Health Science
·30 min read
Molecular Mystery of Chronic Fatigue
How Disrupted Cellular Energy Production, WASF3 Protein Dysfunction, and AI-Powered Cardiorespiratory Digital Twins™ Are Rewriting the Future of Fatigue Medicine
By Tony Medrano & Sydney Wiredu, LongevityPlan.AI
Abstract
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) affects approximately 1% of the global population—roughly 80 million people worldwide—with debilitating symptoms including profound fatigue, post-exertional malaise, cognitive impairment, and exercise intolerance. For decades, the molecular mechanisms underlying this condition remained elusive, leaving patients without validated biomarkers or effective treatments. However, breakthrough research from 2023-2025 has unveiled a complex biochemical cascade involving mitochondrial dysfunction, endoplasmic reticulum (ER) stress, disrupted ATP production, and the overexpression ofWiskott-Aldrich Syndrome Protein Family Member 3(WASF3). These discoveries, combined with emerging AI-powered digital twin technologies, are transforming chronic fatigue from an enigmatic diagnosis into a targetable, measurable condition amenable to precision medicine interventions. This article examines the cutting-edge chemistry driving chronic fatigue, explores how digital twin technology and AI are enabling personalized fatigue management, and provides a roadmap for athletes, executives, and longevity-focused individuals seeking to optimize their cellular energy production and extend their healthspan.
The Silent Epidemic: Understanding the Scope and Impact of Chronic Fatigue
Imagine waking up each morning feeling as though you've run a marathon overnight. Your muscles ache, your mind feels foggy, and the simple act of climbing stairs leaves you breathless and exhausted for days. This is the daily reality for millions suffering from Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), a debilitating condition that affects approximately 1% of the general population in the United States and an estimated 80 million people globally. Women are affected at a rate three times higher than men, and the condition typically strikes adults between ages 40-60, though it can affect any age group.
The characteristic symptoms of ME/CFS include debilitating fatigue, post-exertional malaise (PEM), unrefreshing sleep, and cognitive impairment—symptoms that also appear in many cases of Long COVID, suggesting shared underlying mechanisms. According to theCenters for Disease Control and Prevention(CDC), ME/CFS causes significant disability, with many patients unable to work or maintain their previous activity levels. The economic impact is staggering: lost productivity, medical costs, anddisability payments associated with ME/CFS exceed $17-24 billion annually in the United States alone.
For high-performing individuals—elite athletes, CEOs, military personnel, and professionals who rely on sustained mental and physical performance—the prospect of chronic fatigue represents not just a health concern but an existential threat to their careers and identities. As one 38-year-old patient who participated in groundbreaking NIH research described it, her fatigue began after contracting infectious mononucleosis at age 16 and progressively worsened, eventually requiring days to recover from simple exercise. Traditional medicine offered few answers and no validated treatments.
However, 2024 and 2025 marked a watershed moment in our understanding of chronic fatigue. A convergence of advanced molecular biology, metabolomics, proteomics, and artificial intelligence has finally begun to illuminate the biochemical darkness at the heart of this condition. The key breakthrough? Identifying specific molecular abnormalities in cellular energy production—particularly involving a protein called WASF3 and its disruption of mitochondrial function—that can be measured, monitored, and potentially targeted for treatment.
The WASF3 Discovery: How a Single Protein Disrupts Cellular Power Plants
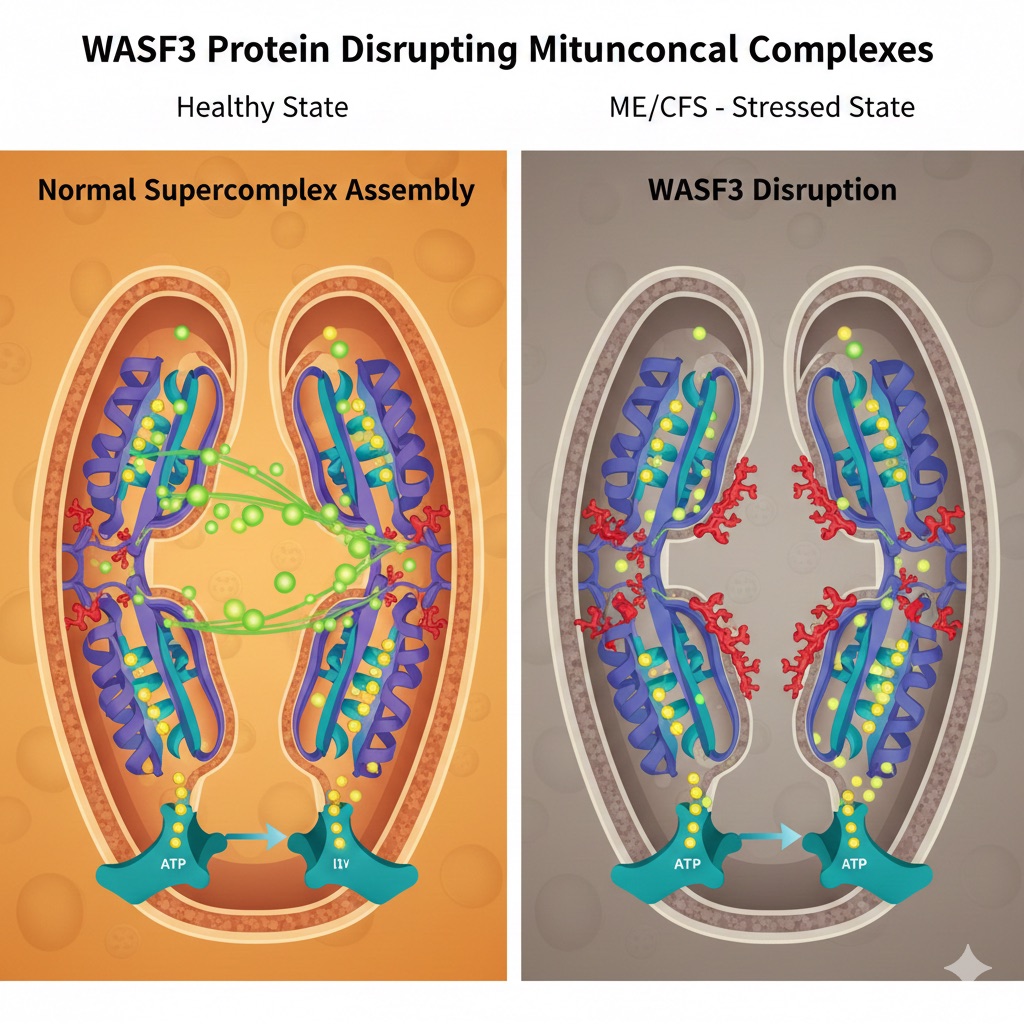
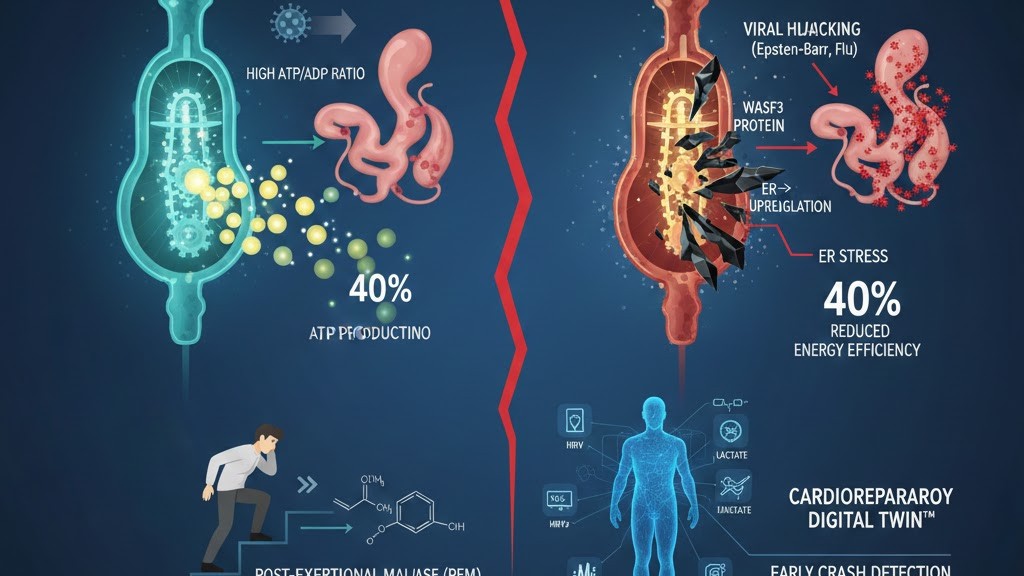
WASF3 protein disrupting mitochondrial supercomplexes: normal assembly in a healthy state versus WASF3 disruption in ME/CFS.
