Military & Veterans
·15 min read
From Battlefield to Bedside
How the US Army's Digital Twin Revolution Is Rewriting the Future of Veteran Health and Human Performance
By Tony Medrano, CEO & Co-Founder, LongevityPlan.AI

The soldier crouches behind a low wall during a 72-hour field exercise at Fort Devens, Massachusetts, sweat dripping down her face as she prepares for a live-fire drill. Unbeknownst to her, seventeen different sensors are silently monitoring her heart rate variability, skin temperature, hydration status, sleep quality from the previous nights, and cognitive alertness scores. Somewhere in a command center, algorithms are calculating whether her squad is ready for the next mission—or whether they need another four hours of recovery before they can perform at peak capacity.
This is not science fiction. This is the MASTR-E program, and it represents one of the most ambitious human performance optimization initiatives ever undertaken by the United States military. More importantly, it offers a blueprint for how personalized medicine, powered by digital twin technology and artificial intelligence, could transform healthcare for the 19 million veterans currently served by the Department of Veterans Affairs—and ultimately, for anyone seeking to extend their healthspan and optimize their performance across the lifespan.
The question is no longer whether we can create virtual replicas of the human body that predict, optimize, and personalize health outcomes. The question is whether we're ready to scale this technology from elite military applications to the broader population. And the answer, based on recent developments at the intersection of defense technology, AI research, and digital health, is a resounding yes.
The Humanoid Digital Twin: More Than a Virtual Mannequin
When most people hear "digital twin," they think of industrial applications—virtual replicas of jet engines, manufacturing plants, or smart cities. But the concept's origins lie in a far more dramatic setting: the Apollo 13 mission, when NASA engineers frantically created simulations aboard a grounded spacecraft to bring three astronauts safely home from space.¹
Today's humanoid digital twins have evolved far beyond that emergency improvisation. As defined in a landmark 2024 scoping review published in NPJ Digital Medicine, a digital twin for healthcare represents "a virtual representation of a person which allows dynamic simulation of potential treatment strategy, monitoring and prediction of health trajectory, and early intervention and prevention, based on multi-scale modeling of multi-modal data."²
The critical distinction between a digital twin and a simple computer model lies in three essential components: a physical entity (the human), a virtual replica (the computational model), and a bidirectional real-time connection between the two. As the review's authors—led by Dr. Evangelia Katsoulakis of the VA Informatics and Computing Infrastructure and Dr. Jun Deng of Yale University—emphasize, a true digital twin must be "individualized, interconnected, interactive, informative, and impactful."³
This 5-Is framework matters because it separates genuine digital twin technology from the marketing hype that surrounds much of what passes for "AI health" today. Your fitness tracker may collect data, but unless it creates a personalized model that adapts in real time, predicts your future health trajectory, and enables genuine interventions, it's not a digital twin—it's just another wearable.
The military understood this distinction early. And they've spent $100 million proving it works.
MASTR-E: The Largest Human Performance Science Program in Military History
In 2018, the U.S. Army Combat Capabilities Development Command (DEVCOM) Soldier Center launched Measuring and Advancing Soldier Tactical Readiness and Effectiveness—MASTR-E—as part of the Department of Defense Close Combat Lethality Task Force. The goal was audacious: create quantifiable metrics for human performance that could predict how well soldiers and small units would perform under stress, then use that data to optimize training, recovery, and mission planning.⁴
"We want to know what are these critical 'X factors' that can predict the ability to sustain performance under tough conditions," explained George Matook, the MASTR-E Program Manager, in an interview with Army Times. The program's approach mirrors what elite sports organizations have been doing for decades—but with higher stakes and more rigorous methodology.⁵
The MASTR-E framework analyzes four domains of performance predictors—health, physical, social-emotional, and cognitive—against five outcome categories: shoot, move, sustain, navigate, and communicate. Within each domain lies a constellation of measured factors: immune system status, gut microbiome composition, nutrition and metabolism, sleep quality, stress reactivity, emotional regulation, and cognitive speed under fatigue.⁶
During a foundational 2020 study, researchers monitored 530 soldiers from the 4th Battalion, 31st Infantry Regiment, 2nd Brigade Combat Team, 10th Mountain Division throughout a full field exercise. Participants wore smart rings for sleep monitoring, chest straps for cardiac data, and wrist devices for activity tracking. Training cadre used tablet computers to monitor soldiers and small units in real time, watching for degradation patterns that might predict injury or performance failure.⁷
The results were striking. As Col. Paul O. Kwon, DO, MPH, and his colleagues noted in a May 2025 article published in the U.S. Army's Special Warfare Journal, MASTR-E demonstrated that "utilizing advances in AI and computer vision, we've been able to track and study personalized analytics from a variety of tasks to determine the strengths and deficiencies in performance and help make data-informed training and competition plans."⁸
Perhaps more importantly, MASTR-E generated the largest dataset of soldier physiological and cognitive performance data ever collected under operationally relevant conditions. This data didn't just stay in military research labs—it became the foundation for a new approach to performance optimization that could extend far beyond the battlefield.
