acceleration of the drug development process.
Insilico's trajectory illustrates a critical point about the digital twin paradigm: the technology's power is not confined to any single scale. The same computational logic that allows Unlearn.AI to simulate a patient's placebo trajectory or Nova In Silico to predict a Phase III outcome also allows Insilico to model molecular interactions and design novel therapeutics. When these molecular, organ, and patient-level twins eventually converge into integrated systems, the result will be a drug development pipeline that is computational from end to end.
7. The Regulatory Landscape: FDA, EMA, and the Avicenna Alliance
No technology in medicine advances without regulatory scaffolding, and digital twins are no exception. The good news is that regulators are leaning in, not pulling back.
The FDA has been progressively embracing computational modeling and simulation. In 2024, the Reagan-Udall Foundation published a strategic report calling in silico technologies "a strategic imperative for accelerating breakthroughs and market leadership for FDA-regulated products." The FDA's guidance on Assessing the Credibility of Computational Modeling and Simulation in Medical Device Submissions provides a formal framework for evaluating digital twin-based evidence. And both the EMA's formal qualification of Unlearn.AI's PROCOVA methodology and the FDA's subsequent alignment represent watershed moments—establishing that AI-generated digital twins can be used in primary analyses of pivotal clinical trials.
Europe's Avicenna Alliance—a nonprofit organization dedicated to the adoption of in silico methods in healthcare—has been instrumental in building consensus across academia, industry, and regulatory bodies. Through initiatives like the VPH Institute (Virtual Physiological Human Institute) and collaborations with the European Commission, the Alliance has helped develop roadmaps for regulatory acceptance of computational evidence.
Marco Viceconti, a pioneer in computational biomechanics and a key figure in the VPH Institute, and Liesbet Geris of KU Leuven have published extensively on the "possible contexts of use for in silico trial methodologies," providing a taxonomy that helps regulators and developers speak the same language about what digital twins can and cannot do.
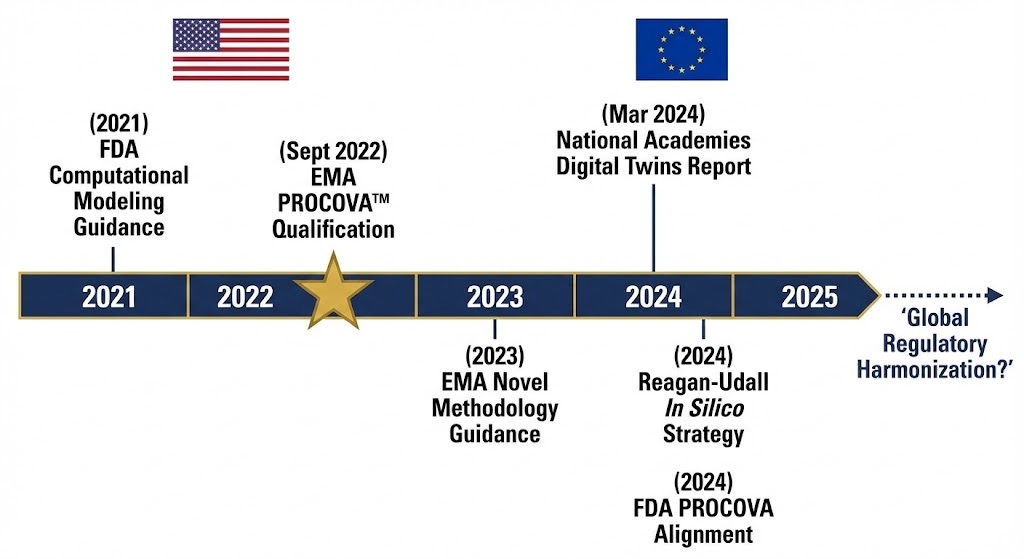
Regulatory milestones from 2021 to 2025 show accelerating institutional acceptance of digital twin methodologies, with the EMA's September 2022 PROCOVA qualification marking the first formal endorsement of AI-generated digital twins for pivotal clinical trial analysis.
8. From Clinical Trials to Your Living Room: What Digital Twins Mean for You
The same computational principles that power digital twins in clinical trials are now being translated into personal health and performance optimization—and this is where the story becomes deeply relevant to every reader.