In August 2023, a team led by Dr. Paul M. Hwang at the National Heart, Lung, and Blood Institute (NHLBI) published groundbreaking research in the Proceedings of the National Academy of Sciences that fundamentally altered our understanding of ME/CFS pathophysiology. The study began with a single patient—a 38-year-old woman with lifelong fatigue and exercise intolerance—whose muscle tissue revealed a startling biochemical signature.
Using phosphorus-31 magnetic resonance spectroscopy (31P-MRS), Hwang’s team measured phosphocreatine recovery in the patient’s tibialis anterior muscle after exercise. Phosphocreatine serves as an immediate energy buffer in muscle cells, rapidly regenerating ATP during and after exertion. The patient showed significantly delayed phosphocreatine recovery, indicating impaired mitochondrial ATP synthesis capacity. When the researchers examined her skin fibroblasts in culture, they found reduced oxygen consumption rates—a telltale sign of mitochondrial dysfunction.
Further investigation revealed elevated levels of a protein called Wiskott-Aldrich Syndrome Protein Family Member 3 (WASF3). WASF3 is primarily known for regulating actin polymerization and cell motility, but Hwang’s team discovered it also plays a critical role in mitochondrial function. When they knocked down WASF3 expression in the patient’s cultured cells using RNA interference, mitochondrial function was restored. Conversely, when they genetically engineered mice to overexpress WASF3, the animals showed a 50% reduction in treadmill running capacity despite normal muscle strength—a pattern eerily similar to ME/CFS patients who experience exercise intolerance without apparent muscle weakness.
The molecular mechanism is elegant yet devastating. WASF3 localizes to the contact sites between the endoplasmic reticulum (ER) and mitochondria, where it disrupts the assembly of mitochondrial respiratory supercomplexes—specifically the complex III₂+IV supercomplex (III₂IV) and the complex I+III₂+IV₁ megacomplex (I+III₂IV). These supercomplexes are crucial for efficient electron transfer and ATP production through oxidative phosphorylation. When WASF3 levels rise, it physically interferes with complex IV assembly, reducing cellular oxygen consumption and ATP generation by up to 40%.
To validate these findings beyond a single patient, Hwang collaborated with Dr. Avindra Nath, who was conducting the NIH Intramural ME/CFS Study. They analyzed skeletal muscle biopsies from 14 well-characterized ME/CFS patients and compared them to 10 healthy controls. The results were striking: ME/CFS patients showed approximately 40% higher WASF3 protein levels alongside decreased complex IV subunits (MTCO1 and COX17). The levels of WASF3 showed significant negative correlation with complex IV subunits, confirming the relationship between elevated WASF3 and impaired mitochondrial function.
As Dr. Hwang told Science magazine, "It’s extremely encouraging to see this kind of detailed molecular approach applied to an understudied illness like ME/CFS." The discovery has profound implications: it provides the first validated molecular biomarker for ME/CFS, offers a potential therapeutic target, and explains the hallmark symptom of post-exertional malaise at a mechanistic level. When ME/CFS patients exercise, their already-compromised mitochondria struggle even more to regenerate ATP, triggering a cascade of cellular stress that can last for days.
The Upstream Trigger: Endoplasmic Reticulum Stress and the Viral Connection
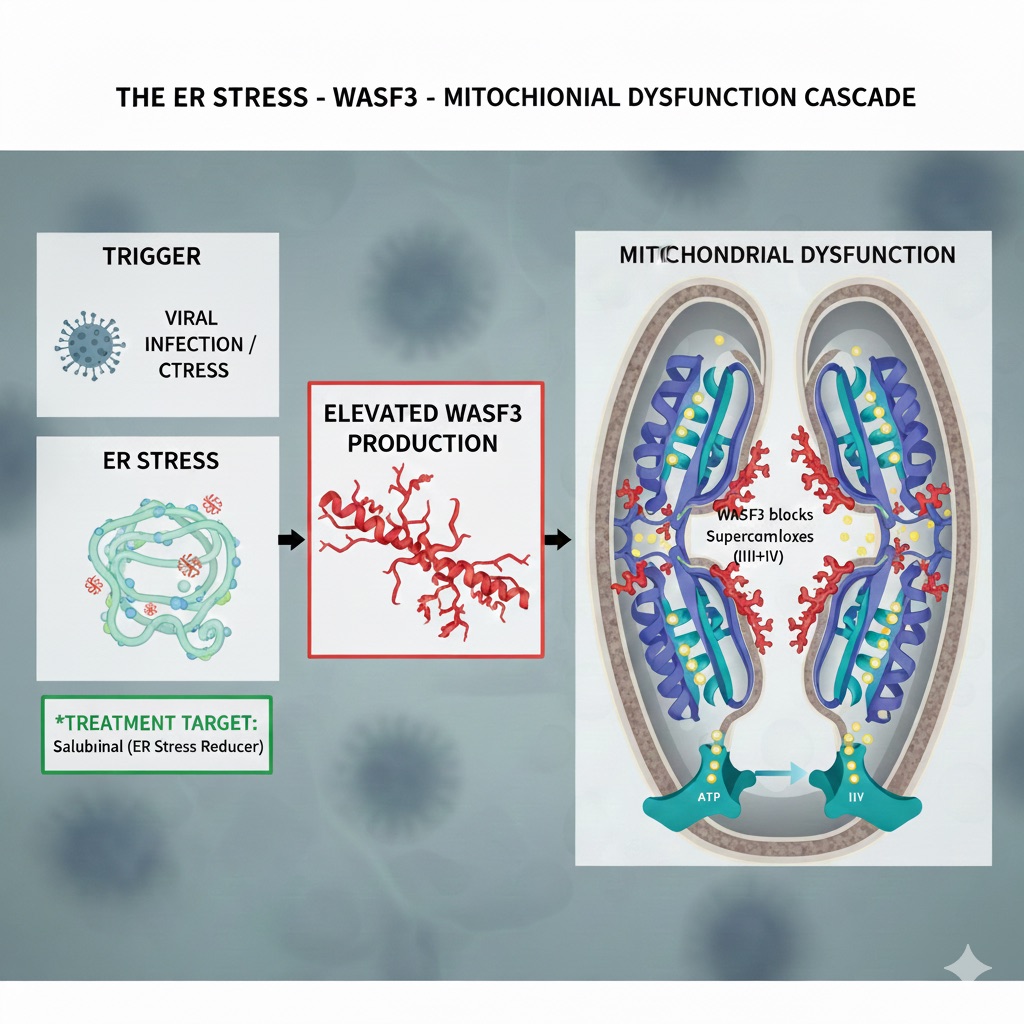
The ER-stress to WASF3 to mitochondrial-dysfunction cascade, with ER-stress reducers such as salubrinal as a potential treatment target.
The discovery of WASF3 dysfunction immediately raised a crucial question: What causes WASF3 levels to rise in the first place? The answer appears to lie in endoplasmic reticulum (ER) stress—a cellular condition that occurs when the ER’s protein-folding machinery becomes overwhelmed.
The endoplasmic reticulum is a vast network of membranous tubules and sacs within cells where proteins are synthesized, folded, and prepared for their cellular roles. When the ER encounters stress—whether from viral infection, inflammatory signals, oxidative damage, or calcium dysregulation—it activates the unfolded protein response (UPR), a sophisticated quality-control system designed to restore normal function. Three major ER stress sensors orchestrate this response: PERK (protein kinase RNA-like ER kinase), IRE1 (inositol-requiring enzyme 1), and ATF6 (activating transcription factor 6).
WASF3 is regulated by BiP (binding immunoglobulin protein, also known as GRP78), an ER chaperone protein that normally keeps ER stress sensors inactive. When ER stress occurs, BiP dissociates from these sensors to help fold accumulating proteins, inadvertently activating the stress response and upregulating WASF3. In Hwang’s study, ME/CFS muscle samples showed significantly higher PERK levels but paradoxically lower BiP levels—a pattern termed "ER Stress Response Failure" that has been associated with metabolic disorders.
The viral connection is particularly intriguing. Many ME/CFS patients report their symptoms began after a viral infection—mononucleosis (Epstein-Barr virus), influenza, or more recently, SARS-CoV-2. Viruses are notorious for usurping the ER machinery to replicate their own proteins, triggering ER stress in the process. The patient in Hwang’s study reported her fatigue started after contracting mononucleosis as a teenager. Similarly, Long COVID patients—many of whom develop ME/CFS-like symptoms—show evidence of persistent ER stress and elevated WASF3.