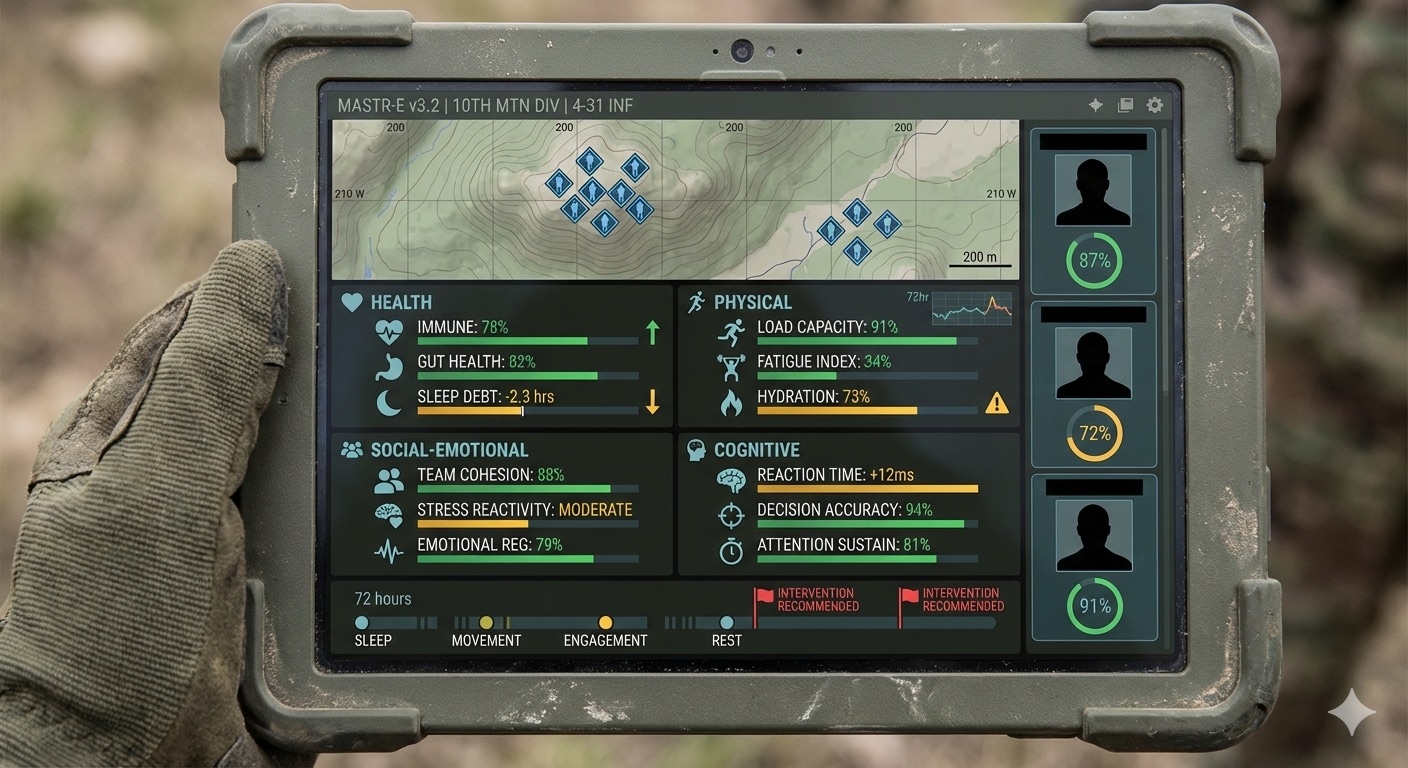
The MASTR-E commander's dashboard tracks soldier readiness across four domains—health, physical, social-emotional, and cognitive—enabling real-time intervention decisions during field exercises. This $100 million program generated the largest dataset of soldier physiological performance ever collected under operational conditions.
From Soldier to Patient: The Casualty Digital Twin Paradigm
While MASTR-E focused on healthy soldier optimization, a parallel effort was developing digital twin technology for the opposite scenario: what happens when a soldier is wounded and enters the military healthcare system?
In a groundbreaking commentary published in Military Medicine in January 2025, Dr. Jeremy C. Pamplin of the Telemedicine and Advanced Technology Research Center and his colleagues introduced the concept of Casualty Digital Twins (CDTs)—virtual representations of wounded service members that predict their probable treatment needs and match those needs to available resources across the care continuum.⁹
"A casualty digital twin is a model of a casualty and the care system that can be used to predict a real casualty's probable treatment needs—like blood, surgery, medications, and evacuation—and to match those needs to their availability within the continuum of care," Dr. Pamplin explained. "It is informed by critical inputs such as environmental context, injury and illness patterns, caregiver actions, resource availability, mission requirements, and more."¹⁰
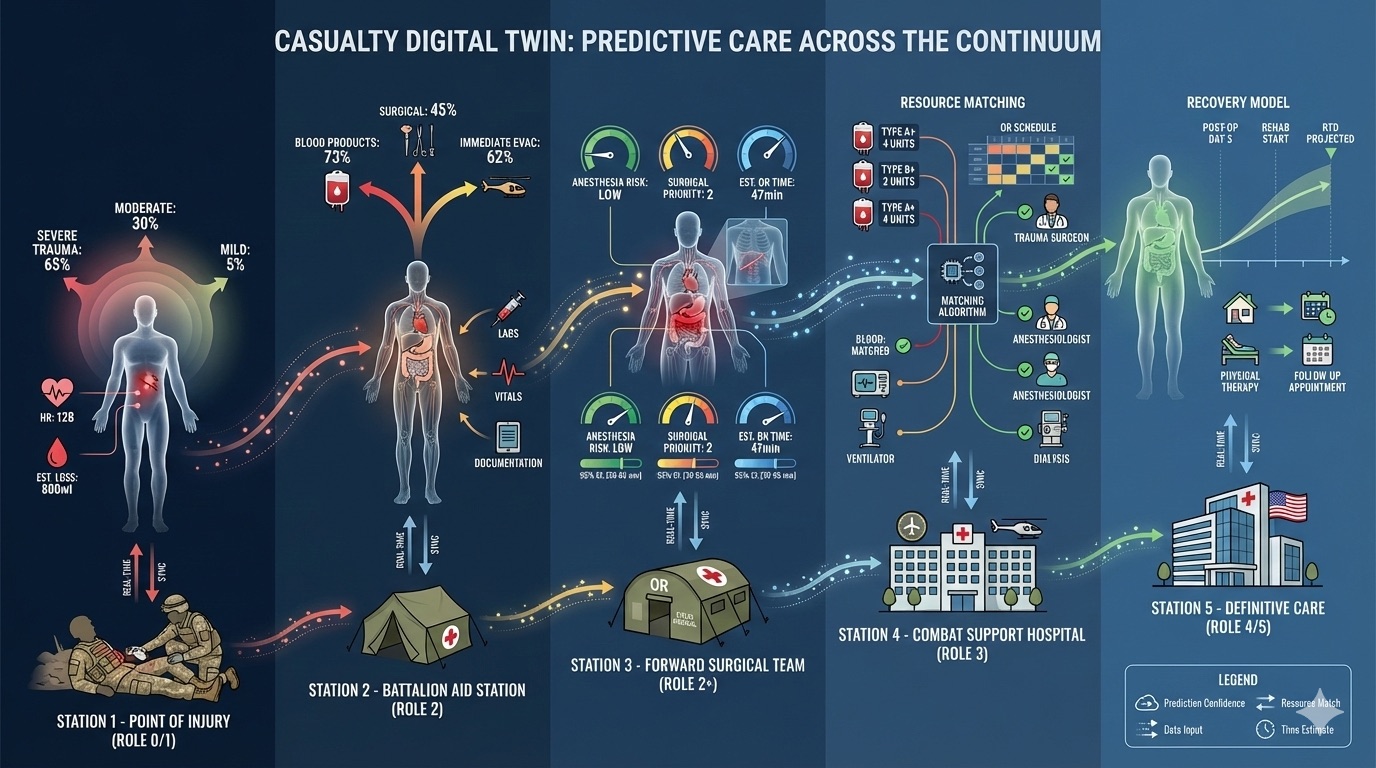
The Casualty Digital Twin paradigm predicts wounded service members' treatment needs—blood products, surgical intervention, medication requirements, evacuation timing—at each stage of the combat care continuum, enabling resource matching before patients arrive at treatment facilities.
The implications are profound. Consider a medic managing multiple casualties after an explosion. Currently, triage decisions depend on training, experience, and often incomplete information about each patient's condition and likely trajectory. With CDTs, the medic's computing system would know what treatments and resources each casualty will likely need and when—enabling data-driven decisions about who receives limited blood supplies, who should be evacuated first, and who might be designated expectant because their surgical needs cannot be met.
Dr. Pamplin drew an illuminating parallel to the autonomous vehicle industry, which has spent decades collecting massive datasets from millions of driven miles to train AI systems that can navigate complex traffic environments without human intervention. Waymo, he noted, mapped over one million miles of roads between 2009 and 2012, collecting 3 gigabytes of data every minute—roughly 7.2 petabytes total—before earning the license to operate driverless taxis in San Francisco in 2023.¹¹