Consider the data streams that feed a clinical-grade digital twin: genomic sequences, proteomic profiles, continuous wearable data (heart rate, heart rate variability, sleep stages, respiratory rate), imaging studies, blood biomarkers, and lifestyle behaviors. Now consider that a growing number of health-conscious individuals already generate most of this data through services like Function Health (comprehensive blood panels), Viome (microbiome and gene expression), InsideTracker (biomarker optimization), WHOOP and Oura (continuous physiological monitoring), and clinical providers like Fountain Life (full-body MRI, coronary CT, advanced diagnostics).
The problem—as LongevityPlan.AI's founders experienced firsthand—is data fragmentation. Athletes use different wearables, different biomarker providers, and different nutrition apps. Coaches spend 30 to 45 minutes per athlete per week just compiling data before any analysis begins.
This is precisely the gap that a personal digital twin—a Cardiorespiratory Digital Twin™—is designed to close. By integrating disparate data sources into a unified computational model of an individual's physiology, a personal digital twin can do for your health what Unlearn.AI's platform does for a clinical trial: reduce noise, identify signal, predict outcomes, and optimize interventions.
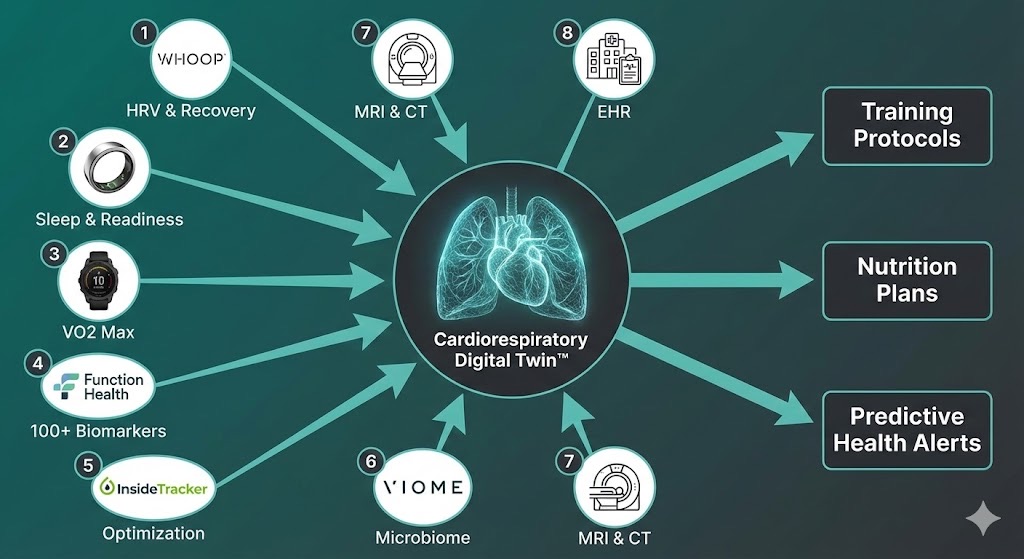
A Cardiorespiratory Digital Twin integrates fragmented data streams from wearables, biomarker panels, genomics, and clinical imaging into a unified computational model, generating personalized training, nutrition, and predictive health recommendations.
Mikael Benson of the Karolinska Institute, whose Medical Digital Twin Research Group published a comprehensive framework in Genome Medicine in February 2025, described digital twins as "global learning health and disease models for preventive and personalized medicine." His team, collaborating with Joseph Loscalzo of Harvard's Brigham and Women's Hospital and Marinka Zitnik of Harvard's Department of Biomedical Informatics, demonstrated how multi-omics integration can reveal that even patients with identical diagnoses may have fundamentally different underlying cellular and molecular mechanisms—a finding with profound implications for treatment selection and, ultimately, longevity planning.
The emerging ecosystem of consumer-facing longevity platforms reflects this convergence. TwinHealth uses digital twin technology specifically for metabolic disease reversal. Deep Longevity, spun out of Alex Zhavoronkov's broader AI aging research portfolio, applies deep learning to aging biomarkers to estimate biological age and project health trajectories. Tally Health, co-founded by epigenetics researcher David Sinclair of Harvard, combines epigenetic testing with personalized lifestyle recommendations.
What distinguishes a genuine digital twin from a dashboard of disconnected metrics is the modeling layer—the computational engine that integrates data, applies physiological constraints, and generates forward-looking predictions. This is the domain where LongevityPlan.AI's approach, grounding its platform in the scientific principles advocated by researchers like Andrew Huberman, Dr. Eric Topol, and Dr. Peter Attia, aims to democratize access to the kind of predictive, personalized planning that was once available only to professional athletes and ultra-high-net-worth individuals.