To test the ER stress-WASF3 connection experimentally, researchers treated human myoblasts (muscle precursor cells) with chemical ER stress inducers like tunicamycin and thapsigargin. WASF3 protein levels increased proportionally with ER stress intensity. They also induced ER stress in mice using endotoxin (lipopolysaccharide), which is known to cause fatigue in humans. These mice showed elevated WASF3 and decreased complex IV levels in skeletal muscle, recapitulating the ME/CFS phenotype.
Critically, when researchers treated the patient’s cells with salubrinal—a small molecule that inhibits ER stress by blocking eIF2α dephosphorylation—WASF3 levels decreased and mitochondrial function improved. This finding suggests that targeting ER stress could be a viable therapeutic strategy for ME/CFS. Dr. Hwang’s team is now exploring drugs that reduce ER stress or directly inhibit WASF3 as potential treatments, with plans for clinical trials.
The Energy Crisis: ATP Depletion, ADP/AMP Accumulation, and Cellular Exhaustion
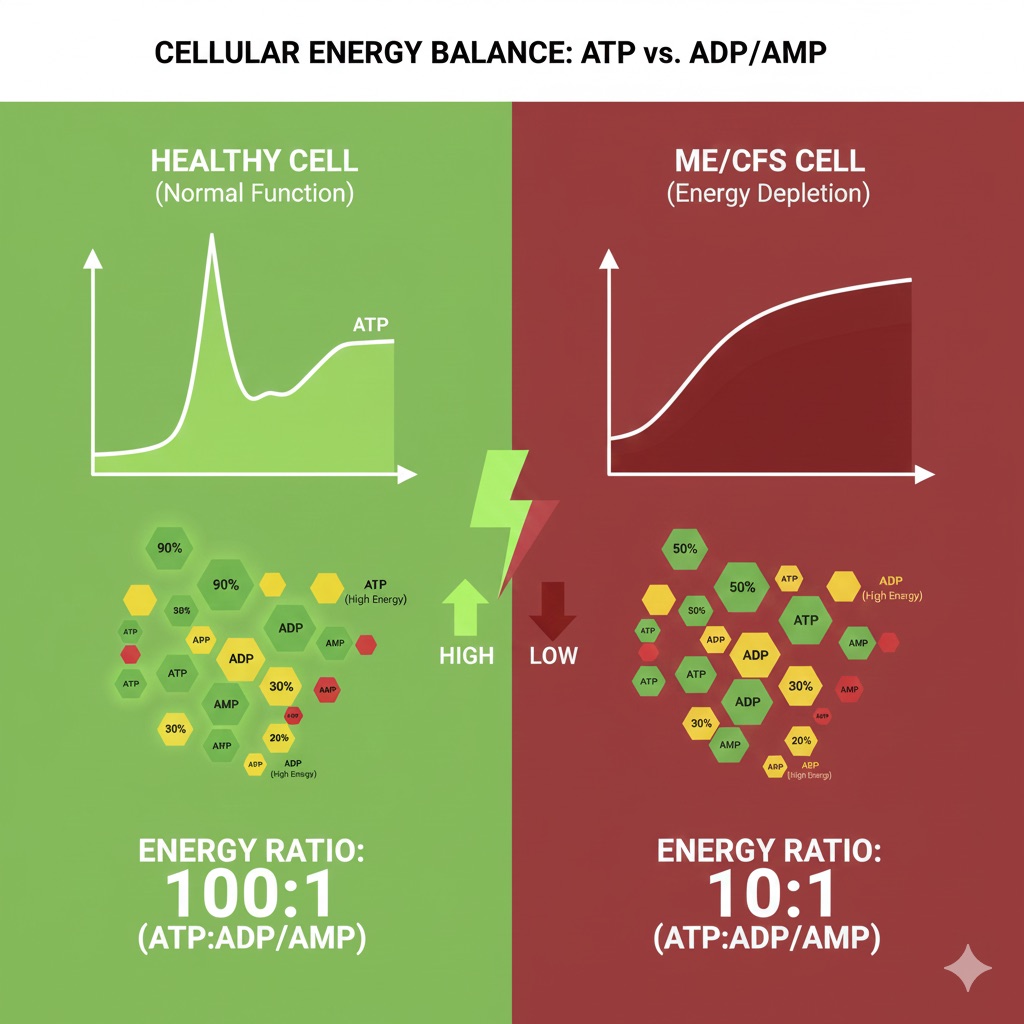
Cellular energy balance: a healthy cell holds an ATP:ADP/AMP ratio near 100:1, versus roughly 10:1 in energy-depleted ME/CFS cells.
At the molecular heart of chronic fatigue lies a fundamental disruption in cellular energy metabolism. Adenosine triphosphate (ATP) is the universal energy currency of life—every muscle contraction, nerve impulse, protein synthesis, and cellular repair process requires ATP hydrolysis to release energy. In healthy individuals, mitochondria continuously regenerate ATP through oxidative phosphorylation, maintaining cellular ATP/ADP ratios around 100:1. In ME/CFS patients, this delicate balance collapses.
A landmark 2025 study published in Cell Reports Medicine examined immune cells from ME/CFS patients and found elevated levels of adenosine monophosphate (AMP) and adenosine diphosphate (ADP) with correspondingly reduced ATP/ADP ratios—a clear signature of cellular energy stress. When mitochondria fail to produce sufficient ATP, cells accumulate ADP (which has two phosphate groups) and AMP (one phosphate group), triggering an energy crisis that affects every cellular system.
The accumulation of AMP activates AMP-activated protein kinase (AMPK), a master metabolic regulator that senses energy depletion. AMPK activation initiates an emergency metabolic shift: it shuts down energy-consuming anabolic processes (protein synthesis, cell division) and activates energy-generating catabolic pathways (fatty acid oxidation, glucose uptake). While beneficial in acute situations, chronic AMPK activation—as seen in ME/CFS—leads to cellular exhaustion and impaired function.
The impaired ATP production in ME/CFS stems from multiple converging mechanisms. First, WASF3 disruption of complex IV directly reduces electron transport chain efficiency, decreasing the proton gradient across the inner mitochondrial membrane that drives ATP synthase. Second, chronic oxidative stress damages mitochondrial proteins and lipids, further impairing function. Third, altered calcium handling disrupts the TCA (tricarboxylic acid) cycle enzymes that generate NADH and FADH₂—the electron carriers that fuel the respiratory chain.
A 2025 study using 7 Tesla magnetic resonance spectroscopy examined brain and muscle chemistry in ME/CFS patients versus healthy controls. ME/CFS patients showed elevated lactate levels in both the pregenual and dorsal anterior cingulate cortex—brain regions critical for motivation, attention, and pain processing. Elevated lactate indicates a metabolic shift toward glycolysis (anaerobic energy production) and away from oxidative phosphorylation, consistent with mitochondrial dysfunction. Notably, skeletal muscle metabolites at rest did not differ significantly between groups, suggesting the energy deficit becomes most apparent during cognitive tasks and physical exertion.
Post-exertional malaise (PEM)—the worsening of symptoms following physical or mental exertion—can now be understood at a molecular level. Exercise increases cellular ATP demand dramatically. In healthy individuals, mitochondria ramp up oxidative phosphorylation to meet this demand, and ATP reserves recover within minutes to hours. In ME/CFS patients with WASF3-disrupted mitochondria, the system cannot respond adequately. ATP depletion triggers a cascade: accumulation of metabolic byproducts (AMP, inorganic phosphate, hydrogen ions), activation of nociceptive pain pathways, inflammatory cytokine release, and oxidative damage. Recovery requires days rather than hours because damaged mitochondrial components must be repaired or replaced through mitophagy and biogenesis—processes that themselves require ATP.