"Unfortunately, obtaining and processing this amount of data is presently untenable in military medicine or combat casualty care," Dr. Pamplin acknowledged. "We lack the intention, and thus the infrastructure, in terms of sensors for data collection, the network approvals for software that can transfer these data, a storage solution for this amount of data, and processes to annotate, curate, analyze, model, and share these with partners who can produce viable solutions from it."¹²
But the groundwork is being laid. And the technology being developed for combat casualty care has direct applications to the nine million veterans who receive care through the VA healthcare system—the largest integrated healthcare network in the United States.
The VA's AI Revolution: Ambient Scribes and Beyond
If you've visited a VA medical center recently, you may have noticed something different: your doctor is actually looking at you instead of typing furiously into a computer. That change reflects one of the most significant AI deployments in federal healthcare history.
In October 2025, the Department of Veterans Affairs launched its ambient AI scribe technology across pilot sites in Dallas, East Orange, Miami, San Francisco, and six other VA Medical Centers. The system works by recording appointment audio with the veteran's consent, then using AI to transcribe the conversation and extract relevant medical information for the patient's chart. What previously required providers to spend 15 to 30 minutes typing notes after each visit now happens automatically in the background.¹³
"Veterans said they felt more connected to their provider because they were having a real conversation, not talking to someone typing on a computer," reported Donna Hill, Director of Operations for AI and Emerging Technologies at the VA's Digital Health Office. "My provider would look me in the eye and have an actual conversation," one veteran told the VA during the pilot evaluation.¹⁴
The numbers are impressive: the VA piloted ambient AI scribe technology with more than 800,000 veterans over six months, and 71% of the 75 veterans surveyed reported no concerns about using the technology. Early metrics suggest a 40% reduction in after-hours charting for participating providers—time that can now be devoted to direct patient care or, critically, to the provider's own recovery and wellbeing.¹⁵
The VA deployed two commercial AI scribe platforms—Abridge and Knowtex AI—after a competitive tech sprint at the VA Innovation Center in Orlando. The contracts, announced by Assistant Under Secretary for Health Carolyn Clancy, MD, represent the VA's largest generative AI deployment to date.¹⁶
VA providers using ambient AI scribes from Abridge and Knowtex report a 40% reduction in after-hours documentation time. "My provider would look me in the eye and have an actual conversation," one veteran observed. Over 800,000 veterans have experienced AI-enhanced visits across 10 VA Medical Centers.