What the Clinical Trial Revolution Means in Practice
Digital twins in clinical trials are not merely an academic curiosity. They are already generating practical, actionable advances—whether you are a 28-year-old startup founder optimizing sleep with your Oura ring, a 55-year-old CEO scheduling a Fountain Life executive health assessment, or a 70-year-old retiree exploring new Alzheimer's prevention trials.
Faster drug approvals for age-related diseases. Unlearn.AI's digital twin technology is already being applied in trials for Alzheimer's disease, ALS, and Parkinson's disease. ProJenX and Unlearn recently announced a partnership to augment the PRO-101 ALS trial with digital twin models.
More ethical, more inclusive trials. Digital twins can reduce the number of patients assigned to placebo arms without sacrificing statistical power. For conditions where existing therapies are limited—which describes most age-related diseases—this is an ethical imperative.
Personalized dosing and response prediction. As Roche's DT-GPT research demonstrates, large language models adapted for clinical data can forecast individual patient trajectories—predicting not just average outcomes but individual responses. When this technology matures from clinical trials into clinical practice, your physician (or your digital twin platform) could simulate how you specifically might respond to a given therapy, at a given dose, at a given time in your life.
Accelerated biomarker discovery. Clinical trials powered by digital twins are not just testing therapies—they are generating unprecedented amounts of longitudinal patient data that feed back into biomarker discovery.
9. Challenges, Limitations, and Honest Caveats
No rigorous scientific article should omit the limitations, and digital twin technology in clinical trials has real ones.
Data quality and interoperability remain the most persistent challenges. Digital twins are only as good as the data that feeds them. Fragmented electronic health records, inconsistent data standards across institutions, and the "80/20 problem"—where an estimated 80 percent of the technical effort goes into data cleaning and harmonization—are constraints that even the most sophisticated AI cannot fully overcome.
Validation and regulatory trust are still evolving. While the EMA and FDA have provided initial frameworks, there is not yet a global consensus on how to validate a digital twin model for regulatory-grade evidence. The 2024 report by the U.S. National Academies identified "foundational research gaps" that need to be addressed, including standardized credibility assessment methods.
Biological complexity remains humbling. As François-Henri Boissel of Nova In Silico has candidly acknowledged: "We cannot model what we don't know. But we can formulate plausible assumptions to bridge any knowledge gap and validate those assumptions against the expected global behavior of the model."
Privacy and ethics present ongoing challenges. Digital twins require deep, granular personal data. Ensuring that these virtual replicas are used to benefit patients—rather than to discriminate, exploit, or surveil—requires robust governance frameworks that are still being developed.
None of these challenges are disqualifying. They are the predictable friction points of any transformative technology moving from proof-of-concept to widespread deployment. The trajectory is clear; the timeline is the variable.
10. The Road Ahead: 2026 and Beyond
In May 2025, Ehsan Samei's PNAS Nexus roundtable produced a consensus goal for the field: to establish in silico trials and digital twins as "the third pillar" of biomedical evidence, complementing (not replacing) in vitro and in vivo experimentation. The roadmap includes standardized validation frameworks, shared digital patient repositories, regulatory harmonization between the FDA and EMA, and integration with emerging real-world evidence (RWE) platforms.
Key developments to watch include Insilico Medicine's anticipated Phase IIb/III trial of rentosertib in IPF; Unlearn.AI's expansion into oncology and rare disease trials; Nova In Silico's continued validation of the Jinkō platform across multiple therapeutic areas; and Duke CVIT's annual International Summit on Virtual Imaging Trials in Medicine.
For anyone planning a longer, healthier life—and for the ecosystem of companies working to make that possible, from Fountain Life's advanced diagnostic centers to Function Health's comprehensive blood panels to LongevityPlan.AI's Cardiorespiratory Digital Twin™—every therapy that reaches patients faster because of digital twin technology is a therapy that can be incorporated into personalized longevity plans sooner.
The shift from patients to prototypes—from reactive medicine to predictive modeling—is not science fiction. It is peer-reviewed science, regulatory reality, and business inevitability. The question is no longer whether digital twins will redefine clinical trials. It is whether you will plan your health accordingly.