The Kynurenine Pathway: NAD+ Deficiency and the Tryptophan-Serotonin Imbalance
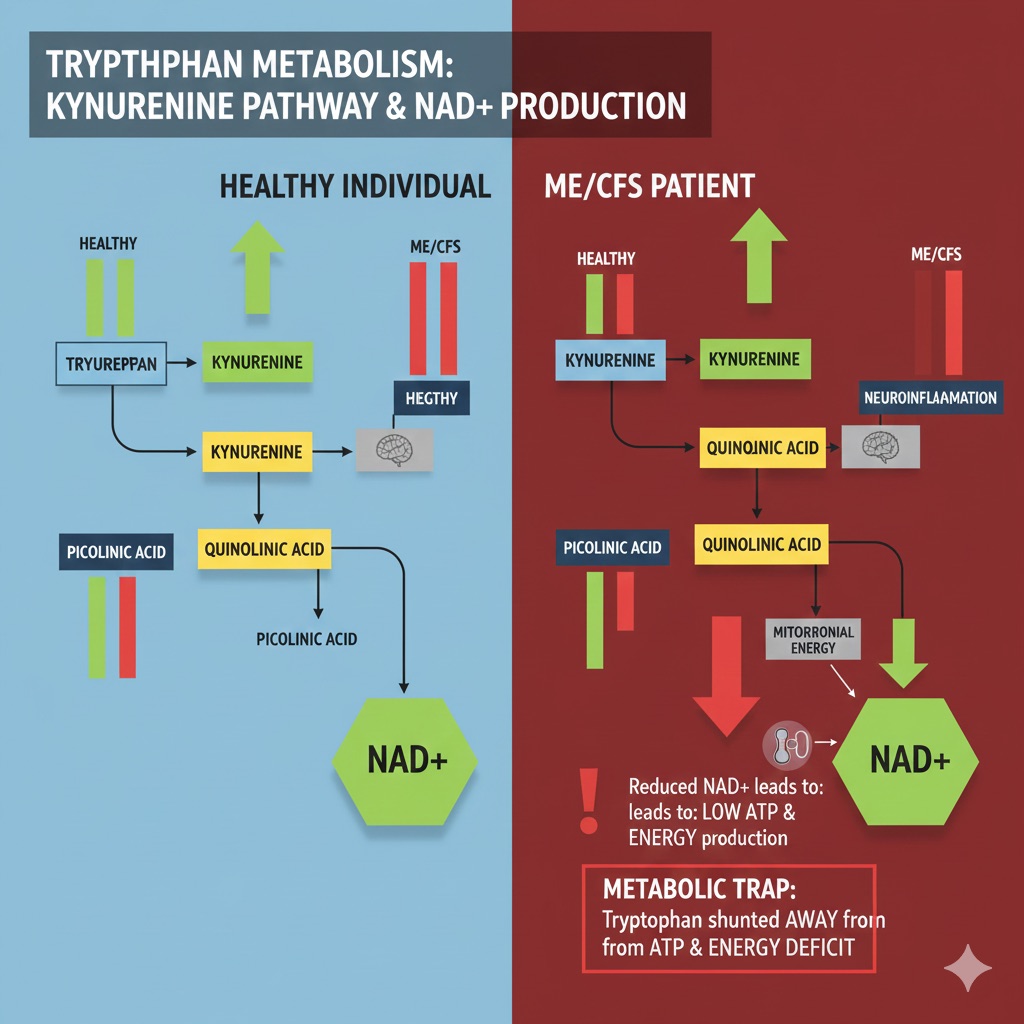
Tryptophan metabolism and the kynurenine pathway: impaired NAD+ production in ME/CFS shunts tryptophan away from ATP and energy.
Beyond ATP, another critical metabolic pathway implicated in ME/CFS involves tryptophan catabolism through the kynurenine pathway (KP)—the sole de novo synthesis route for nicotinamide adenine dinucleotide (NAD+), an essential cofactor for over 500 enzymatic reactions including mitochondrial oxidative phosphorylation.
Tryptophan, an essential amino acid obtained from diet, can be metabolized along three major pathways: the serotonin-melatonin pathway (5%), the tetrahydrobiopterin pathway, and the kynurenine pathway (90-95%). In ME/CFS patients, multiple studies have documented significant alterations in KP metabolites, with profound implications for both energy metabolism and neurological function.
The kynurenine pathway begins when tryptophan is converted to kynurenine by either tryptophan 2,3-dioxygenase (TDO), primarily in the liver, or indoleamine 2,3-dioxygenase (IDO-1), which is expressed in many tissues and strongly induced by inflammatory cytokines like interferon-gamma (IFN-γ) and tumor necrosis factor-alpha (TNF-α). Kynurenine then branches into multiple metabolites: 3-hydroxykynurenine (3-HK), kynurenic acid (KYNA), 3-hydroxyanthranilic acid (3-HAA), quinolinic acid (QUIN), and finally NAD+.
A 2025 multi-omics study published in Cell Reports Medicine found ME/CFS patients had higher 3-hydroxykynurenine (34.29 nM vs. 26.67 nM in controls) and lower kynurenic acid (23.38 nM vs. 30.26 nM), consistent with elevated kynurenine monooxygenase (KMO) activity. More critically, patients showed lower levels of picolinic acid (PIC: 141.8 nM vs. 208 nM) and quinolinic acid (QUIN: 412.5 nM vs. 463.5 nM)—the direct precursors to NAD+. The net effect reduces systemic availability of quinolinic acid, the substrate for NAD+ generation, potentially explaining the NAD+ deficiency documented in ME/CFS.
NAD+ is absolutely critical for mitochondrial function. It serves as the primary electron acceptor in the electron transport chain, accepting electrons from complex I (NADH dehydrogenase) and shuttling them through the respiratory complexes. Without adequate NAD+, oxidative phosphorylation grinds to a halt. NAD+ also serves as a cofactor for sirtuins—a family of longevity-associated proteins that regulate mitochondrial biogenesis, inflammation, and cellular stress responses. SIRT1, for example, deacetylates PGC-1α (peroxisome proliferator-activated receptor gamma coactivator 1-alpha), the master regulator of mitochondrial biogenesis. Low NAD+ levels impair this process, preventing cells from generating new, healthy mitochondria to replace damaged ones.
The kynurenine pathway also produces neuroactive metabolites with opposing effects. Quinolinic acid is an NMDA receptor agonist that, in excess, causes excitotoxicity—overstimulation of neurons leading to calcium influx and cell death. Kynurenic acid, conversely, is an NMDA receptor antagonist with neuroprotective properties. The ratio of these metabolites may influence the cognitive symptoms (“brain fog”) characteristic of ME/CFS. Moreover, increased flux through the kynurenine pathway diverts tryptophan away from serotonin synthesis, potentially contributing to mood disturbances and sleep dysfunction seen in ME/CFS patients.
A 2024 study in Molecular Neurobiology examined KP metabolites, inflammatory cytokines, and proteomics in ME/CFS patients. The researchers found not only disturbed KP metabolite levels but also decreased hepcidin (nearly by half), an iron-regulating hormone that responds to inflammation. Low hepcidin might reflect systemic iron deficiency or ongoing hypoxia—both of which would further compromise mitochondrial function since iron is essential for heme synthesis and cytochrome assembly in respiratory complexes.
Oxidative Stress and Reactive Oxygen Species: The Vicious Cycle of Mitochondrial Damage
Mitochondrial dysfunction and oxidative stress form a self-reinforcing cycle in ME/CFS, each exacerbating the other. A landmark 2025 study published in the Proceedings of the National Academy of Sciences (PNAS) examined lymphocytes from 25 healthy controls, 27 ME/CFS patients, and 20 Long COVID patients, revealing that both ME/CFS and Long COVID patients exhibited signs of elevated oxidative stress, particularly in memory immune cell subsets.
The study used a sophisticated combination of flow cytometry, RNA sequencing, mass spectrometry, and systems chemistry analysis to identify aberrations in reactive oxygen species (ROS) clearance pathways. ME/CFS patients showed elevated glutathione levels—seemingly paradoxical until one considers this represents a compensatory response to overwhelming oxidative stress. Glutathione (γ-glutamyl-cysteinyl-glycine) is the cell’s primary antioxidant defense, with reduced glutathione (GSH) neutralizing ROS by donating electrons, thereby becoming oxidized (GSSG). The GSH/GSSG ratio serves as a key indicator of cellular redox state.
Critically, the study found decreased mitochondrial superoxide dismutase (SOD2) protein levels in ME/CFS patients. SOD2 is a manganese-dependent enzyme located in the mitochondrial matrix that converts superoxide radicals (O₂•⁻) into hydrogen peroxide (H₂O₂), which is then detoxified by glutathione peroxidase and catalase. Reduced SOD2 allows superoxide to accumulate, where it can react with nitric oxide (NO) to form peroxynitrite (ONOO⁻), a highly reactive species that nitrosylates proteins, lipids, and DNA, causing extensive cellular damage.
The study also identified glutathione peroxidase 4 (GPX4)-mediated lipid peroxidation damage. GPX4 protects against ferroptosis—a form of programmed cell death triggered by iron-dependent lipid peroxidation. When GPX4 activity is compromised (either through selenium deficiency, glutathione depletion, or direct oxidative damage), polyunsaturated fatty acids in cell membranes undergo peroxidation, generating toxic lipid peroxides and aldehydes. Mitochondrial membranes, rich in cardiolipin (a phospholipid containing four fatty acid chains), are particularly vulnerable to this damage.