But ambient scribes are just the beginning. The VA's September 2025 AI Strategy document outlined a far more ambitious vision: deploying AI across healthcare diagnostics with computer vision, streamlining benefits claims with generative AI, and creating what the document calls "an industry leader in its use of effective, reliable, and safe AI tools" that will "deliver measurable improvements in speed, quality, efficiency and accuracy, fundamentally transforming the delivery of healthcare and benefits for Veterans."¹⁷
This vision aligns precisely with the digital twin paradigm emerging from military research. The VA already maintains the Million Veteran Program—one of the largest genomic databases in the world—along with decades of longitudinal health records, imaging data, and outcome information that could power sophisticated personalized medicine models.¹⁸
The question now is whether the VA can bridge the gap between AI documentation tools and true digital twin technology that predicts individual health trajectories and optimizes interventions in real time. The answer may come from an unlikely source: the defense contractors and AI companies that have been building digital twin infrastructure for the Pentagon.
The Defense-Tech Pipeline: From Palantir to Patient Care
When Palantir Technologies delivered its first two Tactical Intelligence Targeting Access Node (TITAN) systems to the U.S. Army in March 2025, the $178 million contract represented more than a military procurement milestone. It demonstrated that software companies could successfully serve as primary contractors for sophisticated hardware-software integration programs that previously belonged exclusively to legacy defense giants.¹⁹
TITAN operates as a mobile ground station that harnesses AI to collect data from space sensors, assisting soldiers with warfare strategy and improving strike targeting accuracy. But the underlying technology—what Palantir calls its "Ontology"—creates what is essentially a digital twin of an organization, allowing AI to understand relationships, dependencies, and potential outcomes across complex systems.²⁰
"No single company is capable of delivering on the promise of AI for national security," Palantir and Anduril Industries stated in a December 2024 joint announcement of their partnership to build military AI infrastructure. "Exabytes of defense data, indispensable for AI training and inferencing, are currently evaporating."²¹
That last sentence should resonate with anyone concerned about healthcare. The same problem—valuable data being generated but not captured, processed, or utilized for AI training—exists throughout civilian medicine. Every clinical encounter generates potential training data for personalized medicine models, but without the infrastructure to capture and process it, that data evaporates as surely as battlefield sensor feeds.
The Palantir-Anduril partnership aims to solve this problem for defense applications by deploying Anduril's Lattice software and Menace edge computing systems to collect data from sensors, vehicles, and weapons in the field, then flowing that information into Palantir's AI Platform for processing and model development. The same architecture could, in principle, collect clinical data from wearables, medical devices, and electronic health records, then process it into personalized health models.²²
This isn't speculation. Palantir's Foundry platform already powers healthcare operations at major hospital systems, and the company's partnership with Amazon Web Services gives it cloud infrastructure capable of handling the scale required for population-level health modeling. Meanwhile, NVIDIA—whose GPUs power both military AI systems and healthcare computing clusters—has invested heavily in healthcare applications, including partnerships with major academic medical centers for AI-driven drug discovery and clinical decision support.²³
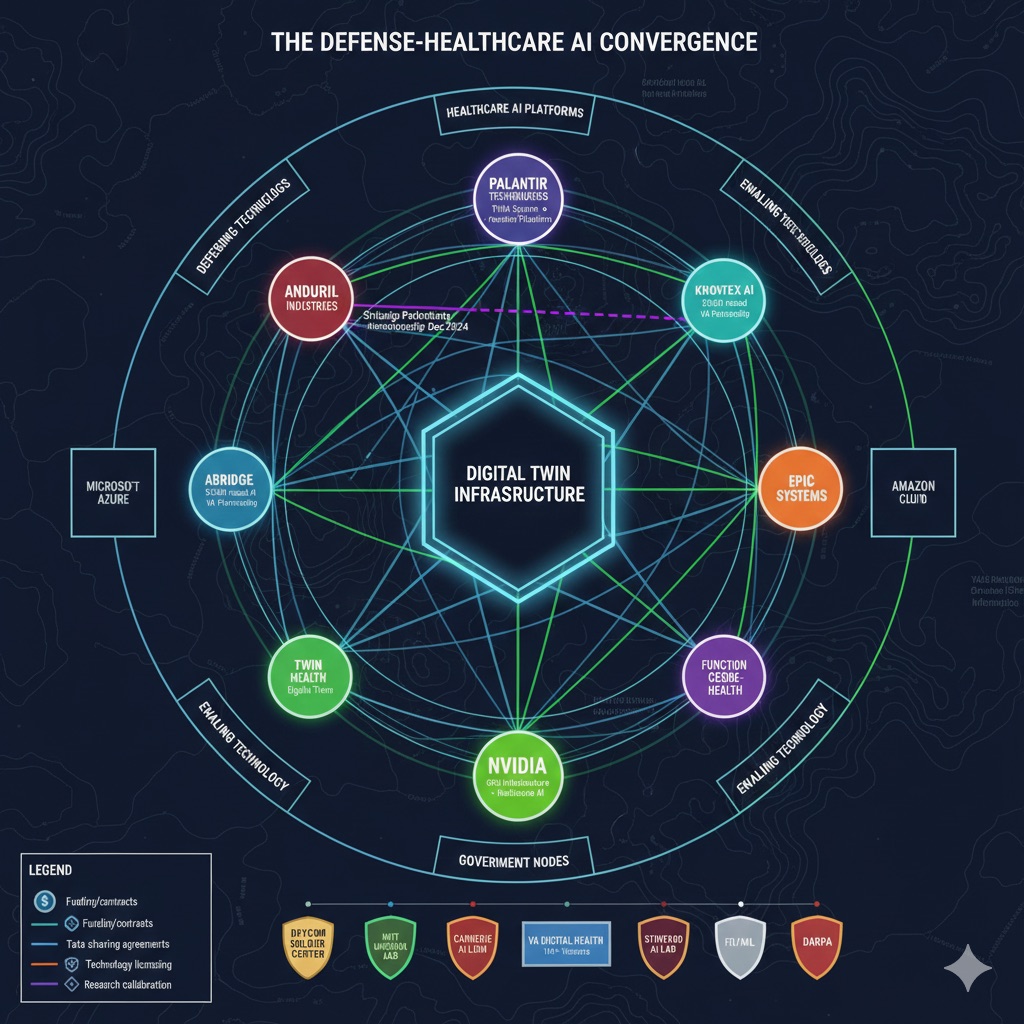
The defense-healthcare technology ecosystem converges around digital twin infrastructure: the same companies building AI for battlefield situational awareness—Palantir, Anduril, NVIDIA—are now deploying their capabilities to transform veteran care and civilian medicine.