The source of excessive ROS in ME/CFS appears multifactorial. First, when electron transport through complexes I-IV is impaired (as occurs with WASF3 disruption), electrons “leak” from the respiratory chain, reducing molecular oxygen directly to form superoxide. Second, damaged respiratory complexes themselves become ROS generators, creating a feed-forward loop. Third, inflammatory cytokines activate NADPH oxidases in immune cells, generating additional ROS as part of the innate immune response.
The consequences of chronic oxidative stress extend beyond mitochondria. ROS damage nuclear and mitochondrial DNA, potentially causing mutations that impair mitochondrial gene expression. They modify proteins through carbonylation and nitrosylation, altering enzyme function. They activate inflammatory signaling pathways including NF-κB, perpetuating a pro-inflammatory state. Perhaps most insidiously, ROS promote mitochondrial fission—the process by which large, interconnected mitochondrial networks fragment into smaller, less efficient units.
A 2025 study published in Cell Reports Medicine found that ME/CFS patients exhibited enhanced dephosphorylation of Drp1 (dynamin-related protein 1) at serine residues 616 and 637, enhancing Drp1 GTPase activity and promoting mitochondrial fission. Fragmented mitochondria have reduced capacity for oxidative phosphorylation, produce more ROS, and are preferentially targeted for degradation via mitophagy. While mitophagy removes damaged mitochondria, excessive fission and mitophagy can deplete the mitochondrial pool, particularly when biogenesis (creation of new mitochondria) is impaired.
Immune Dysregulation: How Chronic Inflammation and T-Cell Exhaustion Perpetuate Energy Deficiency
The intersection of immune dysfunction and cellular energetics represents one of the most fascinating aspects of ME/CFS pathophysiology. A 2024-2025 synthesis of research reveals that immune cells in ME/CFS patients are both hyperactivated and metabolically exhausted—a paradoxical state with profound implications.
The immune system accounts for 15-20% of daily energy expenditure in healthy humans, increasing to approximately 25% during serious infections. This enormous energy demand reflects the metabolic costs of immune cell proliferation, cytokine production, antibody synthesis, and the oxidative burst used to kill pathogens. In ME/CFS, evidence suggests the immune system remains chronically activated, continuously draining precious ATP reserves.
A 2025 study in Cell Reports Medicine revealed multiple immunological abnormalities in ME/CFS. Immunophenotyping showed significant changes in natural killer (NK) cell and dendritic cell (DC) populations. ME/CFS patients had smaller populations of CD56low CD16+ NK cells, which are the cytotoxic subset responsible for killing virus-infected and tumor cells. This finding is consistent with numerous prior studies documenting NK cell dysfunction in ME/CFS, potentially explaining increased susceptibility to infections.
T-cell abnormalities are particularly striking. Research by Dr. Maureen Hanson at Cornell University suggests ME/CFS patients’ T-cells may have been epigenetically reprogrammed by viral infection to become exhausted—a state characterized by reduced proliferation, impaired cytokine production, and expression of inhibitory receptors like PD-1 (programmed death-1) and CTLA-4. T-cell exhaustion typically occurs during chronic viral infections when persistent antigen stimulation drives cells into a hyporesponsive state.
A 2025 npj Metabolic Health and Disease study reported an exaggerated innate immune response in ME/CFS after exposure to microbial antigens. When researchers stimulated immune cells with bacterial lipopolysaccharide or fungal zymosan before and after exercise, ME/CFS patients showed heightened cytokine production—particularly interleukin-6 (IL-6), IL-1β, and TNF-α. This hyperresponsiveness suggests immune cells are primed or “trained” to overreact, possibly due to epigenetic modifications in promoter regions of inflammatory genes.
The connection between immune activation and mitochondrial dysfunction is bidirectional. On one hand, mitochondrial dysfunction impairs immune cell function—T-cells with damaged mitochondria cannot produce sufficient ATP for clonal expansion and cytokine secretion. On the other hand, chronic immune activation depletes cellular energy reserves. The metabolic shift induced by WASF3 overexpression—suppressing oxidative phosphorylation while promoting glycolysis—may initially support innate immune activation (which relies heavily on glycolysis), but becomes maladaptive when sustained chronically.
Autoimmunity also features prominently in ME/CFS. Individuals with the condition possess autoantibodies against neurotransmitters (serotonin, dopamine), gangliosides, muscarinic receptors, and serotonin receptor 5-HT1A. A 2025 study published in medRxiv demonstrated that immunoglobulin G (IgG) isolated from ME/CFS patients selectively induces mitochondrial fragmentation in human endothelial cells when transferred to cell cultures. The intact IgG molecule triggered this effect, but when cleaved into Fab and Fc fragments, the Fab fragment alone could alter mitochondrial energetics while the Fc fragment induced a hypometabolic phenotype characterized by reduced ATP content. This suggests some ME/CFS patients develop autoantibodies that directly target mitochondrial or endothelial cell proteins.
The gut microbiome represents another immunometabolic nexus in ME/CFS. Studies have documented dysbiosis—altered microbial composition—with reduced populations of butyrate-producing bacteria. Butyrate, a short-chain fatty acid produced by bacterial fermentation of dietary fiber, serves as the primary fuel for colonocytes and exerts anti-inflammatory effects systemically. Reduced butyrate production may compromise intestinal barrier integrity (“leaky gut”), allowing bacterial translocation that triggers chronic inflammation and autoimmunity. The 2025 Cell Reports Medicine study found that 5 of the 7 most significantly modulated proteins in ME/CFS patient plasma had roles in maintaining gut health, underscoring the importance of the gut-systemic axis.
AI-Powered Digital Twins: The Cardiorespiratory Digital Twin™ Revolution in Fatigue Management
An AI-powered Cardiorespiratory Digital Twin integrates wearable, biomarker, and energy-budget data for personalized fatigue management.
The molecular complexity of chronic fatigue—involving mitochondrial dysfunction, oxidative stress, immune dysregulation, metabolic pathway disruptions, and neurotransmitter imbalances—demands a radically different approach to diagnosis and treatment. Enter artificial intelligence and digital twin technology: the marriage of personalized data collection with predictive computational modeling that is transforming ME/CFS from a mystery into a manageable condition.
A digital twin is a virtual replica of a physical system that is continuously updated by real-world data, enabling simulation, prediction, and optimization without direct intervention on the actual system. Originally developed by NASA in 2002 for spacecraft lifecycle management, digital twins have evolved into dynamic, AI-integrated systems capable of mirroring complex adaptive systems—including the human body.
The healthcare digital twin market is experiencing explosive growth. According to 2024-2025 industry reports, 66% of healthcare executives plan to invest in digital twin technologies over the next three years, with the global market projected to grow at a compound annual growth rate exceeding 30% between 2023 and 2027. By 2025, approximately 25% of all digital transformation initiatives in healthcare are expected to incorporate digital twins. As of 2024, 86% of organizations across various industries view digital twins as core to their digital innovation strategies.
For ME/CFS and chronic fatigue management, the Cardiorespiratory Digital Twin™ represents a particularly promising application. This specialized digital twin integrates multi-modal data—wearable device metrics (heart rate variability, oxygen saturation, sleep stages, activity levels), biomarker panels (ATP/ADP ratios, lactate, NAD+ levels, kynurenine metabolites, inflammatory cytokines), genetic information (mitochondrial haplogroups, oxidative stress pathway polymorphisms), and clinical assessments (exercise testing, cognitive function, symptom severity)—into a unified computational model.
The power of AI-enabled digital twins lies in their ability to identify patterns invisible to human clinicians. Machine learning algorithms can detect subtle correlations between wearable data signatures and impending crashes (severe PEM episodes). For example, research has shown that ME/CFS patients exhibit characteristic heart rate variability patterns—reduced high-frequency power, elevated low-frequency/high-frequency ratios—indicating autonomic nervous system dysfunction. A Cardiorespiratory Digital Twin™ continuously monitoring HRV could alert patients when parameters drift into danger zones, prompting preemptive rest.
Companies likeFountain Life, co-founded byPeter DiamandisandTony Robbins, are pioneering comprehensive diagnostic approaches that generate 150GB of imaging and genetic data per member. Their platform combines AI-enhanced full-body MRI, coronary CT angiography, advanced blood biomarker panels (including mitochondrial function tests), genomic analysis, and microbiome testing. Members receive access to Zori AI, a personalized AI medical assistant that analyzes health data and optimizes longevity strategies. For ME/CFS patients, such comprehensive phenotyping could identify mitochondrial dysfunction before debilitating symptoms emerge.
Viome, founded byNaveen Jain, takes a complementary approach focused on RNA sequencing of gut and oral microbiomes. Unlike traditional microbiome testing that only identifies which organisms are present, Viome uses metatranscriptomics to measure what those organisms are actually doing—which metabolic pathways are active. For ME/CFS patients with gut dysbiosis and reduced butyrate production, Viome’s AI-driven platform (trained on hundreds of thousands of users) can provide personalized dietary recommendations to restore beneficial microbial metabolism.
TruDiagnostic has pioneered epigenetic methylation testing using DNA analysis that examines over 950,000 loci to measure biological age through sophisticated algorithms including the DunedinPoAm (Pace of Aging) and partnerships with Harvard and Yale universities. Their platform provides an 85+ page report with machine learning-driven recommendations. For ME/CFS patients, biological aging acceleration has been documented, and epigenetic clocks could track treatment efficacy—successful interventions should slow or reverse epigenetic aging.
Deep Longevity, a spin-off of Insilico Medicine, uses deep neural networks to develop biological age clocks across multiple data types—blood biochemistry, cell counts, protein-coding gene expression, and gut bacteria composition. Their portfolio of AI-powered aging clocks provides comprehensive age tracking. For ME/CFS, comparing biological ages across different systems (immune age, metabolic age, mitochondrial age) could reveal which systems are most affected and prioritize interventions.
InsideTracker, co-founded with longevity expertDr. David Sinclairon its scientific advisory board, uses algorithms based on extensive human population studies (not animal models) to predict biological age from blood biomarkers and provide personalized nutrition and lifestyle recommendations.GlycanAgemeasures biological age through glycan analysis of immunoglobulin G, revealing immune system aging. In comparative research, GlycanAge was one of the best predictors of future hospitalization across the broadest range of diseases, outperforming 11 other molecular aging clocks. For ME/CFS patients with immune dysfunction, glycan patterns could serve as sensitive biomarkers of disease activity.
A 2025 study from theWeizmann Institute of Science, published in Nature Medicine, demonstrated the power of AI-generated digital twins for predictive medicine. Researchers fromProf. Eran Segal’s laboratory analyzed extensive medical information from the Human Phenotype Project, creating personalized digital twins that could detect disease risk, initiate preventive treatment, and simulate which treatment would be most effective. The system essentially allows “what-if” testing—trying different interventions virtually before implementing them physically.
For ME/CFS specifically, this predictive capability is transformative. Imagine a patient whose Cardiorespiratory Digital Twin™ indicates declining mitochondrial function based on wearable data trends, biomarker shifts, and activity patterns. The AI could simulate responses to various interventions: NAD+ precursor supplementation (nicotinamide riboside), CoQ10 augmentation, ER stress reducers (low-dose salubrinal analogs), pacing strategies (structured activity management), or targeted anti-inflammatory protocols. The digital twin would predict which intervention—or combination—offers the highest probability of benefit for that individual’s specific biochemical profile.
LongevityPlan.AI represents the next evolution in this space. Founded by Tony Medrano (3x Ironman finisher, 3x tech CEO with Harvard, Columbia, and Stanford degrees),Lina Ramos(35x Ironman finisher including 2026 Kona qualification, Stanford MBA), andFelipe Loureiro(600+ triathlon finisher, 40+ years coaching experience), the platform integrates wearable data, biomarkers, medical records, and lifestyle activities into a personalized Cardiorespiratory Digital Twin™—an AI-powered software replica that mirrors the human body to predict, optimize, and personalize health, recovery, and performance in real-time.
The platform was born from real-world challenges in elite endurance training. After decades competing and coaching, the founders experienced firsthand the data fragmentation crisis: athletes use different wearables (ŌURA, WHOOP, Garmin), different biomarker providers (Function Health, InsideTracker, Viome), and different nutrition apps. Coaches spent 30-45 minutes per athlete per week just compiling data before analysis could begin. They knew there had to be a better way. The solution: AI-powered integration that consolidates multi-source data, identifies patterns, and generates actionable insights automatically.
For ME/CFS patients and individuals concerned about chronic fatigue, the LongevityPlan.AI approach offers several advantages. First, continuous monitoring detects energy depletion patterns before crashes occur. Second, the AI learns each individual’s unique physiology—their personal ATP production capacity, oxidative stress tolerance, inflammatory thresholds—and adjusts recommendations accordingly. Third, the platform democratizes elite sports science, making NFL and Ironman-level performance optimization accessible to anyone seeking to extend their healthspan.
From Bench to Bedside: Emerging Therapeutic Strategies and Clinical Trials
The molecular insights gained from 2023-2025 research are rapidly translating into potential therapeutic strategies. While no FDA-approved treatments currently exist for ME/CFS, multiple promising interventions are in preclinical or early clinical testing, guided by digital biomarker monitoring.
Targeting ER Stress: Given the clear connection between ER stress and WASF3 overexpression, compounds that alleviate ER stress represent logical therapeutic candidates. Salubrinal, which blocked WASF3-induced mitochondrial dysfunction in Hwang’s research, inhibits eIF2α dephosphorylation, thereby reducing protein synthesis load on the ER. While salubrinal itself has poor pharmacokinetics for clinical use, pharmaceutical companies are developing second-generation ER stress modulators with improved properties. Tauroursodeoxycholic acid (TUDCA), a bile acid with ER stress-reducing properties, is already available as a supplement and has shown promise in various conditions involving ER stress. Dr. Hwang’s team is evaluating drugs that reduce ER stress or directly inhibit WASF3 for future clinical trials.
NAD+ Augmentation: Multiple NAD+ precursors are being investigated for ME/CFS. Nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) are direct NAD+ precursors that bypass the dysfunctional kynurenine pathway. Studies in animal models and preliminary human trials show these compounds can boost tissue NAD+ levels by 25-100%, improve mitochondrial function, reduce oxidative stress, and extend lifespan. For ME/CFS patients with documented NAD+ deficiency, supplementation could provide substrate-level support for ATP production.
Mitochondrial Support: Coenzyme Q10 (CoQ10) serves as an electron carrier between complexes I/II and complex III in the respiratory chain. Studies have found deficiencies in CoQ10 and NADH (the reduced form of NAD+) in ME/CFS patients. Optimal levels are required for oxidative phosphorylation and ATP production. Clinical trials testing CoQ10 supplementation (typically 200-400 mg daily in the ubiquinol form for better absorption) have shown modest improvements in fatigue and exercise tolerance. Combining CoQ10 with L-carnitine (which transports fatty acids into mitochondria for β-oxidation) may provide synergistic benefits.
Antioxidant Strategies: Given the clear evidence of oxidative stress, targeted antioxidant interventions merit investigation. N-acetylcysteine (NAC) serves as a glutathione precursor and has shown benefits in various oxidative stress-related conditions. Alpha-lipoic acid (ALA) functions as a universal antioxidant in both aqueous and lipid environments and regenerates other antioxidants including glutathione and vitamin E. Mitochondria-targeted antioxidants like MitoQ and SkQ1, which concentrate in mitochondrial membranes due to their lipophilic cation structure, may provide superior protection against mitochondrial ROS damage.
Immunomodulation: For patients with evidence of autoimmunity or persistent immune activation, immunomodulatory approaches may be beneficial. Low-dose naltrexone (LDN), an opioid receptor antagonist at low doses (1.5-4.5 mg), has anti-inflammatory properties and has shown promise in several autoimmune conditions. Rituximab, a monoclonal antibody that depletes B-cells, showed initial promise in small ME/CFS trials, though larger studies yielded mixed results. Selective targeting of specific inflammatory pathways—such as IL-6 blockade or JAK-STAT inhibition—based on individual cytokine profiles identified through digital twin monitoring could provide more precise immunomodulation.
Exercise as Medicine (With Critical Caveats): Traditional graded exercise therapy (GET) has proven harmful for many ME/CFS patients because it fails to respect energy limitations and can trigger severe crashes. However, carefully titrated, personalized exercise protocols guided by digital twin monitoring show promise. The key is maintaining activity levels below the anaerobic threshold—the point where lactate accumulation begins, indicating inadequate oxygen delivery or mitochondrial capacity. Cardiorespiratory Digital Twin™ technology can identify this threshold precisely through continuous monitoring and adjust recommendations dynamically. Very gentle movement—perhaps as little as 5-10 minutes of recumbent cycling or swimming at 40-50% of maximum heart rate—may stimulate mitochondrial biogenesis signals (PGC-1α activation) without depleting energy reserves.