The convergence of defense AI capabilities and healthcare needs creates an unprecedented opportunity for what Harvard Law School's I. Glenn Cohen calls "AI that handles anything with medium to high risk." Speaking to the Harvard Gazette about AI healthcare regulation in January 2026, Cohen noted that "the vast majority of medical AI is never reviewed by a federal regulator—and probably no state regulator. We want to have standards for healthcare AI and an incentive to adopt standards."²⁴
The military's rigorous verification, validation, and accreditation processes for AI systems—developed for applications where failure means lives lost—could provide a model for civilian healthcare AI governance. As Cohen observed, "If they perform badly, many of these technologies are a much greater risk to the general populace than the average device on the market."²⁵
The Cardiorespiratory Digital Twin™: Bridging Military Research and Longevity Science
The military's focus on cardiorespiratory fitness isn't coincidental. VO2 max—the maximum rate at which the body can utilize oxygen during intense exercise—has emerged as arguably the most powerful single predictor of all-cause mortality across dozens of longitudinal studies. A 2018 study published in JAMA Network Open found that cardiorespiratory fitness was inversely associated with long-term mortality regardless of age, sex, or baseline health status.²⁶
This is where military human performance research directly intersects with longevity science. The MASTR-E program's focus on sustain, navigate, and communicate outcomes all depend fundamentally on cardiorespiratory capacity—the soldier's ability to deliver oxygen to working muscles and maintain cognitive function under physical stress.
A Cardiorespiratory Digital Twin™ takes this concept further by creating a personalized model of an individual's oxygen delivery system—heart, lungs, blood vessels, mitochondria, and the control systems that coordinate them—that can predict responses to different training stimuli, recovery patterns, and long-term capacity changes.
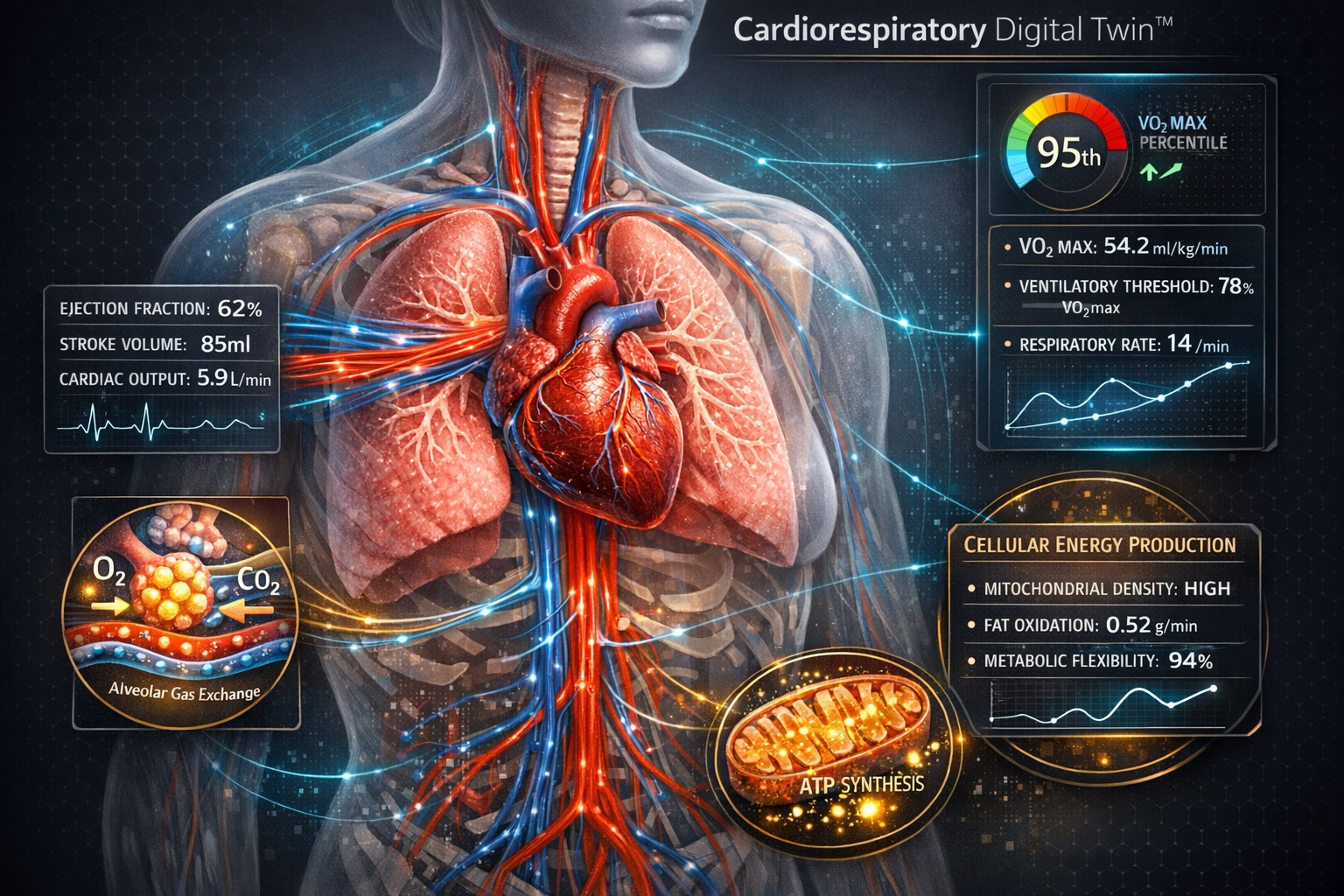
The Cardiorespiratory Digital Twin™ integrates heart function, pulmonary gas exchange, vascular dynamics, and mitochondrial metabolism into a unified predictive model. Research shows VO2 max is the strongest modifiable predictor of all-cause mortality—making cardiorespiratory optimization the foundation of evidence-based longevity planning.
Dr. Iñigo San Millán, the exercise physiologist who coaches Tour de France champion Tadej Pogačar, has emphasized that understanding an athlete's individual metabolic profile is essential for optimizing training. "Zone 2 training is about training your mitochondria," San Millán explained in a widely-cited interview. "It's the only way to really improve your fat oxidation and your mitochondrial function."²⁷
The military's approach applies similar principles at scale. During MASTR-E studies, researchers measured not just external performance metrics but internal physiological responses—how individual soldiers' metabolic systems handled sustained exertion, how quickly they recovered, and what factors predicted performance degradation under stress.
For veterans transitioning to civilian life, this research has direct implications. Many veterans develop cardiovascular disease, metabolic syndrome, and other chronic conditions at higher rates than the general population—conditions that reflect the long-term consequences of operational stress, sleep disruption, and the physiological demands of military service.²⁸
A Cardiorespiratory Digital Twin™ could enable personalized prevention strategies that account for each veteran's unique physiological history, current capacity, and risk factors. Rather than generic recommendations to "exercise more," the model could specify optimal training intensities, predict recovery needs, and identify early warning signs of declining capacity—the same approach that helps elite soldiers maintain readiness applied to helping veterans maintain health.
Dassault, Siemens, and the Living Heart: Industry Leaders Building the Infrastructure
The digital twin revolution in healthcare isn't being built by startups alone. Major industrial technology companies—the same ones that create digital twins for jet engines and manufacturing plants—have turned their attention to biological systems.
Dassault Systèmes' SIMULIA Living Heart Project, launched in 2014 in collaboration with the FDA, represents one of the most sophisticated organ-level digital twins ever created. The validated model simulates the structure and physiological function of the human heart, enabling researchers to test cardiac devices, study drug interactions, and plan interventions without risking patient safety.²⁹
Siemens Healthineers has partnered with academic medical centers, including the Medical University of South Carolina, to develop digital twin applications for hospital operations, clinical workflow optimization, and personalized treatment planning. Their cardiac digital twin technology enables simulation of cardiac resynchronization therapy—identifying optimal device settings before surgery rather than through trial and error afterward.³⁰
Swedish medical simulation pioneer Mentice AB (STO: MNTC) represents another critical node in this ecosystem, having spent over two decades building what amounts to procedural digital twins for endovascular interventions. Founded in 1999, Mentice has established approximately 50 medical simulation patents and deployed over 2,000 systems worldwide covering cardiovascular, neurovascular, and peripheral interventions. Their VIST® Virtual Patient platform—integrated directly into Siemens Healthineers' Artis icono angiography systems—enables clinicians to perform simulated cardiac and vascular procedures using actual C-arm controls, table manipulation, and foot pedals while deploying real medical devices in a radiation-free environment. "The VIST® Virtual Patient provides an immersive, high-fidelity, simulation-based environment accessible right from the Artis icono system making this integration one of the most sophisticated options in the field of endovascular skills acquisition," explained Göran Malmberg, Mentice CEO.
Critically, Mentice's platform allows clinicians to import actual MR and CT patient data for case training and rehearsal—creating patient-specific anatomical twins that physicians can practice on before touching a real patient. This capability proved instrumental when EBR Systems used Mentice technology to conduct FDA approval studies for the WiSE® wireless pacing system, demonstrating that high-fidelity simulation can accelerate device validation while enhancing patient safety. As medical device complexity increases and procedural learning curves steepen, platforms like Mentice's represent the training infrastructure that will enable widespread adoption of digital twin-guided interventions—bridging the gap between sophisticated AI prediction and the human hands that must ultimately execute care.

Mentice's VIST® Virtual Patient, integrated with Siemens Healthineers' Artis icono angio-suite, enables clinicians to practice complex endovascular procedures on patient-specific digital anatomies—imported directly from CT and MRI data—in a radiation-free environment before treating actual patients.