Pacing and Energy Management: Perhaps the most immediately actionable intervention is sophisticated pacing—balancing activity and rest to stay within energy budgets. Digital twins excel at this application. By tracking real-time energy expenditure (via heart rate, activity sensors, oxygen consumption estimates) and comparing it against individualized energy production capacity (derived from biomarker data and previous activity-recovery patterns), AI systems can provide instant feedback: “You have 15 minutes of moderate activity remaining in your energy budget today” or “Your current activity level is 10% above sustainable; reduce intensity to avoid crash.” This transforms pacing from guesswork into precision medicine.
Beyond Disease Management: Chronic Fatigue Science for Longevity and Peak Performance
The molecular insights from chronic fatigue research extend far beyond ME/CFS treatment—they provide a roadmap for anyone seeking to optimize cellular energy production, extend healthspan, and maintain peak performance throughout life. As Dr. Andrew Huberman, Dr. Peter Attia, and Dr. Eric Topol emphasize, mitochondrial function, metabolic flexibility, and oxidative stress management are foundational to healthy aging.
Elite athletic organizations have long understood this connection. The NBA, NFL, US Olympic Team, and Stanford Athletics employ sophisticated biomarker monitoring, metabolomics, and performance analytics to maximize player longevity and minimize injury. NASA similarly monitors astronaut health with unprecedented detail, recognizing that spaceflight accelerates aging through oxidative stress, mitochondrial dysfunction, and immune dysregulation—precisely the mechanisms implicated in ME/CFS.
For aging executives, competitive masters athletes, and parents of elite student-athletes seeking admission to universities like Stanford, MIT, or Yale, the lessons are clear: mitochondrial health is performance health. VO2 max—the maximum rate of oxygen consumption during exercise, which depends entirely on mitochondrial respiratory capacity—is the single most powerful predictor of longevity and healthspan. Every 1-MET (metabolic equivalent) increase in VO2 max (approximately 3.5 mL/kg/min of oxygen consumption) reduces all-cause mortality risk by 13-15%.
The training principles for optimizing mitochondrial function mirror those being discovered in ME/CFS research. Zone 2 training—sustained aerobic exercise at 60-70% maximum heart rate where lactate production equals lactate clearance—stimulates mitochondrial biogenesis through PGC-1α activation. But critically, this adaptation requires adequate recovery and nutritional support (sufficient protein, antioxidants, NAD+ precursors) to build new mitochondria. ME/CFS patients who cannot tolerate even Zone 2 exercise remind us that energy systems can be pushed past the point of adaptation into dysfunction.
High-intensity interval training (HIIT) provides complementary benefits by challenging mitochondria to handle oxidative stress and rapid ATP demand changes. However, the same research showing WASF3 disruption under ER stress suggests that excessive high-intensity training—particularly without adequate recovery—could trigger similar pathological cascades in healthy individuals. The emerging field of overtraining syndrome (OTS) shares striking similarities with ME/CFS: severe fatigue, hormonal disruption, immune dysfunction, and prolonged recovery requirements. Both likely involve mitochondrial exhaustion and ER stress.
This is where personalized medicine via digital twins becomes transformative. Organizations providing longevity-related services—from Fountain Life’s comprehensive diagnostics to LongevityPlan.AI’s integrated coaching platforms—enable individuals to walk the knife-edge between optimal training stimulus and pathological overload. Real-time biomarker feedback (lactate, cortisol, inflammatory markers, mitochondrial function tests) combined with continuous wearable monitoring allows precise titration of training stress to match individual recovery capacity.
Companies like TwinHealth, Reya.ai, and Longevity AI are pioneering this integrated approach, using AI agents to continuously assess health status and provide real-time, data-driven care. TwinHealth, for example, creates comprehensive metabolic profiles and adjusts recommendations daily based on glucose monitors, activity trackers, and biomarker trends. For the affluent health-conscious individual—the CEO funding corporate wellness programs, the aging model maintaining peak physicality, the venture capitalist seeking cognitive edge—these platforms offer unprecedented optimization potential.
The implications for youth sports and academic achievement are equally profound. Organizations like IMG Academy, Academic Architect, and Crimson Education provide comprehensive athletic and academic coaching for students seeking admission to elite universities. However, the “training intensity” arms race in youth sports—with specialization, year-round competition, and private coaching beginning as early as age 6-8—creates concerning parallels to overtraining syndrome in adults. Recent research by Dr. Kirsten Hextrum at Oregon State University documents how family affluence drives sport specialization, which in turn predicts higher training volumes and injury rates.
A 2024 study published in PLoS ONE found that families with higher socioeconomic status were more likely to have children in competitive travel sports programs, with median annual costs exceeding $2,500 per sport. These families also reported higher training intensity and earlier sport specialization. While athletic achievement can facilitate college admission, the metabolic cost—potential mitochondrial dysfunction, ER stress, and long-term health consequences—remains poorly studied in pediatric populations. Digital twin technology could provide crucial safeguards, monitoring young athletes for early signs of overtraining and energy system dysfunction before irreversible damage occurs.
The Future of Fatigue: Precision Medicine, AI Integration, and Cellular Rejuvenation
The scientific revolution in chronic fatigue research from 2023-2025 has fundamentally transformed our understanding of this debilitating condition. What was once dismissed as psychosomatic or untreatable is now recognized as a complex but tractable biochemical disorder involving WASF3-mediated mitochondrial dysfunction, ER stress, NAD+ deficiency, oxidative damage, immune dysregulation, and kynurenine pathway alterations. Each of these mechanisms provides potential therapeutic targets, and their elucidation offers hope to the 80 million people worldwide suffering from ME/CFS.
Perhaps most importantly, the molecular characterization of chronic fatigue enables precision medicine approaches powered by artificial intelligence. Digital twins—virtual replicas continuously updated with real-world data—can predict energy system failures before they occur, optimize interventions for individual biochemistries, and track treatment responses with unprecedented granularity. The Cardiorespiratory Digital Twin™ represents a paradigm shift from reactive medicine (treating crashes after they happen) to predictive medicine (preventing crashes before they occur).
The convergence of several technological and scientific trends positions 2025-2030 as a potentially transformative period for fatigue medicine. First, wearable technology continues to improve, with next-generation devices measuring previously inaccessible parameters: continuous lactate monitoring, non-invasive NAD+ sensing, real-time mitochondrial function assessment. Second, AI algorithms are becoming increasingly sophisticated at pattern recognition, with deep learning models identifying subtle biomarker combinations that predict disease course months in advance. Third, omics technologies (genomics, transcriptomics, proteomics, metabolomics) are becoming faster and cheaper, enabling comprehensive molecular profiling at costs accessible beyond research settings.
Fourth, pharmaceutical development is accelerating. Dr. Hwang’s team at the NIH is actively pursuing clinical trials of ER stress modulators and WASF3 inhibitors. Biotech companies like Insilico Medicine and Deep Longevity are using AI to design novel compounds targeting age-related mitochondrial dysfunction—compounds that could benefit both ME/CFS patients and healthy individuals seeking to extend their healthspan. The first drug designed entirely by artificial intelligence (INS018_055, a fibrosis treatment) entered human trials in 2023, demonstrating the potential of this approach.
The democratization of elite health optimization represents another crucial trend. Platforms like LongevityPlan.AI, Function Health, and Viome are making professional-grade health monitoring and personalized recommendations accessible to broader populations. What was once available only to Olympic athletes and billionaire biohackers—comprehensive biomarker panels, AI-powered coaching, real-time metabolic feedback—is becoming available to anyone willing to invest in their health. This democratization aligns with the scientific principle underlying personalized medicine: everyone is biochemically unique, and optimization strategies must be individualized.
For the target audience—aging athletes, longevity-focused executives, competitive professionals, parents of elite student-athletes—the message is clear: your mitochondria matter. The same cellular powerhouses that enable an Ironman finish or a 16-hour workday can, if overtaxed or insufficiently supported, slide into the dysfunctional state characteristic of ME/CFS. The difference between peak performance and debilitating fatigue often lies not in motivation or willpower but in the molecular health of your mitochondrial fleet.
Strategic planning for longevity therefore must incorporate mitochondrial optimization as a cornerstone. This means: (1) Regular monitoring of mitochondrial function markers (VO2 max testing, lactate threshold assessment, comprehensive metabolomics including NAD+ levels and kynurenine pathway metabolites), (2) Balancing training stress with adequate recovery (perhaps the most important lesson from ME/CFS research), (3) Nutritional support for cellular energetics (sufficient protein, antioxidants, NAD+ precursors, B-vitamins, magnesium, CoQ10), (4) Managing inflammation and oxidative stress (through diet, sleep optimization, stress management), and (5) Leveraging AI-powered digital twins for real-time optimization and early warning of energy system dysfunction.