GE Healthcare's Care Command platform, deployed across multiple hospital systems, creates digital twins of hospital operations—tracking bed availability, staffing levels, equipment status, and patient flow in real time. During the COVID-19 pandemic, Oregon deployed Care Command technology statewide to track ventilator capacity across all hospitals, demonstrating how digital twin infrastructure can enable population-level resource optimization.³¹
These industrial digital twin capabilities are increasingly converging with AI platforms from companies like C3.ai, which specializes in enterprise AI applications, and emerging defense-focused firms like Shield AI and Scale AI. The result is an ecosystem capable of supporting digital twins across multiple scales—from molecular interactions to organ systems to hospital operations to population health.
For longevity-focused individuals and organizations, this infrastructure represents unprecedented opportunity. The same technology that tracks fighter jet maintenance schedules could track biomarker trends. The same AI that optimizes manufacturing processes could optimize training protocols. The same platforms that model combat scenarios could model health interventions.
The Johns Hopkins Applied Physics Laboratory and Military-Academic Collaboration
The military's digital twin research doesn't happen in isolation. Academic partnerships—particularly with institutions that bridge basic research and applied defense technology—play a crucial role in developing the scientific foundations that make digital twins possible.
The Johns Hopkins Applied Physics Laboratory (APL), one of the nation's largest university-affiliated research centers, has been instrumental in developing sensing technologies, data fusion algorithms, and computational models for military applications. APL's work spans from underwater acoustic sensing to space systems to human performance monitoring—the full spectrum of technologies required for comprehensive digital twin implementations.³²
MIT Lincoln Laboratory, another federally funded research center, has contributed to the development of AI systems for defense applications, including the kind of computer vision and natural language processing that enables ambient AI scribes and automated medical documentation. The laboratory's proximity to MIT's broader AI research community creates pathways for translating cutting-edge research into deployed applications.³³
Carnegie Mellon University's robotics and AI research programs have produced technologies now being adapted for both military and healthcare applications. The university's Human-Computer Interaction Institute has pioneered research on how humans interact with intelligent systems—critical for designing digital twin interfaces that clinicians and patients can actually use effectively.³⁴
These academic partnerships ensure that military digital twin development draws on the best available science while also contributing back to the broader research community.
Challenges: Data, Privacy, and the Scaling Problem
Despite the promise, significant obstacles remain before digital twin technology can achieve its potential in military and veteran healthcare.
Data Quality and Interoperability. As Dr. Pamplin acknowledged in his Military Medicine commentary, "We lack the intention, and thus the infrastructure" for the kind of massive data collection that would enable sophisticated digital twin models. Military medical data is fragmented across multiple systems—some classified, some not—and civilian healthcare data presents even greater interoperability challenges.³⁵
Privacy and Security. Digital twins require extensive personal data to function effectively. For military personnel, this data could reveal operational capabilities if compromised. For veterans and civilians, health data represents some of the most sensitive personal information imaginable.
Validation and Regulation. As Harvard's I. Glenn Cohen noted, most medical AI is never reviewed by federal regulators. The FDA has issued guidance on computational modeling for medical devices, but comprehensive frameworks for regulating AI-driven personalized medicine models remain under development.³⁶
Equity and Access. Perhaps most significantly, digital twin technology could exacerbate existing healthcare disparities if deployment concentrates in well-resourced academic medical centers while underserved populations lack access. "If the answer is, 'If you can't play in the big leagues, you shouldn't step up to bat,' that creates a have/have-not distribution in terms of healthcare access," Cohen warned.³⁷
The Path Forward: From Research to Reality
Despite these challenges, the convergence of military research, AI capabilities, and healthcare needs creates a realistic path toward digital twin-enabled personalized medicine.
Near-term (2025–2027). The VA's ambient AI scribe deployment will expand to all 170 VA Medical Centers by 2027, creating the foundation for more sophisticated AI applications. The military will continue MASTR-E-derived human performance research through programs at the Army Combat Capabilities Development Command Soldier Center and the Telemedicine and Advanced Technology Research Center.³⁸
Medium-term (2027–2030). Integration of wearable data streams with electronic health records will enable longitudinal tracking that approximates digital twin functionality. Companies like Oura, WHOOP, and Garmin—already collecting continuous physiological data from millions of users—will increasingly partner with healthcare systems to integrate this data into clinical workflows.
Long-term (2030+). True digital twins—personalized models that predict individual health trajectories and optimize interventions in real time—will become feasible for early adopters. Initially expensive and limited to high-risk or high-performance populations, these systems will gradually become more accessible as AI costs decline and infrastructure matures. TwinHealth, which uses AI-driven digital twin technology for metabolic disease management, has demonstrated that personalized models can drive meaningful clinical outcomes—a randomized controlled trial showed their approach achieved type 2 diabetes remission rates significantly exceeding standard of care.