The vision is ambitious but achievable: a future where chronic fatigue is diagnosed objectively through molecular profiling, treated effectively with targeted interventions, and prevented proactively through digital twin monitoring. A future where athletes extend their competitive careers by precisely managing their energy systems. A future where executives maintain cognitive performance into their 70s and 80s because their mitochondria remain robust. A future where "long COVID" patients recover fully because we understand and can reverse the WASF3-ER stress-mitochondrial dysfunction cascade.
This future is being built today in laboratories at the NIH, Stanford, Harvard, Macquarie University, and Weizmann Institute. It is being commercialized by companies like Fountain Life, Viome, TruDiagnostic, and LongevityPlan.AI. It is being adopted by elite organizations from the NBA to NASA. And it offers hope—grounded in rigorous science rather than wishful thinking—that the molecular mysteries of fatigue can be solved, that cellular energetics can be optimized, and that human performance and longevity can be extended far beyond current limitations.
The journey from chronic exhaustion to sustained vitality is being mapped at the molecular level. The tools to navigate this journey—comprehensive diagnostics, AI-powered analytics, personalized interventions—are rapidly becoming available. The question is not whether chronic fatigue can be understood and managed, but whether individuals and organizations will embrace the data-driven, precision medicine approaches that make it possible. For those who do, the rewards are profound: extended healthspan, optimized performance, and freedom from the devastating burden of cellular energy failure.
References
-
Wang PY, Ma J, Kim YC, et al. WASF3 disrupts mitochondrial respiration and may mediate exercise intolerance in myalgic encephalomyelitis/chronic fatigue syndrome. Proc Natl Acad Sci U S A. 2023;120(34):e2302738120. doi:10.1073/pnas.2302738120
-
Unger ER, Lin JS, Brimmer DJ, Tian H, Blanton R, Smail MJ. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: United States, 2021–2022. NCHS Data Brief No. 488. National Center for Health Statistics. December 2023.
-
Lim EJ, Ahn YC, Jang ES, Lee SW, Lee SH, Son CG. Systematic review and meta-analysis of the prevalence of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J Transl Med. 2020;18:100. doi:10.1186/s12967-020-02269-0
-
Institute of Medicine. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. Washington, DC: The National Academies Press; 2015. doi:10.17226/19012
-
Boyce M, Bryant KF, Jousse C, et al. A selective inhibitor of eIF2α dephosphorylation protects cells from ER stress. Science. 2005;307(5711):935-939. doi:10.1126/science.1101902
-
Valdez AR, Hancock EE, Adebayo S, et al. Estimating Prevalence, Demographics, and Costs of ME/CFS Using Large Scale Medical Claims Data and Machine Learning. Front Pediatr. 2019;6:412. doi:10.3389/fped.2018.00412
-
Missailidis D, Annesley SJ, Fisher PR. Pathological Mechanisms Underlying Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Diagnostics (Basel). 2019;9(3):80. doi:10.3390/diagnostics9030080
-
Tomas C, Newton J. Metabolic abnormalities in chronic fatigue syndrome/myalgic encephalomyelitis: a mini-review. Biochem Soc Trans. 2018;46(3):547-553. doi:10.1042/BST20170503
-
Naviaux RK, Naviaux JC, Li K, et al. Metabolic features of chronic fatigue syndrome. Proc Natl Acad Sci U S A. 2016;113(37):E5472-E5480. doi:10.1073/pnas.1607571113
-
Germain A, Ruppert D, Levine SM, Hanson MR. Metabolic profiling of a myalgic encephalomyelitis/chronic fatigue syndrome discovery cohort reveals disturbances in fatty acid and lipid metabolism. Mol Biosyst. 2017;13(2):441-455. doi:10.1039/c6mb00600k
-
Komaroff AL, Lipkin WI. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol Med. 2021;27(9):895-906. doi:10.1016/j.molmed.2021.06.002
-
Armstrong CW, McGregor NR, Lewis DP, Butt HL, Gooley PR. Metabolic profiling reveals anomalous energy metabolism and oxidative stress pathways in chronic fatigue syndrome patients. Metabolomics. 2015;11:1626-1639. doi:10.1007/s11306-015-0816-5
-
Morris G, Maes M. Oxidative and Nitrosative Stress and Immune-Inflammatory Pathways in Patients with Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Curr Neuropharmacol. 2014;12(2):168-185. doi:10.2174/1570159X11666131120224653
-
Fluge Ø, Mella O, Bruland O, et al. Metabolic profiling indicates impaired pyruvate dehydrogenase function in myalgic encephalopathy/chronic fatigue syndrome. JCI Insight. 2016;1(21):e89376. doi:10.1172/jci.insight.89376
-
Grieves M, Vickers J. Digital Twin: Mitigating Unpredictable, Undesirable Emergent Behavior in Complex Systems. In: Kahlen FJ, Flumerfelt S, Alves A, eds. Transdisciplinary Perspectives on Complex Systems. Springer; 2017:85-113. doi:10.1007/978-3-319-38756-7_4
-
Hornig M, Montoya JG, Klimas NG, et al. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. Sci Adv. 2015;1(1):e1400121. doi:10.1126/sciadv.1400121
-
Mandarano AH, Maya J, Giloteaux L, et al. Myalgic encephalomyelitis/chronic fatigue syndrome patients exhibit altered T cell metabolism and cytokine associations. J Clin Invest. 2020;130(3):1491-1505. doi:10.1172/JCI132185
-
Montoya JG, Holmes TH, Anderson JN, et al. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proc Natl Acad Sci U S A. 2017;114(34):E7150-E7158. doi:10.1073/pnas.1710519114
About the Authors
Tony Medrano is CEO and co-founder of LongevityPlan.AI, a platform that integrates performance and health data from athletes and leverages proprietary digital twin technology, wearable data, and biomarker data to deliver personalized performance optimization and longevity recommendations to athletes, coaches, organizations, businesses, government, and the military. In addition to being a 3x technology / AI company CEO with 2 successful exits, Tony has also finished 3 Full Ironman Triathlons (140.6 mi) since 2019. He has degrees from Harvard University, Columbia University, and a JD/MBA from Stanford University. Tony has been involved with AI and molecular diagnostic start-ups for 10 years, and also worked with the US Olympic Team, National Basketball Association (NBA), National Football League (NFL), Major League Baseball (MLB), Iditarod, FBI, NASA, U.S. Department of Health and Human Services (HHS), Google, Microsoft, Netflix, Bridgewater Associates, ConocoPhillips, British Petroleum, Jenny Craig, Inc. and Chevron to provide technology, artificial intelligence and/or molecular diagnostics solutions to their employees.
Sydney Wiredu is a Research Intern at LongevityPlan.AI and a researcher and entrepreneur passionate about using science and technology to extend human healthspan. A Ghanaian-American student at Harvard University, he studies Chemistry and Neuroscience with a secondary focus in Global Health and Health Policy. His work lies at the intersection of biotechnology, health systems innovation, and rare disease research, united by a mission to make longevity accessible to all. At Harvard Medical School and Massachusetts General Hospital, Sydney investigates mitochondrial dysfunction and neurodegenerative mechanisms in X-linked dystonia parkinsonism at the Bragg Lab. Sydney also co-first authored a publication in Therapeutic Advances in Rare Disease analyzing how integrated care models can improve outcomes for rare disease patients. Beyond the lab, Sydney leads initiatives that bridge scientific research and social impact. As President of the Harvard Undergraduate Biotechnology Club, he built partnerships with some of the globe’s largest biotechnology companies, generating record fundraising and establishing international programs in rare disease innovation. He also served as Director of Strategy for the Harvard Undergraduate Tech and Global Health Initiative. Sydney is also the Co-Founder and CEO of Circlez, a Harvard Innovation Labs-incubated startup developing goal-setting software that blends behavioral science with AI. Under his leadership, Circlez has raised over $50,000 in non-dilutive funding, been accepted to the NSF Innovation Corps, and recognized among the top 5% of Y Combinator applicants. His achievements have earned him honors such as the Boston Inno and Philly Inno’s 25 Under 25 lists. Sydney was also selected to represent the state of New Jersey at Boys Nation, and he was admitted to seven Ivy League universities. He plans to attend medical school upon graduating. Driven by a belief that breakthroughs in longevity should benefit everyone, Sydney brings to LongevityPlan.AI a perspective that combines molecular neuroscience, entrepreneurial innovation, and public health ethics. Outside of research, he enjoys playing piano, tennis, and calisthenics.