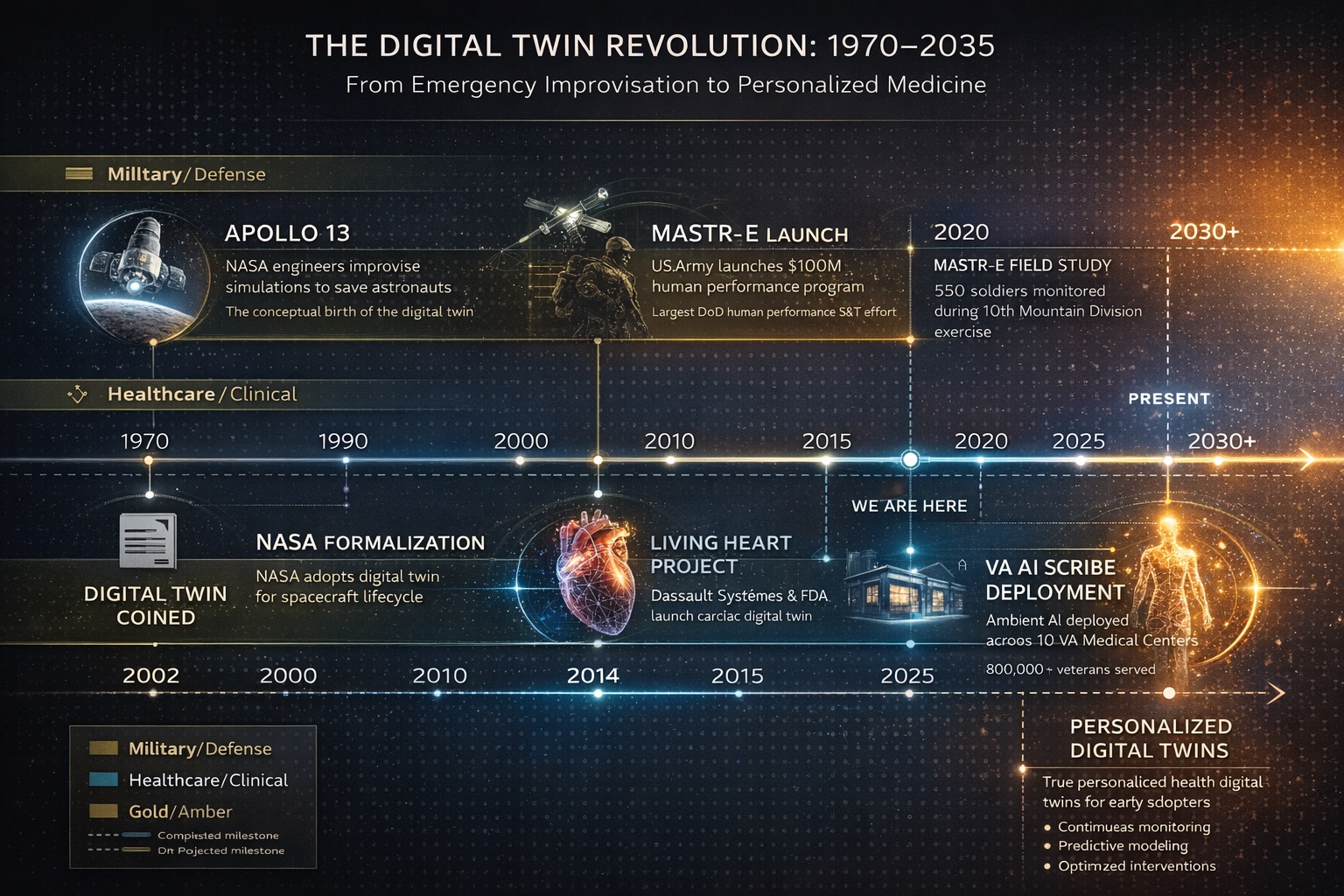
From emergency improvisation during Apollo 13 to the VA's 2025 AI deployment, digital twin technology has evolved from concept to clinical reality over five decades—with true personalized health optimization projected to reach early adopters by 2030 and broader populations thereafter.
Implications for Longevity Planning
For individuals serious about extending their healthspan—the years of healthy, active life rather than mere survival—the digital twin revolution offers both immediate opportunities and a framework for future optimization.
Embrace data collection now. The foundation of any digital twin is longitudinal data. Individuals who begin systematic tracking of biomarkers, activity patterns, sleep quality, and other health indicators today will have years of baseline data when more sophisticated analysis tools become available.
Prioritize cardiorespiratory fitness. The military's focus on cardiorespiratory capacity reflects overwhelming evidence that aerobic fitness is the most modifiable predictor of longevity. While a true Cardiorespiratory Digital Twin™ may be years away, individuals can approximate its benefits by conducting regular VO2 max testing, training across multiple intensity zones, and tracking recovery patterns over time.
Plan for personalization. Generic health advice—eat less, exercise more, sleep better—has limited utility precisely because individuals vary so dramatically in their physiological responses. As personalized models become available, those who have invested in understanding their own patterns will be better positioned to benefit.
Conclusion: The Digital Twin Dividend
In a May 2025 article in the Special Warfare Journal, Col. Paul O. Kwon and his colleagues made a prediction: "Humanoid digital twin technology provides a solution to deliver personalized and dynamic training at a scale that ensures a ready medical force to improve the survivability and lethality of the Soldier."
The same technology that improves soldier survivability and lethality can improve civilian healthspan and longevity. The same data infrastructure that enables casualty digital twins can enable patient digital twins. The same AI capabilities that optimize military training can optimize personal health interventions.
What began as a NASA emergency improvisation during Apollo 13 has evolved into a comprehensive framework for understanding, predicting, and optimizing human health and performance. The future of longevity isn't found in a single supplement, a miracle diet, or a revolutionary exercise program. It's found in the comprehensive understanding of individual physiology that digital twin technology enables—the ability to model your unique system, predict your specific responses, and optimize your personal path to extended healthspan.
The soldiers at Fort Devens, monitored by seventeen sensors as they prepare for their next mission, are the early adopters of this future. The question for the rest of us is whether we're ready to follow.